REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
CLINICAL
INFORMATION
Neuraxial
anesthesia
after
local
anesthesia
for
management
of
percutaneous
vertebroplasty
complication
during
vertebroplasty
Hüseyin
Balkarlı
a,
Mesut
Kılıc
¸
b, ˙Ibrahim
Öztürk
c,∗aAkdenizUniversityFacultyofMedicine,OrthopaedicsandTraumatology,Antalya,Turkey bOndokuzmayısUniversityFacultyofMedicine,OrthopaedicsandTraumatology,Samsun,Turkey
cDıs¸kapıYıldırımBeyazıtEducationandResearchHospital,AnesthesiologyandReanimation,Ankara,Turkey
Received9June2014;accepted16July2014 Availableonline27October2014
KEYWORDS
Neuraxialanesthesia; Percutaneous vertebroplasty; Vertebra; Fracture
Abstract Percutaneousvertebroplastyisarelativelysafe,simpleandcommonlyperformed interventional procedurefor themanagementofvertebral compressionfractures. However, seriouscomplicationsarerarely reportedintheprocedure.Thosearepulmonaryembolism, severeinfection,paraplegiaandanoccurrenceofanewfractureinanadjacentvertebraafter vertebroplasty.Acutecomplicationsaregenerallyassociatedwiththeprocedure.Wepresent thecaseofneuraxialanesthesia,developedafterlocalanesthesiawith8mLof2%prilocaine, in a68-year-old woman who underwent percutaneous vertebroplastyafter anosteoporotic collapsedfractureintheL1vertebraduetotrauma.Toourknowledge,thisisthefirstcasein
theliterature.
©2014SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE Bloqueioneuraxial; Vertebroplastia percutânea; Vértebra; Fratura
Bloqueioneuroaxialapósanestesialocalparamanejodecomplicac¸ão
devertebroplastiapercutâneadurantevertebroplastia
Resumo Vertebroplastia percutânea é um procedimento intervencionista relativamente seguro, simples e comumente realizado para tratar fraturas por compressão vertebral. No entanto, as complicac¸ões graves relacionadas ao procedimento são raramente relatadas, incluindoembolia pulmonar,infecc¸ãograve,paraplegiaeaocorrênciadeuma novafratura emvértebraadjacenteapósavertebroplastia.Complicac¸õesagudassãogeralmenteassociadas aoprocedimento.Apresentamosocasodebloqueioneuroaxial,realizadoapósanestesialocal
∗Correspondingauthor.
E-mail:[email protected](˙I.Öztürk).
http://dx.doi.org/10.1016/j.bjane.2014.07.007
0104-0014/©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC
206 H.Balkarlıetal.
com8mLdeprilocaínaa2%,emumamulherde68anosdeidade,submetidaàvertebroplastia percutâneaapósfraturaosteoporóticanavértebraL1devidoatrauma.Deacordocomnossa
pesquisa,esteéoprimeirocasonaliteratura.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Percutaneous vertebroplasty (PV) is a relatively safe, simple,and commonly performedprocedure for the man-agement of vertebral compression fractures, but serious complications have been reported, including pulmonary embolism,1 severe infection,2 paraplegia3 and an
occur-rence of a new fracture in an adjacent vertebra after vertebroplasty.4Acutecomplicationsaremostlyrelatedto
surgicalprocedures,whichincludeleakageofbonecement, infection,andfracturealongthepathofthevertebroplasty cannula.5,6
We present a rare case of neuraxial anesthesia corre-latedwith localanesthesiaduring a surgical PV usingthe transpedicularapproach.
Case
report
A68-year-oldand75kgweighingfemalepatientwas admit-ted to the Emergency Department of Tavas Community Hospitalwithbackpainduetotraumafollowingfallingdown athome.Thepatienthadanosteoporoticcollapsedfracture intheL1 vertebra,which wastreated conservativelywith
bedrest,corsetandanalgesicmedications.Atthe3rdweek follow-up examination, pain had not reduced and onthe directradiographmorethan50%ofthefracturedL1
verte-brawasobservedtohavecollapsedcomparedtotheupper adjacent vertebra(Fig. 1). PV was recommended for the patient.
At the preoperative evaluation of patient, laboratory tests, electrocardiogram and X-ray of lung were normal. Therewasnochronicsystemicdisease.Andherphysical sta-tuswasevaluatedaslevel1accordingtoAmericanSociety ofAnesthesiologist’sscale.Thepreoperativevisualanalogue painscalescore(VAS)was8.Afterobtaininginformed con-sent, patient’s fracture line waslocated with fluoroscopy inpronepositionandthenunderfluoroscopiccontrol,local anesthesiaof 8mL of 2% prilocaine wasapplied fromthe pedicleentranceasfarasthesubcutaneoustissue.No neu-rologicaldeficitwasdeterminedfollowinglocalanesthesia. Afterlocationofthepedicleentranceofthefractured ver-tebraunderfluoroscopy, an11G needlewasentered from thepedicle.Whentheneedlereached2/3anteriorofthe vertebralcorpusonthelateralview,theanterior---posterior viewwasregarded and thatthe tipof the needle wasat thesamelevelasthespinousprocess.Theneedleposition wascheckedbyfluoroscopy.Atthisstage,theneurological examinationofthepatientwasnormal.Afterconfirmation
oftheneedletiplocation,8mLofcementwasinjectedinto thefractureline(Fig.2).
During and following the cementing, the neurological examinationofthepatientwasnormal.Aftersettingofthe cement,thepatientwasplacedinasupineposition. Imme-diatelyafterthepatientwaspositionedsupine,abilateral lowerextremitylossofstrength(2/5)andsensationdeficit occurred.Itwasnoticedbytheoperatorduringneurological examination.Bloodpressurewasmeasuredas90/50mmHg and500mLof0.9%NaClwasadministered.Asthesensation loss,atT10levelatfirstexamination,reacheduptoT5.The
patientwasmovedintothebeach-chairpositiontoprevent furtherdevelopmentofneuraxialblock.
The patient was again evaluated neurologically, and bilateral loss of strength (0/5) in the lower extremities and anesthesia were observed. 6mg betamethasone was administered intramuscularly. The patient was evaluated with direct radiographs at operating theater and cement wasnotobserved incanal (Fig.3). 30min aftertheonset of the sensation deficit, blood pressure was measured as 110/90mmHgandthedeficithadreturnedtothelevelofthe umbilicus.
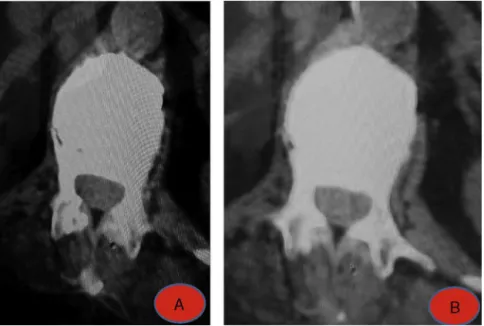
On evaluation of patient by computer tomography, no cement was observed in canal (Fig. 4). At the 4th hour of follow-up sensation and motor deficit was completely resolved. The patient wasmobilized. We didnot observe hypotension or bradycardia and no inotropic drug was needed.
Discussion
Vertebroplastyhasbeenwidelyusedtotreatvertebralbody compression fractures (VCFs) caused by varied patholo-gies includinghemangioma, multiple myeloma, osteolytic metastases,and primaryorsecondary osteoporosis.7VCFs
arethemostcommontypeofosteoporoticfractures, result-ingin severeback pain,spinaldeformity,muscleatrophy, prolonged hospitalization, and potential risk of increased mortality.8
Inmeta-analysisofPV,lowcomplicationrateof0.4---3.8% hasbeenreported.9OverallcomplicationratesduetoPVare
Figure1 (A)AcuteL1fracture.(B)After3weeksconservativetreatment.
Inliterature,nopatienthasbeenreportedwith neurax-ialanesthesiadevelopmentassociatedwithlocalanesthesia during PV. The significance of this is that a neurological injuryassociatedwiththeguideusedduringtheprocedure maybeconfusedwithneurologicalinjurywhichmayoccur after leakage of the cement into thecanal and a second operationsuchasopensurgeryisrequired.Differential diag-nosisshouldcertainlybemadefortheseabove-mentioned
complications which may arise following PV and other neurologicalinjurieswhichoccurduringPV.Ifthereare neu-rologicaldeficits which occur during PV and this event is consideredtobeassociatedwithlocalanesthetic,thelevel ofneuraxialanesthesiamaybeincreasedandcomplications associatedwiththeincreasedlevelshouldbekeptinmind, thepatientshouldbecloselymonitored,andanesthesia spe-cialistmustcertainlyconsultthepatient.
208 H.Balkarlıetal.
Figure3 (A)PostoperativeX-ray(AP).(B)PostoperativeX-ray(lateral).
Figure4 (AandB)PostoperativeCT.
Conclusion
Inourknowledge,thisisthefirstneuraxialanesthesiacase duetolocalanesthesiaafterPV intheliterature.Ifthere isnocementintothecanal,neuraxialanesthesiashouldbe keptinmind.Atthispoint,radiopaqueagentmaybeuseful beforeinjectionoflocalanestheticdrugforconfirmingthe placeof needle’stip,topreventan inadvertentneuraxial anesthesia.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.ChenHL,WongCS,HoST,etal.Alethalpulmonary embolism during percutaneous vertebroplasty. Anesth Analg. 2002;95: 1060---2.
2.Lin WC, Lee CH, Chen SH, et al. Unusual presentation of infected vertebroplasty with delayed cement dislodgment in an immunocompromised patient: case report and review of literature. Cardiovasc Intervent Radiol. 2008;31 (Suppl. 2): 231---5.
3.LeeBJ, Lee SR,Yoo TY. Paraplegia asa complication of per-cutaneousvertebroplastywithpolymethylmethacrylate:acase report.Spine(PhilaPa1976).2002;27:E419---22.
loadingdirectionafterawedgefracture.Spine(PhilaPa1976). 2011;36:E408---12.
5.McArthurN,KasperkC,BaierM,etal.1150kyphoplastiesover7 years:indications,techniques,andintraoperativecomplications. Orthopedics.2009;32:90.
6.Tanigawa N,KariyaS,KomemushiA, etal.Cement leakagein percutaneousvertebroplastyforosteoporoticcompression frac-tureswithorwithoutintravertebralclefts.AJRAmJRoentgenol. 2009;193:W442---5.
7.Afzal S, Dhar S, Vasavada NB, et al. Percutaneous verte-broplasty for osteoporotic fractures. Pain Physician. 2007;10: 559---63.
8.ShiMM,CaiXZ,LinT,etal.Istherereallynobenefitof verte-broplastyforosteoporoticvertebralfractures?Ameta-analysis. ClinOrthopRelatRes.2012;470:2785---99.