www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
In
vitro
antimicrobial
activity
of
Luffa
operculata
夽
,
夽
Rodolfo
Alexander
Scalia
a,b,∗,
José
Eduardo
Lutaif
Dolci
c,
Suely
Mitoi
Ykko
Ueda
d,
Suzethe
Matiko
Sassagawa
daDepartmentofOtorhynolaryngology,IrmandadedaSantaCasadeSãoPaulo,SãoPaulo,SP,Brazil
bPostgraduatePrograminSurgeryResearch,MedicalSciencesSchool,SantaCasadeSãoPaulo(FCMSCSP),SãoPaulo,SP,Brazil cMedicalSciencesSchool,SantaCasadeSãoPaulo(FCMSCSP),SãoPaulo,SP,Brazil
dDepartmentofPathologicalSciences,MedicalSciencesSchool,SantaCasadeSãoPaulo(FCMSCSP),SãoPaulo,SP,Brazil
Received23June2014;accepted24July2014 Availableonline25December2014
KEYWORDS
Luffaoperculata; Sinusitis;
Productswith antimicrobialaction; Phytotherapeutic drugs
Abstract
Introduction:Luffaoperculataisprobablyoneofthemostpopularherbalmedicinesusedin thetreatmentofrhinitisandrhinosinusitis.However,itsspecificmechanismofactionisstill unknown.
Objective:ToevaluateinvitroantibacterialactivityofL.operculataagainstthreeordinary agentsofupperrespiratorytractinfection:Staphylococcusaureus,Streptococcuspneumoniae andStreptococcuspyogenes.
Methods:DifferentconcentrationsofL.operculataalcoholicextractwereappliedtobacterial brothcontainingreferenceandcommunitystrainsofthethreedescribedagents.Aftera24-h incubationperiod,thebacterialcultureturbiditywasmeasured.Thesampleswerethen inoc-ulatedontoMueller-Hintonandhumanbloodagarplates.Bacterialgrowthwasanalyzedafter 24-and48-hincubationperiod.Thetestwasconsiderednegativewhentherewasno environ-mentalturbidity,confirmedbytheabsenceofbacterialgrowthintotheinoculatedplates.Tests wereconsideredpositivewheneitherturbiditychangeswereobservedonthebacterialbroth orwhenbacterialgrowthwasdetectedoninoculatedplates.Appropriatestatisticalanalysisof thedatawasperformed.
Results:L.operculataextractsshowed antibacterialactivitymainlytoS.pyogenesfollowed byS.pneumoniaeandS.aureus.
Conclusions:L.operculataextractshowedpromisingantibacterialactivityinvitroagainstthe studiedagents.
© 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:ScaliaRA,DolciJEL,UedaSMY,SassagawaSM.InvitroantimicrobialactivityofLuffaoperculata.BrazJ Otorhinolaryngol.2015;81:422---30.
夽
Institution:StudyconductedatMedicalSciencesSchool,SantaCasadeSãoPaulo(FCMSCSP),toobtainDoctorate’sdegreeinSurgery Research.
∗Correspondingauthor.
E-mail:[email protected](R.A.Scalia).
http://dx.doi.org/10.1016/j.bjorl.2014.07.015
1808-8694/©2014Associac¸ãoBrasileiradeOtorrinolaringologia eCirurgiaCérvico-Facial. PublishedbyElsevierEditoraLtda.All rights
PALAVRAS-CHAVE
Luffaoperculata; Sinusite;
Produtoscomac¸ão antimicrobiana; Medicamentos fitoterápicos
AtividadeantimicrobianainvitrodaLuffaoperculata
Resumo
Introduc¸ão: ALuffaoperculataé,provavelmente,ofitoterápicomaisutilizadonotratamento dasriniteserinossinusites.Apesardeamplamenteutilizadapelapopulac¸ão,seusmecanismos deac¸ãoaindanãoestãocompletamenteestabelecidos.
Objetivo: Avaliar a atividade antimicrobiana in vitro da Luffa operculata em agentes causadoresdeinfecc¸õesdeviasaéreassuperiores:Staphylococcusaureus,Streptococcus pneu-moniaeeStreptococcuspyogenes.
Método: Foramutilizadasdiferentesconcentrac¸õesdeextratoalcoólicodeLuffaoperculata emcaldodebactériasdosagentesavaliados.Apósincubac¸ãode24horasfoirealizadaaleitura deturvac¸ãodomeio,eposteriormente,semeaduraemplacasdeágar-sangueeágar Muller-Hinton, após24 e 48 horasdeincubac¸ão.Foramconsiderados testes negativosaqueles em quenãohouveaturvac¸ãodomeio,confirmadospelaausênciadocrescimentodasbactérias nassemeaduras.Foramconsideradospositivosostestesqueapresentaramturvac¸ãodocaldo oupositividadenassemeadurasde24ou48horas.Osresultadosforamsubmetidosàanálise estatísticapertinente.
Resultados: OsextratosdeLuffaoperculataapresentaramatividadeantimicrobiana, especial-menteparaStreptococcuspyogenes,seguidodosStreptococcuspneumoniaeeSthaphylococcus aureus.
Conclusões: Oextratode Luffa operculata apresentou promissoraatividade antimicrobiana invitrocontraosagentesestudados.
©2014Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Thewidespreaduseofantibioticstotreatbacterial rhinos-inusitis,besidestheeliminationoftheoffendingorganism, aimstorestorethenormalfunctionofthenasalmucosaand theparanasalsinuses,shorteningthedurationofsymptoms andpreventinglocalandintracranialcomplications.1
Althoughwidelyused,antibioticsarenottheonly thera-peuticoptionforrhinosinusitis.2Adjuvanttreatmentsshould beused,inaccordancewiththesymptoms,needsand lim-itations of each patient. In general, nasal washes with salinesolutions,topicalandsystemiccorticosteroids, anti-histamines, nasal decongestants, and mucolytics, among others,mayalsobeused.1---4
One of the therapeutic options employed by a large portionof the populationin the treatment of rhinosinusi-tisistheuseofphytotheraphy,or herbalism.Traditionally usedbythepoorsegmentoftheBrazilianruralpopulation, especiallyin North,Northeastand Midwestregions of the country,herbalmedicinehasbeenusedincreasinglyinurban centersacrossthe country,by patientsof variouscultural andsocioeconomiclevels.4
Amongthemedicinalplantsusedinformallyforthe treat-mentofrhinitisandrhinosinusitis,Luffaoperculata,known inBrazilas‘‘cabacinha’’or‘‘buchinha-do-norte’’,is prob-ablythemostcommonlyused.5,6L.operculatapossessesa numberoftherapeuticproperties,accordingtothe Brazil-ian population. Although several studies in the literature soughttoidentifythemechanismsbywhichL.operculata exhibitssuchproperties,noevidenceofantihistamine, vaso-constrictor,anti-inflammatory, or antiviral activity of this
herbal medicine wasfound.7---10 Structural changes in the respiratorymucosa were described by experimental stud-ies;however, the concentration and the way in which L. operculatawasusedwerenotclearlystated.4,11
In a recent systematic review on L. operculata effec-tivenessin the clinical treatment of rhinosinusitis, it was concludedthatmanyclarifyingscientificdataonthesubject arestillmissing,andthatthedatacurrentlyavailable are stillverycontroversial.12 Thus,new,insightfulandreliable studiesareinorder,sothatL.operculatacanbeusedsafely andeffectivelyinthetreatmentofsinonasaldiseases.12,13
Inanattempttoelucidatetheseproperties,theaimof thisstudywastoevaluatetheinvitroantimicrobialactivity ofL.operculata againstsomecausativeagents of rhinosi-nusitis.
Methods
The study wasconducted in the Laboratory of Microbiol-ogy,Departmentof PathologicalSciences andDepartment ofOtorhinolaryngology,afterapprovaloftherelevant Sci-entificCommittees.TheResearchEthicsCommitteeofthe institution waived the evaluation of the project, because thereis noinvolvementof human beings or experimental animals.
Obtainingmicroorganisms
Table1 McFarlandnephelometricscalewiththeestimatednumberofbacteriaineachtube.
Tubeno. 0.5 1 2 3 4 5 6 7 8 9 10
Approximatenumberofbacteria(×108) 1.5 3 6 9 12 15 18 21 24 27 30
of Microbiology of the institution. In addition, strains of AmericanTypeCulture Collection (ATCC) origin were also selected.
ATCCstrainsarestandard strainswithaknown suscep-tibilityprofile(i.e.,theyhave aserialnumberthatallows ustoknow,regardlessof where theyareevaluated, their responsefrompreviouslytestedantibiotics),thereby ensur-ingthereproducibilityofthestudy.
Despite ATCCstrainspresent aknown profile,it is not possible to evaluate the antimicrobial activity of a new drugwithout also usingstrains of clinical origin, because ATCC strains do not represent bacteria causing diseases indaily life. Strainsof clinical origin arenecessary, since they have different susceptibility profiles, which ensure greater fidelity for the evaluation of antimicrobial action withrespecttothoseorganismsofinterest.
ATCCstrainsmaybesensitive orresistant.Those sensi-tivestrains,usedinthisstudy,showsensitivitytoantibiotics usedinclinicalpractice,butthisisnotthecasewith resis-tant strains. Conceptually,ATCC strains, when presenting resistancetotwoormoreclassesofantimicrobialstowhich theywouldbe originallysensitive, areclassified as multi-resistantstrains.
The most prevalent etiologic agents of bacterial rhi-nusinusitis are Streptococcus pneumoniae, Haemophilus influenzaeand Moraxellacatarrhalis;but therearemany factors involved in the acquisition, culture, and mainte-nanceofeachofthesebacterialorganisms,whichinfluenced thechoiceofagentsinourstudy.
H. influenzae and M. catarrhalis are fastidious slow-growing bacteria that require special culture media and nutrientsfortheirdevelopment.This,togetherwiththefact thatmostofourpatientswhohadculturessenttothe lab-oratoryhadbeentreatedwithantibioticspriortospecimen collection,resultedintheisolationofonlyafewstrainsof
M.catarrhalisandH.influenzaeduringthe26-monthperiod ofestablishingourbacterioteca.Evenaftertheirisolation, duetopreservationdifficulties,noneofthestrainsremained viable,precludingtheiruseinourresearch.
Given that Staphylococcus aureus, S. pneumoniae and
Streptococcuspyogenesareprevalentinupperairway infec-tionsandlessfastidiousbacteriaanddonotrequirespecial culturemediatomaintaintheirviabilityandgrowth,these organismswereselectedforthisstudy.
Theselectionofthestrainsoccurredasfollows:
a S.aureus(25strains):
1ATCC-25923sample---standardstrain,withaknown sensitivesusceptibilityprofile.
24isolatesofclinicaloriginwithavariable susceptibil-ityprofile.
b S.pneumoniae(25strains):
1ATCC-49619sample---standardstrain,withaknown sensitivesusceptibilityprofile.
24isolatesofclinicaloriginwithavariable susceptibil-ityprofile.
c S.pyogenes(25strains):
1ATCC-19615sample---standardstrain,withaknown sensitivesusceptibilityprofile.
24isolatesofclinicaloriginwithavariable susceptibil-ityprofile.
Withthe aidofasterilized platinumloop,strainsofS. aureus, S. pneumoniaeand S. pyogenes were transferred totesttubescontaining10mLofcasein-peptone soymeal-peptonebroth,i.e.,TrypticSoyBean(TSB),anenvironment thatallowspreservationofbacterialviability.Suspensionsof themicroorganismswerestandardizedbytheircomparison to0.5inaMcFarlandscale,correspondingtoapproximately 1.5×108CFU/mL(ColonyFormingUnitspermilliliter).
TheMcFarland scale (Table1)is anephelometricscale of 11 tubes, numberedfrom0.5 to10; itsturbidity stan-dardisthemostoftenusedinmicrobiologylaboratoriesin Braziland intheUnited Statestodeterminetheintensity ofbacterialmultiplicationinliquidculturemedia.The bac-terialmultiplication precludesthe passageoflight, which causes turbidityandopacification ofthe culture medium. Thegreaterthenumberofbacteriapresentinthesample, the greater the turbidityof the culture medium. Recom-mendedbytheClinicalandLaboratoryStandardsInstitute (CLSI), United States, the McFarland nephelometricscale wasalsoadoptedandrecommendedbyANVISAinBrazil.14 With thisregulation, it is possible toestablish astandard thatcanbegaugedatanylocationinthecountry,generating correspondenceinthereadingoftheirresults.
ObtainingconcentrationsofL.operculata
The evaluation of the in vitro antimicrobialactivity of L. operculatawithrespecttothetestedagentswasperformed by the brothmacrodilutiontechnique, withL. operculata concentrationsof0.2%;0.3%;0.4%;0.5%;1%and2%inTSB culturemedium.
AnalcoholicextractofL.operculata(Schraiber®),batch number5343,with125mL,alcoholstrengthof65%,withL. operculataconcentrationof10%wasused.Thisproductwas manufacturedonOctober6,2010withvalidityperioduntil October6,2015.
Table2 Calculationofdilutionsfromtheinitialconcentrationof10%alcoholicextractofLuffaoperculata.
ConcentrationsofLuffaoperculata(%) Luffaoperculata10%(mL) TSB(mL) Luffaoperculata+TSB(mL)
0.2 0.2 9.8 10
0.3 0.3 9.7 10
0.4 0.4 9.6 10
0.5 0.5 9.5 10
1 1 9 10
2 2 8 10
TSB,TrypticSoyBean.
After thisdilution, 1mLof alcoholic extractin several concentrations wasdeposited into differentdry and ster-ile 10×1.5-cm test tubes. Next, 1mL of bacterial broth (concentration of 0.5 McFarland, which corresponds to approximately 1.5×108CFU/mL) was deposited in these
testtubes.Allturbiditytests,24-and48-hcultures,and con-trolswereperformedinduplicateforallconcentrations,and controlswereperformedinduplicateforallconcentrations, inordertoexcludeanysamplecontamination.
Controls
Toavoidbiasintheinterpretationofdata,threesample con-trolswereperformed:anegativecontrol,apositivecontrol andanalcoholiccontrol.
For negative control, a 2-mL tube containing L. oper-culata was used; and for positive control, another 2-mL tube with bacteria broth was used. These tubes were taken to the incubator, where they were incubated at about37◦C±2◦C×24h.After24h,atubereadingwas
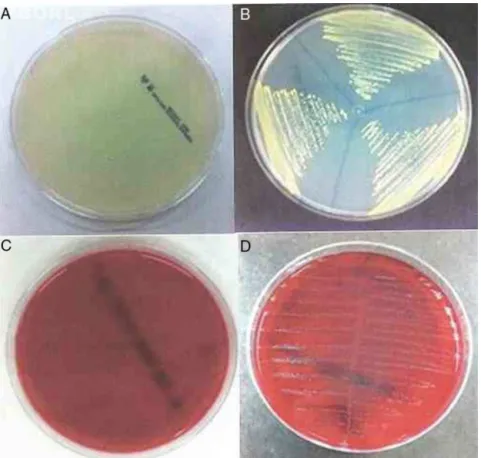
per-formed, to ascertain whether or not there was bacterial growth,whichwasindicatedbytheoccurrenceofmedium turbidity.Alltubeswereplatedon90-mmbloodagarplates toassessgrowthandviabilityofS.pneumoniaeandS. pyo-genes,andon150-mmMuellerHintonagarplatestoassess growth and viabilityof S. aureus. Plate reading was per-formedafter24and48h.
Withrespecttoouranalysiscriteria,testsnotpresenting medium turbidityafter bacterialinoculation were consid-ered negative, andthis was confirmed by the absenceof bacterialgrowthin24-and48-hinoculations.Tests exhibit-ingbrothturbidityorpositivityin24-and48-hinoculations wereconsideredpositive(Figs.1and2).
The simple absenceof turbidityin the test tubesdoes notmakeitpossibletoassertwhetherornottherewas bac-terialeradicationinamediumcontainingL.operculataand inbacterialbroth.Ontheotherhand,thisfindingallowsus tostatethattherewasaminimuminhibitoryconcentration (MIC),i.e.,theminimumconcentrationatwhich bacterial growth wasinhibited. Ifbacterial growth in 24- and48-h inoculationsoccurred,thissuggeststhatagreaterL. oper-culataconcentrationwillberequiredtokillallbacteria.On theother hand,when,duringthereading,the absenceof turbidityisconfirmedbybacterialgrowthabsencein24-and 48-hinoculations,wecanestablishtheminimum bacterici-dalconcentration(MBC), i.e.,theminimumconcentration requiredforkillingallbacteria.
Afterdilution ofL.operculataextractto10% andwith an alcoholic contentof 65% for L.operculata extracts at concentrations of 0.2%;0.3%; 0.4%; 0.5%; 1% and2%, the alcoholcontentofthesameconcentrationswascalculated (Table3).
Thehigheralcoholiccontentfoundwas13%ata concen-tration of 2% of L. operculata. To confirm the absence ofantimicrobial action by ethanolin these different con-centrations,ethanoltubeswithdifferentalcoholstrengths (between 1.35% and 13%) and with bacterial broth were taken to the incubator, where the tubes were incubated atabout37◦C±2◦C×24h.After24h,atube readingwas
performed to verifywhether there wasbacterial growth, indicated by medium turbidity; culturing of all tubes on 90-mmagar-bloodplateswasperformedtoassessS. pneu-moniae andS. pyogenes growth and viability.We did the samefor S. aureus on150-mm Muller-Hinton agar plates. Thisschemewasrepeatedafter48hincubation.
Toassesstheagreementbetweenthemethodsof turbid-ityandof24-and48-hcultures,theKappamethod,which aims, by ameasure of association, toestablish an agree-mentbetweenqualitativevariables,wasused.Itsvaluecan beequal to zero, or non-zero. When a non-zero value is obtained, the agreementis calculated. The agreement is deemed poor when p<0.4; moderate, when 0.4<p<0.6; and strong when p>0.6. All samples were performed in
Figure2 Muller-Hintonagarplates:(A)nobacterialgrowth;(B)withbacterialgrowth.Blood-Agarplates:(C)nobacterialgrowth; (D)withbacterialgrowth.
duplicate.TheprogramusedforstatisticalanalysiswasSPSS 13.0forWindows.
Results
Controls
Inallconcentrationsconsidered,noneofthenegative con-trol tubes with L. operculata showed visible turbidity or growthofanybacteriastrain.
Allbacterialbrothandallalcoholiccontrolsshowed vis-ibleturbidityand specificbacterialgrowth ofeach broth, withoutsamplecontamination.
Allnegative, positive and alcoholic controls were per-formedinduplicateforallsamples,havingconfirmedtheir results.
Microorganisms
AlltubescontainingL.operculataatconcentrationsof0.2% and0.3%andwithS.pyogenes,S.pneumoniaeandS.aureus bacterial broth showed turbidity after a 24-h incubation period.The24-and48-hseedingsconfirmed thepresence ofbacteria,showinggrowthof justthosebacteriatested, whichexcludedanysamplecontamination.
All tubes containing L. operculata at a concentration of 0.4% and with S. pyogenes bacterial broth showed no
Table3 Calculationofdilutionsandalcoholstrengthfromtheinitialconcentrationof10%alcoholicextractofLuffaoperculata, andwithalcoholicstrengthof65%.
Concentrationsof Luffaoperculata(%)
Luffaoperculata 10%(mL)
TSB(mL) Luffa
operculata+TSB(mL)
Alcoholic strength(%)
0.2 0.2 9.8 10 1.30
0.3 0.3 9.7 10 1.95
0.4 0.4 9.6 10 2.60
0.5 0.5 9.5 10 3.25
1 1 9 10 6.50
2 2 8 10 13.00
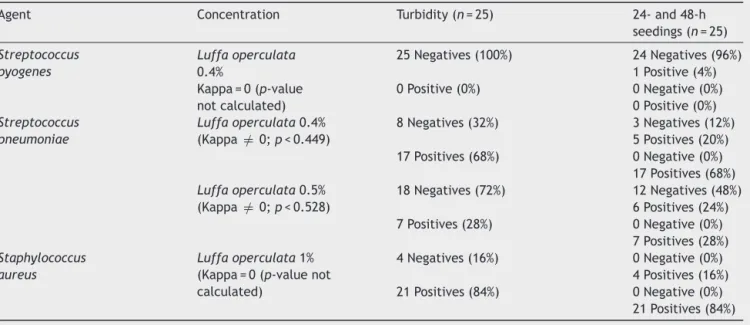
Table4 TurbidityandseedingresultsonbacterialagentsforLuffaoperculataindifferentconcentrations.
Agent Concentration Turbidity(n=25) 24-and48-h
seedings(n=25)
Streptococcus pyogenes
Luffaoperculata 0.4%
25Negatives(100%) 24Negatives(96%) 1Positive(4%) Kappa=0(p-value
notcalculated)
0Positive(0%) 0Negative(0%) 0Positive(0%) Streptococcus
pneumoniae
Luffaoperculata0.4% (Kappa =/ 0;p<0.449)
8Negatives(32%) 3Negatives(12%) 5Positives(20%) 17Positives(68%) 0Negative(0%)
17Positives(68%) Luffaoperculata0.5%
(Kappa =/ 0;p<0.528)
18Negatives(72%) 12Negatives(48%) 6Positives(24%) 7Positives(28%) 0Negative(0%)
7Positives(28%) Staphylococcus
aureus
Luffaoperculata1% (Kappa=0(p-valuenot calculated)
4Negatives(16%) 0Negative(0%) 4Positives(16%) 21Positives(84%) 0Negative(0%)
21Positives(84%)
turbidityafter a 24-h incubation period. However,among those25samplesofS.pyogenes(ATCC-19615and24clinical isolates) tested, a clinical isolate (4%) showed bacterial growthin24-and48-hseedings(Table4).
Amongthe25tubescontainingL.operculataata concen-tration of 0.4% and with S. pneumoniae bacterial broth (ATCC-49619and24clinicalisolates),theATCCsampleand twoclinicalisolates(12%)showednoturbidityaftera24-h incubationperiodandnobacterialgrowthin24-and48-h cultures.Fiveother clinicalsamples(20%) showedno tur-bidityaftera24-hincubation,butshowedgrowthin24-and 48-hcultures.Seventeenclinicalisolates(68%)showed tur-bidityaftera24-hincubation periodandbacterialgrowth in24-and48-hcultures.These25culturesshowedgrowth onlyfor S. pneumoniae,whichexcluded anytypeof sam-ple contamination.Statistical analysisshowed Kappa =/ 0 andp<0.449,indicating amoderatelysuggestiveresultof antimicrobialresponse(Table4).
All tubescontainingL.operculata at concentrationsof 0.4%and0.5%andwithS.aureusbacterialbrothshowed tur-bidityaftera24-hincubationperiod.24-and48-hcultures confirmedthepresenceofthesebacteria.
All tubescontainingL.operculata at concentrationsof 0.5%;1%and2%andwithS.pyogenesbacterialbrothshowed noturbidityaftera24-hincubationperiodandnobacterial growthin24-and48-hcultures.
Amongthe25tubescontainingL.operculataata concen-tration of 5% and with S. pneumoniae bacterial broth (ATCC-49619and24clinicalisolates),theATCCsampleand 11clinical isolates(48%) showednoturbidityaftera24-h incubationperiod,orbacterialgrowthin48-hcultures.Six otherclinicalisolates(24%)showednoturbidityaftera24-h incubationperiod,butwithgrowthafter24-and48-h cul-tures.Seven clinical isolates(28%) showed turbidityafter a 24-h incubation periodand bacterial growth in 24- and 48-hcultures.These25culturesshowedgrowthonlyofS. pneumoniae,whichexcludedanytypeofsample contami-nation.StatisticalanalysisshowedKappa =/ 0andp<0.528,
indicating amoderately suggestive resultof antimicrobial response(Table4).
ThetesttubescontainingL.operculataatconcentrations of1%and2%andwithS.pneumoniaebacterialbrothshowed noturbidityaftera24-hincubationperiodandnobacterial growthin24-and48-hcultures.
Amongthe25tubescontainingL.operculataata concen-trationof1%andcontainingS.aureus(ATCC-25923and24 clinicalisolates),theATCCsampleandthreeclinicalisolates (16%)showedno turbidityaftera 24-h incubation period; however, all showed growth after 24- and 48-h cultures (Table4).
ThetubescontainingL.operculataataconcentrationof 2%andwithS.aureus bacterialbrothshowednoturbidity aftera24-hincubationperiodandnobacterialgrowthin 24-and48-hcultures.
Discussion
Extractchoice
Oneofthemajordifficultiesintheuseofherbalmedicine incontrolledstudiesisthelackofstandardizationofherbal drugs.Noneoftheexperimentalstudiespublishedbetween 2001and2010hadthesamemethodofobtainingL. opercu-lataextracts.4,11---13
Aimingtoavoidthepresenceofcontaminatedfruitsthat couldcontaminatethesamplesin ourstudy,aswell asto ensurethatthesameextractwasusedthroughoutthework, we chose touse an industrialized alcoholic extract of L. operculata, whose accesswas available for replication of thestudy,ifnecessary.
It is relevant to note that the reproducibility of the researchisrestricted tothebatchspecificallyusedinthis study.Dependingontheconditionsofsoil,sunlightand rain-fallindex,wecannotguaranteethatotherbatchesproduced inotherseasonsorwithorigininothercropswouldhavethe sameresults found in ourstudy.It is importanttoensure somecomparison level inthe conduction of other studies usingdifferentL.operculataextractsatthesame concen-trationsandwiththesamebacterialagents.
Concentrationsused
Since1960afew articleshave attemptedtoevaluatethe mechanismsof action by which L.operculata acts onthe respiratoryepithelium,andalsotoproveitstherapeutic effi-cacyintheclinicaltreatmentofrhinosinusitis.12Theauthors could not identify anything that would establish reliable criteriafor itssafeuse12 andsome actuallyreportedthat theimproperuseofthisherbalproduct,especiallyathigh concentrations of L. operculata, can lead to a worsening ofsinonasal conditions.4,6 Nevertheless, some clinicaland experimentalstudieslistconcentrationsof0.5%and1%for thetreatmentofrhinosinusitis.13,16,17
As we found noreferences onantimicrobialactivity of L. operculata in the literature before 2008, when, in a singlestudy, only one screening procedure withdifferent bacteriaandfungiwasconducted,18 wechosetostartour investigation with a concentration of 1%, the same level presentinthiscommercialextract,releasedbyANVISAand testedinmoststudiescitedintheliterature.11,13,17Weused twice the recommended concentration (2%), thus setting alimit to thisantimicrobial activity, without approaching LD507,16 or causing an increase of its deleterious effects tothe mucosa. Finally, other concentrations (0.2%; 0.3%; 0.4%and0.5%)wereevaluated,inanattempttoestablish aminimumconcentrationinwhichL.operculataexhibited anantimicrobialeffect,soastominimizeanysideeffects.
Bacterialagents
AlltubescontainingL.operculataatconcentrationsof0.2% and0.3%andwithS.pyogenes,S.pneumoniaeandS.aureus bacterial broth showed turbidity after a 24-h incubation period,indicatingbacterialgrowthintheseconcentrations, andhence,noantimicrobialactiontothesemicroorganisms. All tubes containing L. operculata at a concentration of 0.4% and with S. pyogenes bacterial broth showed no turbidity after a 24-h incubation period, demonstrating antimicrobialactivityfor thisagent,inthisconcentration. The absence of visual turbidity per se led tothe conclu-sionthat,ataconcentrationaround0.4%,itwaspossibleto determineMICforS.pyogenes.
Considering that the absence of visual turbidity, con-firmedbyanabsenceofgrowthin24-and48-hcultures,only occurredinthosetubeswithL.operculataatconcentrations
greaterthan0,5%,itwasinferredthat,withconcentrations aroundthislevel,MBCoftheseagentscanbeestablished.
SomesamplescontainingL.operculataatconcentrations of0.4% and0.5% andwithS. pneumoniaebacterialbroth, showednomedium turbidity.However,thefactthatsome samples presented bacterial growth in the cultures con-firmedthat,withaconcentrationaround0.4%or0.5%,we canestablishMICforS.pneumoniae,inthesamelineasfor S.pyogenes.
AtL.operculataconcentrationshigherthan1%,neither turbidityin tubes containing S. pneumoniaenor bacterial growth in 24- and 48-h cultures wasperceived; however, considering that no intermediateconcentrations between 0.5% and 1% were tested, we cannot conclude that MBC forS. pneumoniaeis equalto1%.Itmaybethat,at some concentrationbetween0.5%and1%,thekillingofalltested bacteria occurs, and in order for this tohappen, clinical studieswithagreater L.operculata concentrationvariety wouldbeneededtoestablishitsMBC.
SometubescontainingL.operculataataconcentration of1% andwithS. aureusbacterialbrothshowednovisual turbidity after the 24-h reading, suggesting that, at this concentration,L.operculatashowedantimicrobialactivity forthisagent,therebyestablishingitsMIC.Onlyata concen-trationof2%therewasnoturbidityandnobacterialgrowth in24-and48-hcultures;however,asalsooccurredwithS. pneumoniae,wecannotguaranteethatthisconcentration representsitsMBC.Thelackofintermediateconcentrations between1%and2%isnoguaranteethatavaluehigherthan 1%andlowerthan2%alsomaybeabletoeradicateallS. aureusorganisms(Table5).
In spite of being Gram-positive cocci, S. pyogenes, S. pneumoniae and S. aureus showed different susceptibil-ity profiles, when in a milieu containing L. operculata. Lowerconcentrationsofaround0.5%wereabletokillallS. pyogenes organisms, whileS. pneumoniaeorganismswere eradicatedonlyataconcentrationof1%;asforS. aureus, itseradicationoccurredonlyataconcentrationof2%.This responsetothe presence ofL.operculata wasequivalent to the response of these microorganisms to conventional antibiotics.Therearemultiplemechanismsbywhichthese bacteriadevelopresistancetoantibiotics.
S.pneumoniae,forexample,hasacapsulethatimpairs theactionofantimicrobialagentsonitscellwall.Usually, thisbacteriumismoreresistanttoantibioticsthanS. pyo-genes. On theother hand, S. aureus hasa greater ability togeneratebacterialresistancethanthosemicroorganisms previouslycited,inpartbecauseitisahighbeta-lactamase inducer.
Studylimitations
Table5 PresenceorabsenceofbacterialgrowthindifferentconcentrationsofLuffaoperculataextract.
Bacteria ConcentrationsofLuffaoperculata
0.2% 0.3% 0.4% 0.5% 1% 2%
Streptococcuspyogenes + + + − − −
Streptococcuspneumoniae + + + + − −
Staphylococcusaureus + + + + + −
+,presenceofbacteria(turbidityorseeding-positive);−,absenceofbacteria(turbidityorseeding-negative).
bacterialgrowthafter24-and48-hcultures,not replicat-ingtheresultsoftheATCCsample.Thelackofstudieswith extractsatintermediateconcentrationsbetween0.5%and 1%doesnotallowustostatethatitsMICis1%,butallowsus todeducethatMICmaybesituatedbetween0.5%and1%. Likewise,anMBCforS.aureusalsocannotbeestablished, butwecanstatethat,forthesesamplesusedinourstudy, MBCliesatconcentrationsofL.operculatabetween1%and 2%.
Nopreviousstudyhasevaluatedtheantimicrobial activ-ityofL.operculataagainstS.pyogenesorS.pneumoniae. ItbecameclearinourstudythatS.pyogenessampleswere moresusceptibletotheantimicrobialaction ofL. opercu-lata,comparedtoS. pneumoniaesamples, andthelatter organism,inturn,wasmoresusceptiblethanS.aureus.
Itisimportanttonotethatanumberofsubstances,such ascucurbitacinesBandD,glycosides,saponins,freesterols, organic acids and phenols, wereisolated fromthe phyto-chemical analysis of L.operculata.13,16,19 While a number ofsubstancesexhibittherapeuticeffects,othersmayhave toxic effects, leadingeven to a worseningof the clinical presentationupperairwayinfections.4
Thus, even with the promising antimicrobial effect of thisherbalmedicine,18furtherstudiesshouldbeconducted withtheaimtoestablishwhichofthesecomponentshavea therapeuticeffectandwhatarethemostappropriate con-centrations,sothatitsusedoesnotcausemoreharmthan good.Thesestudiesshouldseektorecognizeandseparate thetherapeuticandtoxiccomponentsofL.operculata,so onecanacceptordiscarditsuseinthetreatmentofupper airwayinflammatoryandinfectiousconditions.4,9,11---13
Considerationsforthefuture
Manystudies havebeenconductedtoelucidate the thera-peuticpropertiesofL.operculata.Thetaskofestablishing thetenuousrelationshipbetweentoxicityandtractabilityis thechallenge tobeconfronted. The findingofan antimi-crobial action in this herbal agent can be of great value in the therapeutic arsenal against upperairway diseases, consideringthat,everyday,mechanismsofbacterial resis-tanceincreasethecomplicationinthetreatment ofthese diseases.
It is a fact thatherbal medicines present variationsin theircharacteristicsandalsoexhibitchangesintheir compo-nents,dependingonvariationsinthecompositionofthesoil, rainfallindexandseasonalityoftheirharvest;thisresultsin aneverdifferentcompositionhavinguniquecharacteristics thatmakeitdifficulttoinducebacterialresistance.
Fromthe momentof the establishment of a safe dose ofL.operculataforuseintheoralcavity,itsantimicrobial effectagainst S. pyogenes could be of great importance, increatinganoralsprayforprophylaxisofrheumaticfever. Patientswithapositiverapidtestandnosignsorverysevere symptomscoulduse this spray,to eradicate thebacterial agentwithoutuseofsystemicantibiotics.
Thesamecanbesaidforthetreatmentofsinonasal dis-eases,wherethepresenceofbiofilmisproved.Thecaustic anddetergenteffectsofthisherbaldrug,throughtheaction ofitscucurbitacinesandsaponins(iftheirsideeffectsare controlled)could,inlowdoses,beusefulinthedestruction ofpolysaccharides’structure,thusfacilitatingtheactionof anassociatedantibiotictoresolvethesediseases.
Itisimportantthatwecontinuesearchingforinformation abouttheseandotherherbalremedies,inanattempttofind solutionstoproblemsthatarise everyday, andthatoften resultinfailurewiththeresourcescurrentlyavailable.
Conclusion
L. operculata extract showed promising antimicrobial activity in vitro against the causative agents of upper airway bacterial infections tested in this study, both in those microorganisms with known susceptibility and pro-file(ATCC), andin thoseofclinical origin.This can bean importantstepincreatingnewdrugstotreatthesediseases.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Anon JB, Jacobs MR, Poole MD, Ambrose PG, Benninger MS,HadleyJA, etal. Antimicrobialtreatmentguidelines for acute bacterial rhinosinusitis. Otolaryngol Head Neck Surg. 2004;130:1---45.
2.Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgia Cérvico-Facial(DepartamentodeORLdaAssociac¸ãoMédicaBrasileira). Diretrizes Brasileiras de Rinossinusites. Rev Bras Otorrino-laringol(Supl).2008;74:S1---59.
3.FokkensWJ,LundVJ,MullolJ.Europeanpositionpaperon rhi-nosinusitisandnasalpolyps.RhinolSuppl.2007;20:1---136.
4.Menon-MiyakeMA.EfeitosdainfusãodeLuffaoperculatasobre oepitélioeaatividademucociliardopalatoisoladoderã [the-sis].SãoPaulo:FaculdadedeMedicinadaUniversidadedeSão Paulo;2004.
6.Menon-Miyake MA, Caniello M, Balbani APS, Butugan O. Inquéritosobreo usodeplantasmedicinaisparatratamento de afeccc¸ões otorrinolaringológicas entre pacientes de um hospitalpúblicoterciário.CadernodeDebates.RevBras Otor-rinolaringol.2004;70:43---55.
7.SilvaJB.AlgumaspesquisassobresaponinasdaLuffa opercu-lata.RevFarmBioquímSãoPaulo.1964;2:153---60.
8.ChampneyR,FergusonNM,FergusonGG.Selected pharmaco-logicalstudiesofLuffaoperculata.JPharmSci.1974;63:942---3.
9.SilvaEA. Contribuic¸ãoparao estudofarmacológicoda Luffa operculata cogniaux [dissertation]. Fortaleza: Universidade FederaldoCeará;1983.
10.Glatthaar-Saalmüller B, Fallier-Becker P. Antiviral action of Euphorbiumcompositumanditscomponents.Forsch Komple-mentarmedKlassNaturheilkd.2001;8:207---12.
11.Roncada PRA. Estudo analítico das alterac¸ões estruturais e ultra-estruturais da superfície do epitélio da mucosa nasal (conchainferior esepto nasal)decoelhos apóso usotópico do extrato dofrutoda Luffaoperculata[thesis]. São Paulo: Faculdadede Ciências Médicas daSanta Casade São Paulo; 2001.
12.SousaNetoPS.Luffaoperculata:mecanismodeac¸ãonoepitélio respiratórioeeficácia terapêuticano tratamentoclínicodas rinossinusites: revisãosistemática [thesis].São Paulo: Facul-dadedeCiênciasMédicasdaSantaCasadeSãoPaulo;2006.
13.CamposCAC. Eficáciade soluc¸ãotópica nasal de extrato de Luffaoperculataparatratamentoderinossinusitebacteriana em coelhos [dissertation]. São Paulo: Faculdade de Ciências MédicasdaSantaCasadeSãoPaulo;2008.
14.The National Committee for Clinical Laboratory Stan-dards (NCCLS). Metodologia dos testes de sensibilidade a agentesantimicrobianospordiluic¸ãoparabactériade cresci-mento aeróbico: norma aprovada---6a
ed. M7-A6, 23; 2011. p.1---81.
15.Amaral FMM, Coutinho DF, Ribeiro MNS. Controle de quali-dadedefrutosdeLuffaoperculataCogn.Comercializadosem MercadosdeSãoLuiz/Maranhão,Brasil.RevHospUnivUFMA. 2001;3:9---13.
16.VasquesCAV,VasquesNV,ArraesLA,GellerM.Revisão farma-cognósticadacabacinha(LuffaoperculataCogn.).FolhaMed. 1986;93:185---7.
17.Salviano PA. Tratamento da sinusite com preparac¸ão con-tendo Luffaoperculata e soluc¸ão fisiológica.Rev Bras Med. 1992;49:681---2.
18.Caribé RA. Abordagem da atividade biológica do extrato de Luffa operculata Cogn. (cucurbitaceae) [disserta-tion]. Pernambuco: Universidade Federal de Pernambuco; 2008.