REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Comparison
of
the
postoperative
analgesic
effects
of
naproxen
sodium
and
naproxen
sodium-codeine
phosphate
for
arthroscopic
meniscus
surgery
夽
Cagla
Bali
∗,
Pinar
Ergenoglu,
Ozlem
Ozmete,
Sule
Akin,
Nesrin
Bozdogan
Ozyilkan,
Oya
Yalcin
Cok,
Anis
Aribogan
BaskentUniversitySchoolofMedicine,AnesthesiologyandReanimationDepartment,Adana,Turkey
Received4July2014;accepted7August2014 Availableonline27November2014
KEYWORDS
Arthroscopy; Postoperative analgesia; Naproxensodium; Codeinephosphate
Abstract
Backgroundandobjectives: Nonsteroidalanti-inflammatorydrugs(NSAIDs)arefrequentlyused
tocontrolarthroscopicpain.Additionoforaleffectiveopioid‘‘codeine’’toNSAIDsmaybemore effectiveanddecreaseparenteralopioidconsumptioninthepostoperativeperiod.Theaimof thisstudywastocomparetheefficacyandsideeffectsofnaproxensodiumandanew prepa-rationnaproxensodium-codeinephosphatewhenadministeredpreemptivelyforarthroscopic meniscectomy.
Methods:Sixty-onepatientswererandomizedintotwogroupstoreceiveeitheroralnaproxen
sodium(GroupN)ornaproxensodium-codeinephosphate(GroupNC)beforesurgery.Thesurgery was carried outundergeneralanesthesia.Intravenous meperidinewasinitiatedby patient-controlled analgesia(PCA)forallpatients.Theprimaryoutcomemeasurewaspain scoreat thefirstpostoperativehourassessedbytheVisualAnalogueScale(VAS).Sedationassessedby RamseySedationScale,firstdemandtimeofPCA,postoperativemeperidineconsumption,side effectsandhemodynamicdatawerealsorecorded.
Results:The groups weredemographically comparable.Median VASscores bothatrest and
onmovementweresignificantlylowerinGroupNCcomparedwithGroupN,except18th hour
onmovement(p<0.05).ThemediantimetothefirstdemandofPCAwasshorterinGroupN comparedwithGroupNC(p<0.001).MeperidineconsumptionwashigherinGroupNcompared withGroupNC(p<0.001).Therewasnodifferencebetweengroupswithrespecttosideeffects (p>0.05).
Conclusions: Thecombinationofnaproxensodium-codeinephosphateprovidedmoreeffective
analgesiathannaproxensodiumanddidnotincreasesideeffects.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
夽 ThisstudywascarriedoutinBaskentUniversity,FacultyofMedicine,DepartmentofAnesthesiologyandReanimation,Adana,Turkey.
∗Correspondingauthor.
E-mail:[email protected](C.Bali).
http://dx.doi.org/10.1016/j.bjane.2014.08.006
PALAVRAS-CHAVE
Artroscopia; Analgesia pós-operatória; Naproxenosódico; Fosfatodecodeína
Comparac¸ãodosefeitosanalgésicospós-operatóriosdenaproxenosódico
enaproxenosódico-fosfatodecodeínaemartroscopiademenisco
Resumo
Justificativaeobjetivos: Osanti-inflamatóriosnãoesteróides(AINEs)sãofrequentemente
usa-dosparacontrolaradorapósartroscopia.Aadic¸ãodeumopiáceooraleficaz(codeína)aosAINEs podesermaisefetivaediminuiroconsumodeopiáceoparenteralnopós-operatório.Oobjetivo desteestudofoicompararaeficáciaeosefeitoscolateraisdenaproxenosódicoeumanova preparac¸ão,naproxenosódico-fosfatodecodeína,quandoadministradospreventivamentepara meniscectomiaartroscópica.
Métodos: Sessentaeumpacientesforamrandomicamentedivididosemdoisgrupospara
rece-bernaproxenosódicoporviaoral(GrupoN)ounaproxeno sódico-fosfatodecodeína(Grupo NC)antesdacirurgia.Acirurgiafoirealizadasobanestesiageral.Meperidinaintravenosafoi iniciadapormeiodeanalgesiacontroladapelopaciente(ACP)paratodosospacientes.O des-fechoprimáriofoioescorededornaprimeirahoradepós-operatório,avaliadacomaEscala VisualAnalógica(EVA).Asedac¸ãofoiavaliadausandoaEscaladeSedac¸ãodeRamsey.Aprimeira demandadeACP,oconsumodemeperidinanopós-operatório,osefeitoscolateraiseosdados hemodinâmicostambémforamregistrados.
Resultados: Osgrupos foram demograficamentecomparáveis. Asmedianas dos escores EVA
tantoemrepousoquantoemmovimentoforamsignificativamentemenoresnoGrupoNC com-paradoaoGrupoN;excetoparamovimentonaavaliac¸ãode18horas(p<0,05).Amedianado tempoatéaprimeirademandadeACPfoimenornoGrupoNemcomparac¸ãocomoGrupoNC (p<0,001).OconsumodemeperidinafoimaiornoGrupoNemcomparac¸ãocomoGrupoNC (p<0,001).Nãohouvediferenc¸aentreosgruposemrelac¸ãoaosefeitoscolaterais(p>0,05).
Conclusões:A combinac¸ãode naproxeno sódico-fosfato decodeína forneceu analgesiamais
efetivaquenaproxenosódico,semaumentarosefeitoscolaterais.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Arthroscopic knee surgery is a common surgical inter-vention. There is evidence that effective postoperative pain management facilitates discharge and more rapid functionalimprovement of these patients.1,2 Nonsteroidal anti-inflammatory drugs (NSAIDs) are frequently used for controllingarthroscopicpain1,2andhavebeenadministered alone or as intraarticular combinations with local anes-thetics or opioids for these procedures.2,3 This group of drugshavebeen demonstratedtoreducepainand inflam-mationduetoarthroscopy,aswell aseffusionsrelatedto inflammation, by inhibiting prostaglandin synthesis.4 The preoperativeadministrationofNSAIDs maybemore effec-tiveinreducingpostoperativepainbyinhibitingprostanoid productionbeforethedevelopmentoftissueinjury.1
Althoughtheefficacyoforalnaproxensodiumasa pre-emptivemedicationhasbeenshownfor arthroscopicknee surgery,5thepreemptiveefficacyoforalnaproxen sodium-codeine phosphate has not yet been investigated to our knowledge.Codeineisaprodrugwithwell-knownanalgesic efficacy,anditisfrequentlyusedinpainmanagement.Itis metabolizedtoitsactiveform,morphine,bytheliver.6
This study aims to compare the efficacy of single preemptive dose of oral naproxen sodium versus a new combinationoforalnaproxensodium-codeinephosphateon postoperativepaininadultpatientsundergoingarthroscopic meniscectomy.
Materials
and
methods
TheBaskentUniversityInstitutionalReviewBoardandEthics Committeeapprovedthisprospective,randomized, double-blind study (Project number: KA12/268). The study was supported by Baskent University Research Fund and was completed within 6 months. Patients undergoing arthro-scopic meniscectomy were included in the study. The exclusioncriteriawereasfollows:≤18yearsofage, hyper-sensitivity to NSAIDs and/or codeine, history of a peptic ulcer,gastritis,uppergastrointestinalbleeding,a coagula-tiondisorder,hepaticfailure,renalimpairment,pregnancy, andtheuseofNSAID,opioidandotheranalgesicagentsup tothetimeofthesurgery.
During the preoperative examination, patients were informedabout thestudyparameters,includingpain man-agementmethodstobeusedduringthestudy,drugsinvolved and potential side effects. Written informed consentwas obtainedfromallpatients.
Enrollment
Assessed for eligibility (n=62)
Lost to follow-up (n=0)
Discontinued Naproxen sodium (n=0)
Lost to follow-up (n=0) Discontinued Naproxen sodium codeine phosphate (n=0) Randomized (n=61)
Allocation
Follow-up
Analysis Analysed (n=30)
♦Excluded from analysis (n=0)
Analysed (n=31)
♦Excluded from analysis (n=0)
Excluded (n=1)
♦Not meeting inclusion criteria (n=1) ♦Declined to participate (n=0) ♦Other reasons (n=0)
Allocated to group NC (n=31)
♦Received Naproxen sodium-codeine
phosphate (n=31)
♦Did not receive Naproxen sodium-codeine
phosphate (n=0) Allocated to group N (n=30)
♦Received Naproxen sodium (n=30) ♦Did not receive Naproxen sodium (n=0)
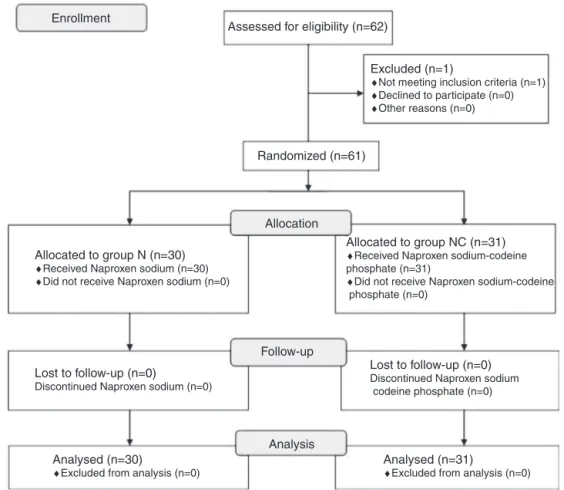
Figure1 Studyflowchart.GroupN,naproxensodiumgroup;GroupNC,naproxensodium-codeinephosphategroup.
GroupNC(n=31)receivednaproxensodium-codeine phos-phate550mg+30mgtablets (ApranaxPlus®, AbdiIbrahim
Ilac,Istanbul/Turkey)(Fig.1).
Followingtransfertotheoperatingroom,patientswere monitoredbypulse-oximetry,electrocardiographyand non-invasive blood pressure. Induction and maintenance of anesthesiawereperformed byan anesthesiologist blinded tothe study.Intravenous propofol (2mg/kg) and fentanyl (0.5g/kg)wereusedforinductionandintravenous
rocuro-niumwasusedasamusclerelaxant(0.6mg/kg).Following endotracheal intubation, anesthesia was maintained with isoflurane(1---1.5%)andamixtureofnitrousoxideand oxy-gen(50%+50%).Attheendoftheoperation,neuromuscular blockadewasreversed withneostigmine (0.05mg/kg) and atropine(0.015mg/kg).Patientswerethenextubated and transferredtotherecoveryroom.
In the recovery room,intravenous meperidine was ini-tiated by patient-controlled analgesia (PCA; 10mg bolus, 20min lockout, no basal infusion and 4h limit) for all patients.
Datawererecordedbyananesthesiatechnicianblinded to the study drugs. Postoperative pain levelsat rest and on movement were evaluated using the Visual Analogue Scale(VAS;0=nopainand10=theworstpainpossible)and recorded at 15 and 30min and at 1, 2, 4,6, 12 and 18h postoperatively.
Sedation scores were assessed usingthe Ramsey Seda-tionScale(1:anxiousandagitated;2:cooperative,oriented and calm;3: drowsy, responsive toorders; 4:asleep,but
responsivetoaglabellartap;5:sleepingandslowly respon-sivetotactilestimuli;and6:patientunresponsivetopainful stimuli)andwererecordedatthesametimepoints.
Hemodynamicdata (systolic, diastolicand mean blood pressure;heartrate)andperipheraloxygensaturationwere recorded before anesthesiaand at 5, 10, 15, 30, 45 and 60minfollowinganestheticinduction;beforeandafterthe surgicalincision;andat15and30minand1,2,4,6,12and 18hpostoperatively.
TimetothefirstdemandofPCA,totalmeperidine con-sumption,andpostoperativesideeffectssuchassedation, respiratorydepression,constipation,urinaryretention, nau-sea, vomiting, gastric complaints and bleeding in the surgicalareawererecorded.
Statistical
analysis
The primary outcome parameter of this study was visual analogscoreforpainatthefirstpostoperativehour.Power analysisofthestudywasbasedonastudybyCodeetal.5 Win-Epi2.0wasusedforsamplesizecalculation;atotalof 60patientswith30patientsineachgroupwasconsideredto beanappropriatenumberfollowingsamplesizecalculation fora95%confidenceintervalandpowerof80%.
Table1 Demographiccharacteristics.
GroupN GroupNC Mean±SD(n=30) Mean±SD(n=31) Age(years) 39.70±13.21 42.03±13.66 Weight(kg) 77.26±12.84 78.35±12.95 Height(cm) 171.13±10.77 169.41±10.03 Sex
(female/male)
15/15 16/15 ASA(I-II) 17/13 15/16 Durationof
surgery(min)
33.43±7.19 30.61±6.08
GroupN,naproxensodiumgroup;GroupNC,naproxen sodium-codeinephosphate group;Datashowthenumberofcases or mean±SD,mean±standarddeviation;ASA, AmericanSociety ofAnesthesiologists;min,minute.
standarddeviation(andasmedianandminimum---maximum whennecessary). Theintergroup comparisonofnumerical variables was performed using Student’s t-test when the assumptions were fulfilled and the Mann---Whitney U test when the assumptions were not fulfilled. For parameters withnormal distribution, repeatedmeasures analysisand thepaired t-test wereused tocomparedependent varia-bleswhereastheWilcoxontestortheFriedmantestswere otherwise used. p-Values less than 0.05 were considered significantforallcomparisons.
Results
Sixty-two patients were invited to participate. During screening,onepatientwasfoundtonotmeettheinclusion criteria, so sixty-one patients were enrolled in the study (Fig.1).Thegroupshadcomparabledemographics, includ-ingage,bodyweight,height,gender,ASA(AmericanSociety ofAnesthesiologists)statusandsurgerytime(Table1).
Therewerenosignificant differencesregardingsystolic anddiastolicbloodpressure,heartrateandperipheral oxy-gensaturationvaluesbetweengroups.Noneofthepatients exhibitedhypotension,hypertension,bradycardiaor tachy-cardia.
Median VAS scores at rest were significantly lower in GroupNCcomparedwithGroupNatallmeasured postopera-tivetimepoints(15minthrough18h)(Table2).MedianVAS
Table2 VisualAnaloguepainscoresatrest. Postoperative GroupN GroupNC p
Times Median (min---max)
Median (min---max)
15min 3(0---4) 1(0---3) 0.0001 30min 3(0---4) 1(0---3) 0.0001 1h 3(0---4) 2(1---3) 0.0001 2h 3(0---4) 2(0---3) 0.001 4h 2(1---4) 2(0---3) 0.0001 6h 2(0---4) 1(0---6) 0.0001 12h 2(0---3) 1(0---3) 0.0001 18h 2(0---3) 1(0---2) 0.0001
GroupN,naproxensodiumgroup;GroupNC,naproxen sodium-codeinephosphategroup;min---max,minimum---maximum.
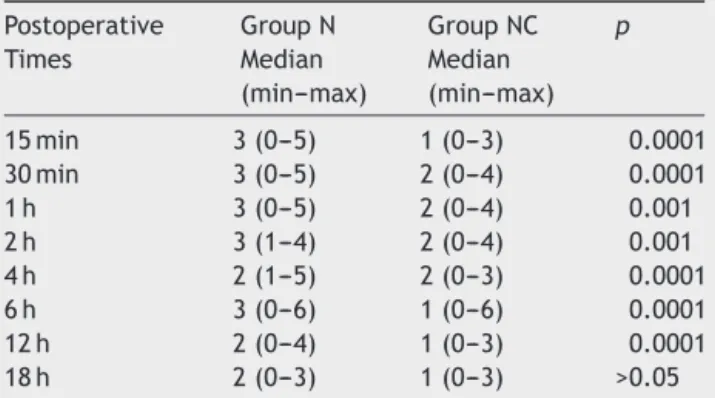
Table3 VisualAnaloguepainscoresonmovement. Postoperative GroupN GroupNC p
Times Median (min---max)
Median (min---max)
15min 3(0---5) 1(0---3) 0.0001 30min 3(0---5) 2(0---4) 0.0001 1h 3(0---5) 2(0---4) 0.001 2h 3(1---4) 2(0---4) 0.001 4h 2(1---5) 2(0---3) 0.0001 6h 3(0---6) 1(0---6) 0.0001 12h 2(0---4) 1(0---3) 0.0001 18h 2(0---3) 1(0---3) >0.05
GroupN,naproxensodiumgroup;GroupNC,naproxen sodium-codeinephosphategroup;min---max;minimum---maximum.
scoresonmovementwerealsosignificantlylowerinGroup NCcompared withGroupN exceptfor the scoreat 18thh postoperatively(Table3).
The mediantimetopatients’ firstdemand ofPCA was 29mininGroupN(10---240min)versus135min(20---600min) in Group NC; this timeperiodwas significantly shorter in Group N (p<0.001). Consumption of intravenous meperi-dineduringthe18hpostoperativelywas20mginGroupNC (10---50mg)versus95mg(10---160mg)inGroupN(p<0.001). Bothgroups hadsimilar sedationscores; the incidence ofnauseaandvomitingdidnotsignificantlydifferbetween groups(p>0.05).Bleedinginthesurgicalarea,gastric com-plaints, respiratory depression, constipation, and urinary retentionwerenotobservedinanypatientsineithergroup.
Discussion
In this study, we evaluated the efficacy of preemptive naproxensodiumandnaproxensodium-codeinephosphate in patients who underwent arthroscopic meniscectomy. We have demonstrated thatpreemptive administration of naproxen sodium-codeine phosphate significantly reduced postoperativeopioidconsumptionandprovidedmore effec-tiveanalgesiacomparedwithnaproxensodiumalone.
NSAIDsarecommonlyadministeredforarthroscopic pro-cedures.Faster recovery,more rapidreturn ofmovement and quadriceps function, and more quick return to work werereportedwhenNSAIDswereadministeredfor arthro-scopicsurgeries.4,7NSAIDssuppresstheacuteinflammatory responsebyblocking prostaglandinsynthesis viainhibition oftheenzymecyclooxygenase.8NSAIDsmayreduce periph-eralnociceptionbyreductionoftheinflammatoryresponse tosurgicaltrauma,8andtheymayalsomodulatethecentral responsetopainfulstimulibyinhibitingprostaglandin syn-thesisin thespinalcord.9Analgesic efficacyof NSAIDsfor postoperativepainhasbeen investigatedinmany studies, andtheir analgesicefficacy isconsidered tobeashighas thatofopioids.10---13
pain andanalgesic requirements evenafter the analgesic effectsof thepreemptive agentshave wornoff.14 Studies haveshownthatthepreemptiveadministrationofnaproxen sodium provides improved postoperative pain control, a reductioninanalgesicusage,orboth.5,15---17
Although the preemptive administration of naproxen sodium has been studied, there are no other studies on thepreemptiveefficacyofthenaproxen-codeine combina-tionsincethis preparationisa newagentonthe market. Codeine,a prodrug withwell-known analgesic efficacy, is frequently usedin pain management in combination with parasetamol.18 For this reason, we compared naproxen sodiumandnaproxensodium-codeinephosphateinpatients undergoing arthroscopic meniscectomy. In our study, VAS scoresweresignificantlylowerinGroupNCcomparedwith Group N, and meperidine consumption was significantly higherinGroupN.
The analgesicefficacyofnaproxen-codeinemaybedue to the prevention of sensitization in peripheral and cen-tral pathways before tissueinjury. The higher efficacy of naproxen-codeinerelativetonaproxensodiummaybedue tothewell-knownanalgesicefficacyofcodeine.The effec-tive dose of codeine phosphate is 30---60mg, with higher doses opioid-related side effects become visible, consti-pation, nausea, and respiratory depression.18 A previous reviewthatincludesdatafrom14clinicaltrialsshowedthat thecombinationofparacetamol(600---1000mg)andcodeine (30---60mg) provided effective analgesia in approximately 50%ofpatientswithmoderatetoseverepostoperativepain andthatthiscombination prolongeddurationof analgesia comparedwithpatients receiving paracetamolalone.19 In another review, which included 35 clinical trials compar-ingcodeine(60---90mg)withplaceboinpostoperativepain management,singleagentcodeineat60mgprovided bet-teranalgesiathanplacebo.However,thisanalgesiawasnot sufficient whena comparison wasmade betweencodeine alone and its use in combination with paracetamol and NSAIDs.20 Similarly, ourstudyshowedmoreeffective post-operativeanalgesiaandlowermeperidineconsumptionwith the naproxen sodium-codeine phosphate combination. In previousstudies,codeineandotherdrugswereadministered asdifferentpillstopatients,whereasourstudyusedsingle pillsthatincludedbothnaproxensodiumandcodeine.This maybeanadvantageforpatients,asitcontributestousage facility.Inboth meta-analyses,opioid-relatedside effects suchasdrowsinessandsomnolenceweremorefrequentin the groups receiving codeine, although this was not sta-tistically significant.19,20 Forbes etal. comparednaproxen sodium,codeinesulfate,naproxensodiumandcodeine sul-fate for postoperative pain after oral surgery.21 In this papercodeinedosewas60mgingroups receivingcodeine which was twice the dose of our study. Accordingly they reported more side effects with codeine. Although our study was not powered to show any difference between the groups regarding side effects, we may roughly state thatsideeffectssuchassedation,drowsiness,nauseaand vomiting were similar between the groups. This may be interpretedthatthedosingofcodeineinthiscommercially availablepreparationwastolerablebythepatientsofthis study.
Codeine is metabolized in the liver to its active form morphine by the cytochrome P-450 isoenzyme 2D6
(CYP2D6).22,23CYP2D6ishighlypolymorphic.These polymor-phismscreatedifferentphenotypesforcodeinemetabolism, from ultra-rapid metabolism to poor metabolism. Ultra-rapid metabolism maycause high levelsof morphine and toxicity.22Seriousadverseeventsanddeathswerereported in children with obstructive sleep apnea (13 cases in an estimated >22 million pediatric tonsillectomies) who receivedcodeine aftera tonsillectomy and/or adenoidec-tomy.Sincethesechildrenhadalreadyunderlyingbreathing problemsand alsosome of them wereultra-rapid metab-olizer,the U.S Food and DrugAdministration (FDA) warns aboutcodeinuseinallchildrenaftertonsillectomyand/or adenoidectomy.22,23 But there is nowarning about codein useinadults.
Although the beneficial effects of NSAIDs have been demonstrated, there are some concerns about negative effects, such as gastrointestinal mucosal damage, renal tubulardamageandplateletdysfunction.24,25 Inourstudy, nosuchproblemsoccurredrelatedtoNSAIDuse.
Conclusions
Preemptiveoral naproxensodium-codeinephosphateis an effective analgesic option in patients undergoing arthro-scopic meniscectomy when compared with oral naproxen sodium,anditcarriestheadvantagesofeaseof administra-tionandlackofserioussideeffectsatthisdose.Wesuggest thatnaproxensodium-codeinephosphatemaybeavaluable optionforclinicaluseforarthroscopicprocedures.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
This study was supported by Baskent University Research Fund(Projectnumber:KA12/268).
References
1.ReubenSS,BhopatkarS,MaciolekH,etal.Thepreemptive anal-gesiceffectofrofecoxib afterambulatoryarthroscopic knee surgery.AnesthAnalg.2002;94:55---9.
2.Menigaux C, Guignard B, Fletcher D, et al. Intraoperative small-doseketamineenhancesanalgesiaafteroutpatientknee arthroscopy.AnesthAnalg.2001;93:606---12.
3.HosseiniH,AbrishamSMJ,JomehH,etal.Thecomparisonof intraarticularmorphine-bupivacaineandtramadol-bupivacaine inpostoperativeanalgesiaafterarthroscopicanteriorcruciate ligamentreconstruction.KneeSurgSportsTraumatolArthrosc. 2012;20:1839---44.
4.Ogilvie-HarrisDJ,BauerM,CoreyP.Prostaglandininhibitionand therateofrecovery afterarthroscopicmeniscectomy.A ran-domiseddouble-blindprospectivestudy.JBoneJointSurgBr. 1985;67:567---71.
5.Code WE,Yip RW,Rooney ME, et al. Preoperative naproxen sodiumreducespostoperativepainfollowingarthroscopicknee surgery.CanJAnaesth.1994;41:98---101.
of pain of different origin. Eur Rev Med Pharmacol Sci. 2013;17:2129---35.
7.PedersenP,NielsenKD,JensenPE.TheefficacyofNa-naproxen afterdiagnosticandtherapeuticarthroscopyofthekneejoint. Arthroscopy.1993;9:170---3.
8.White PF.Therole ofnon-opioidanalgesictechniquesinthe managementofpainafterambulatorysurgery.AnesthAnalg. 2002;94:577---85.
9.MøinicheS,KehletH,DahlJB.Aqualitativeand quantitative systematic reviewofpreemptive analgesia for postoperative pain relief: the role of timing of analgesia. Anesthesiology. 2002;96:725---41.
10.Brown CR,MazzullaJP, MokMS,etal.Comparison ofrepeat dosesofintramuscularketorolactromethamineandmorphine sulfate for analgesia after major surgery. Pharmacotherapy. 1990;10:45S---50S.
11.O’HaraDA,FragenRJ,KinzerM,etal.Ketorolactromethamine ascomparedwithmorphinesulfatefortreatmentof postopera-tivepain.ClinPharmacolTher.1987;41:556---61.
12.PowellH,SmallmanJM,MorganM.Comparisonof intramuscu-lar ketorolacand morphineinpaincontrolafterlaparotomy. Anaesthesia.1990;45:538---42.
13.SammourRN,OhelG,CohenM,etal.Oralnaproxenversusoral tramadolforanalgesiaaftercesareandelivery.IntJGynaecol Obstet.2011;113:144---7.
14.Katz J. Pre-emptive analgesia: importance of timing. Can J Anaesth.2001;48:105---14.
15.vanEER,HemrikaDJ,vanderLindenCT.Painrelieffollowing day-casediagnostichysteroscopy---laparoscopyforinfertility:a double-blindrandomizedtrialwithpreoperativenaproxen ver-susplacebo.ObstetGynecol.1993;82:951---4.
16.DunnTJ,ClarkVA,JonesG.Preoperativeoralnaproxenforpain reliefafterday-caselaparoscopicsterilization.BrJAnaesth. 1995;75:12---4.
17.ComfortVK, CodeWE,Rooney ME,etal.Naproxen premedi-cationreducespostoperativetuballigationpain.CanJAnaesth. 1992;39:349---52.
18.VreeTB,vanDongenRT,Koopman-KimenaiPM.Codeine anal-gesiaisduetocodeine-6-glucuronide,notmorphine.IntJClin Pract.2000;54:395---8.
19.TomsL,DerryS,MooreRA,etal.Singledoseoralparacetamol (acetaminophen)withcodeineforpostoperativepaininadults. CochraneDatabaseSystRev.2009:CD001547.
20.DerryS,MooreRA,McQuayHJ.Singledoseoralcodeine,asa singleagent,foracutepostoperativepaininadults.Cochrane DatabaseSystRev.2010:CD008099.
21.Forbes JA, Keller CK, Smith JW, et al. Analgesic effect of naproxensodium, codeine, a naproxen-codeine combination andaspirinonthepostoperativepainoforalsurgery. Pharma-cotherapy.1986;6:211---8.
22.YellonRF, Kenna MA,CladisFP, etal. Whatis thebest non-codeinepostadenotonsillectomypainmanagementforchildren? Laryngoscope.2014,http://dx.doi.org/10.1002/lary.24599. 23.RacoosinJA,RobersonDW,PacanowskiMA,etal.Newevidence
aboutanolddrug---riskwithcodeineafteradenotonsillectomy. NEnglJMed.2013;368:2155---7.
24.White PF. The changing role of non-opioid analgesic tech-niquesinthemanagementofpostoperativepain.AnesthAnalg. 2005;101:S5---22.