CHRONIC PACHYMENINGITIS ASSOCIATED
TO HYPEREOSINOPHILIA
C A S E R E P O R T
J. CORREALE * — S. AMERISO * — F. MELI * * — R. REY * O. GARCEA * — D. MONTEVERDE *
SUMMARY — A m a l e 22 y e a r s old p a t i e n t w h o c o n s u l t e d d u e t o h e a d a c h e a n d i n c r e a s i n g v i s u a l loss is b e i n g p r e s e n t e d . A l t e r a t i o n s in t h e e x a m w e r e r e p r e s e n t e d b y r i g h t a m a u r o s i s a n d left t e m p o r a l h e m i a n o p s i s . P a t h o l o g i c a l a n d t o m o g r a p h i c a l s t u d i e s r e v e a l e d c h r o n i c p a c h y m e n i n g i t i s w i t h e o s i n o p h i l i c i n f i l t r a t i o n . A n e l e v a t e d e o s i n o p h i l i a a n d a n i n c r e a s i n g in a n t i - A a n d a n t i - B i s o a g g l u t i n i n s w e r e a s s o c i a t e d t o t h e clinical c o u r s e . T h e y r e t u r n e d t o n o r m a l v a l u e s a f t e r t r e a t m e n t w i t h t i a b e n d a z o l . E v e n t h o u g h t h e r e i s n o t a c e r t a i n conclusion a s r e g a r d s t h e etiology, t h e p r o b a b l e p a r a s i t a r y n a t u r e of t h e p r o c e s s is o u t l i n e d .
Paquimeningitis crónica asociada a hipereosinofilia : relato de caso.
R E S Ú M E N — U n p a c i e n t e d e 22 a ñ o s d e sexo m a s c u l i n o , q u e c o n s u l t o p o r cefaleas y d i s m i n u c i ó n d e l a a g u d e z a v i s u a l es p r e s e n t a d o . L o s h a l l a z g o s p a t o l ó g i c o s d e l e x a m e n físico e s t u v i e r o n r e p r e s e n t a d o s p o r a m a u r o s i s d e r e c h a y h e m i a n o p s i a t e m p o r a l i z q u i e r d a . L o s e s t u d i o s t o m o g r á f i c o s y a n a t o m o p a t o l ó g i c o s p e r m i t i e r o n c o n c l u i r en u n a p a q u i m e n i n g i t i s c r ó n i c a con i n f i l t r a d o eosinofílico. U n a i m p o r t a n t e eosinofilia y u n i n c r e m e n t o en l a s i s o a g l u t i n i n a s a n t i - A y a n t i - B se vieron a s o c i a d a s al c u a d r o . L a s m i s m a s se n o r m a l i z a r o n luego del t r a t a m i e n t o con t i a b e n d a z o l . Si bien n o se p u e d e c o n c l u i r con c e r t e z a en el d i a g n ó s t i c o etiológico, se p l a n t e a l a p r o b a b l e n a t u r a l e z a p a r a s i t a r i a d e l p r o c e s o .
P a c h y m e n i n g i t i s c a s e r e c o r d s h a v e been classically a t t r i b u t e d to syphilis, t u -berculosis a n d alcoholism 26. N o w a d a y s c a s e s of p a c h y m e n i n g i t i s r e p o r t e d a r e few and, in m o s t of t h e m t h e c a u s e is u n c e r t a i n , even t h o u g h a p a t h o l o g i c a l s t u d y is a t t a i n e d . T h e use of c o m p u t e d t o m o g r a p h y ( C T ) s c a n s s h o w e d lesions which w e r e frequently clinically u n s u s p e c t e d . T h e p r e s e n c e of a s s o c i a t e d eosinophilia s t a b l i s h e s the possibility of t r y i n g t o explain p a r t i a l l y t h e c a u s e of s o m e of t h e s e lesions, w h e t h e r a s a direct c o n s e q u e n c e of t h e eosinophilic infiltration, by the n e u r o t o x i n p r o d u c e d by eosinophils, or r e p r e s e n t i n g p a r t of t h e systemic r e p e r c u s s i o n of a case due to a n o t h e r etiology.
W e refer to t h e case of a p a t i e n t w i t h h e a d a c h e a n d p r o g r e s s i v e visual loss. T h e C T s h o w e d a h y p e r d e n s e l a m i n a r lesion which w a s m a r k e d l y e n h a n c e d after t h e injection of c o n t r a s t s u b s t a n c e a n d e n g a g e d t h e left p a r a s e l l a r r e g i o n a n d t h e free e d g e of t h e t e n t o r i u m cerebeli. It w a s a s s o c i a t e d to a m a r k e d eosinophilia. T h e surgical biopsy d e m o n s t r a t e d chronic inespecific p a c h y m e n i n g i t i s similar to o t h e r s referred to by different a u t h o r s 9.17.
*Division of N e u r o l o g y , J . M. R a m o s M e j í a H o s p i t a l , B u e n o s A i r e s ; ** N e u r o l o g i c a l R e s e a r c h C e n t e r D r . R a ú l C a r r e a , B u e n o s A i r e s .
CASE R E P O R T
AO, a male 22 years old patient w a s admitted because he presented bilateral t'ronto-orbital headache and progressive visual loss. The s y m p t o m s had begun in an insidious w a y
60 days before his admittance and had evolved slowly till t w o d a y s before, at that time his s y m p t o m s worsened. H e w a s b e i n g treated w i t h corticosteroids w i t h o u t any improvement. The patient w a s born in Bolivia and he w a s a farmer. H e had been in contact w i t h dogs and cats and he had had repeated episodes of intestinal parasitosis in the past. He presented an amaurosis of the right eye and left temporal hemianopsis w i t h macular involvement. Photomotor and consensual reflexes were slow in both eyes. Papillar atrophy, retinal edema and v e s s e l s s h e a t i n g were observed in funduscopy w i t h s i g n s of periphlebitis in both eyes. No alterations appeared in the first lab study. Syphilis serology and tuberculin intradermal reaction were negative. Cerebrospinal fluid (CSF) study did not reveal any alteration in t h e cytochemical exam, nor in search for bacteria, mycobacteria or fungi. Immunological study s h o w e d : anti-nuclear factor (—), latex test for rheumatoid arthritis (—), L.E.cells
eosinophils count reaching 84% of the WBC (Table 1). Stools were negative for ova and parasites. H y d a t i c serology (double diffusion and CIB) w a s negative. An aspiration puncture of the bone marrow did not evidence any alteration. A new CSF w a s normal. Second immunological study revealed: l a t e x t e s t for rheumatoid arthritis (—), C3 152 mg/%, antimitochondrial antibody (_|_) 1/160, anti-A a g g l u t i n i n s 1/1024 and anti-B 1/4096. Lymphocyte populations w i t h monoclonal antibodies study revealed: T3 61%, T4 37%, TS 28%. Serologic-titrations for toxocara (ELISA and hemagglutination) were negative.
The patient w a s operated on. A thickening of the duramater, with adherences to the temporal lobe w a s observed, so a debridement of it w a s performed and a meningeal and encephalic parenchyma biopsy w a s made. The pathological study revealed: pachymeningitis with marked fibrosis, neoformation vessels, inflammatory infiltrates with abundant eosinophils; cerebral parenchyma presented significant edema, microglial and astrocytic migration and
D a y s since Relative value Absolute value
admittance of eosinophils of eosinophils
F i r s t d a y 0 0
50 9% 2520
71 25% 3000
78 37% 4662
88 78% 11700
96 80% 12000
149 84% 25200
166 47% 5120
187 9% 620
206 0 0
330 1% 89
COMMENTS
G o w e r s 9 as well a s W i l s o n 26 consider two t y p e s of p a c h y m e n i n g i t i s : the so called external, a t t r i b u t e d to processes t h a t have the skull bones a s their source (like osteomyelitis and t r a u m a t i s m s with s e c o n d a r y infection), g r a n u l o m a s in the same location or middle e a r infections. All of them g e n e r a t e limited hyperplasic reaction. T h e s e p a c h y m e n i n g i t e s , w i t h h e a d a c h e a n d sometimes slight t e m p e r a t u r e , can a f t e r w a r d s injure v e n o u s sinuses, c a u s i n g phlebitis t h r o m b o s i s or septicemia, and must be differentiated from e x t r a d u r a l a b s c e s s e s . T h e second g r o u p refers to w h a t these a u t h o r s call internal pachymeningitis, which can be seen in c a s e s of t r a u m a t i s m s , syphilis, tuberculosis a n d alcoholism, for instance. However modern neuropathological studies consider t h a t in most c a s e s one c a n n o t a s c e r t a i n such etiologies; so, most of them culminate having no determined c a u s e 9. Fcr.'nga and W e a t h e r b e e 9 related a case of h y p e r t r o p h i c g r a n u l o m a t o u s cranial pachymeningitis with p r o g r e s s i v e visual loss in a patient u n d e r g o i n g chronic dialysis. After necropsy etiology could not be established and it w a s designed a s allergical unspecific g r a n u l o m a t o s i s . Quite opposite to w h a t h a s previously been commented, isolated involvement of the a r a c h n o i d in the posterior fossa h a p p e n s to be relatively frequent in association with middle ear infec-tions, encephalic t r a u m a t i s m s , sinusitis, plaguicide intoxications a n d s t r o k e, t h u s forming 1 % of n e u r o s u r g i c a l interventions a c c o r d i n g to some statistics 20.
In a similar w a y a s the cases r e p o r t e d by K o b a y a s h i and c o l l .1 7
, our patient presented t o m o g r a p h i c lesions expressed by h y p e r d e n s e laminar left p a r a s e l l a r image with extension to the s p h e n o i d a l fissure, the optic foramen a n d the rectus oculi s u p e -rior muscle. T h i s lesion eroded the d o r s u m sellae a n d extended in a m a r k e d w a y along the free e d g e of the t e n t o r i u m cerebelli, e n h a n c i n g after the injection of c o n t r a s t medium. J u s t like in other cases referred to in the literature 9,17, in our patient it w a s impossible to determine a definite cause justifying chronic p a c h y m e -ningitis even t h o u g h meningeal a n d a d e n o p a t h y biopsy w a s performed. T h e presence of eosinophils in p e r i p h e r a l blood is sometimes associated with dysfunction of different o r g a n s . T h e u n d e r l y i n g c a u s e s a r e v a r i o u s a n d they include p a r a s i t o s e s , allergical affections, n e o p l a s i a s a n d vasculitis s.
P a t i e n t s in which the cause for eosinophilia is u n k n o w n a n d p r e s e n t a count of eosinophils g r e a t e r t h a n 1500/mm3 a t least d u r i n g 6 m o n t h s and have developed lesions in some o r g a n s can be said to b e a r hypereosinophilic s y n d r o m e 4. Different o r g a n s may be affected by the presence of these e l e m e n t s ; a m o n g t h e m : lungs, liver skin, eyes, muscles, lymph nodes, h e a r t a n d n e r v o u s system 4,8,11,13,23. Eosinophils a n d their p r o d u c t s (basic or cationic p r o t e i n s ) a r e openly neurotoxic. Moor? a n d coll. 19 described the development of neurological involvement in 6 5 % of studied p a t i e n t s b e a r e r s of hypereosinophilic s y n d r o m e , with r e p e r c u s s i o n t h r o u g h t h r e e phy-siopathological m e c h a n i s m s : e n c e p h a l o p a t h y , sensitive p o l y n e u r o p a t h y , thromboembolic p h e n o m e n a on the central nervous system. On occasions more t h a n one mechanism can be seen. Similar complications have been seen in p a t i e n t s having eosinophilia with a known cause 23.
Some of these c a s e s p r e s e n t a definite eosinophilic meningeal infiltration which justifies neurological s y m p t o m a t o l o g y . T h i s w a y of involvement h a s been described in relation to some infectious diseases such a s helminthiasis and more r a r e l y Coccidioidis immitis is, meningitis by l y m p h o m a s 14,16 an d in one case of disseminated glioblastoma
6 . On the c o n t r a y sometimes hypereosinophilic s y n d r o m e m a y be accompanied by neu-rological s y m p t o m s a n d eosinophilic pleocytosis in the C S F with pathological studies not revealing meningeal or p a r e n c h y m a t o u s infiltration 25. Even t h o u g h the patient p r e s e n t e d normal a m o u n t of eosinophils initially, w e m a y point out to the possibility t h a t such an eventuality might be evident d u r i n g w e e k s or m o n t h s despite the existence of s y m p t o m s 23. On the other h a n d , the p a t i e n t w a s receiving p r e d n i s o n e, a d r u g frequently used in t h e t r e a t m e n t of this g r o u p of affections 8,19,23) s h o w i n g a m a r k e d
a n d p r o g r e s s i v e increase in the number of eosinophils once this medication w a s stopped.
Nevertheless, most of these a g e n t s s h o w an i m p o r t a n t eosinophilic pleocytosis accomp a n y i n g the increase of eosinoaccomphils in accomp e r i accomp h e r a l blood with the exceaccomption of t o x o c a -riasis, which m a y not p r e s e n t such a c h a r a c t e r i s t i c in C S F 1 0
. Most n e m a t o d e s develop c a s e s of visceral larva m i g r a n s with systemic involvement. D i a g n o s i s is sometimes difficult due to low possibilities of visualizying l a r v a e in the lesions. On the other h a n d , m e t h o d s for a n t i b o d i e s detection may, in m a n y c a s e s , give c r o s s - r e a c t i o n s with other p a r a s i t e s having surface a n t i g e n s with similar s t r u c t u r e s . Histopathologically, they resemble g r a n u l o m a s or chronic inflammatory p h e n o m e n a in which the lacking of visualization of the l a r v a e t u r n s them completely u n s p e c i f i c
T o x o c a r i a s i s r e p r e s e n t s most common c a u s e for visceral larva m i g r a n s (VLM) with encephalic involvement Affectation of the n e r v o u s system is r e p r e s e n t e d by the formation of g r a n u l o m a s c o n t a i n i n g eosinophils which e x p r e s s themselves clinically by m e a n s of focal deficits, seizures or b e h a v i o u r a l d i s t u r b a n c e s . Ocular involvement is frequent, with p r o g r e s s i v e visual loss, s t r a b i s m u s a n d ocular pain. F u n d u s c o p y can s h o w isolated g r a n u l o m a s or exudative endophtalmitis. Ocular disease m a y be the only manifestation a n d sometimes it must be differentiated from r e t i n o b l a s t o m a . T h i s p a r a s i t o s i s , j u s t like o t h e r s previously mentioned, h a p p e n to s h o w
c o u n t s of white cells from 30000 t o 100000/mm3 with 50 t o 9 0 % of eosinophils. An increase in the titles of anti-A a n d anti-B a g g l u t i n i n s can be found, since the p a r a s i t e p r e s e n t s a surface a n t i g e n similar to h u m a n h e m a g g l u t i n i n s 3,12,21,22. P r e s e n c e of l a r v a e is r a r e l y detected in the feces and biopsies or n e c r o p s y tissues. Immunodiagnostic t e s t s with ELISA permit 7 8 % sensitivity and 9 9 % specificity 21. T h e illness is generally autolimited, in spite of eosinophils being able t o persist. It is possible t h a t some of t h e lesions might be p r o d u c e d by immune p h e n o m e n a , n o t w i t h s t a n d i n g t h a t this me-chanism w o u l d not r e p r e s e n t the most frequent genesis of the lesions observed in the n e r v o u s system 21.
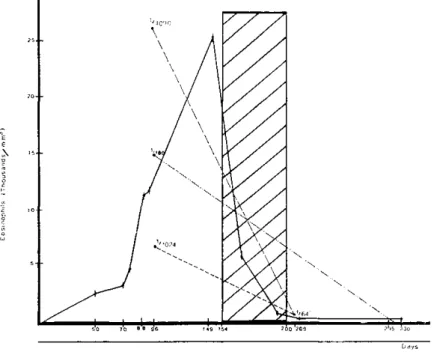
Normalization of eosinophils a b s o l u t e a n d relative counts, a s well a s the d e c r e -ment of anti-A a n d anti-B a g g l u t i n i n s levels after the empirical t r e a t m e n t with a wide s p e c t r u m a n t i p a r a s i t a r y d r u g (Fig. 4 ) g u i d e s the diagnosticai possibility of this case of chronic pachymeningitis t o w a r d s a p a r a s i t i c process, p e r h a p s s e c o n d a r y to an infection with Toxocara canis. T h e fact t h a t the larva w a s not identified in the feces nor in biopsies d o e s not d i s c a r d the d i a g n o s i s since, a s it w a s previously s t a t e d , this
Fig. 4 — Laboratory findings evolution: isoagglutinins; —• • —. .—, antimitocht
eventuality is extremely r a r e . Negativity of specific serology for t o x o c a r a might be due
to an e r r o r m a r g i n , r e p r e s e n t e d by a n u m b e r of false n e g a t i v e s which the study m e t h o
-dology p r e s e n t s . T h e presence of antimitochondrial antibodies could be h o m o l o g a t e d
to the findings performed by different a u t h o r s in relation t o cases of m u l t i p a r e n c h y m a
-tous g r a n u l o m a s , associated to Sjogren disease, sarcoidosis or p r i m a r y biliary cirrhosis,
in which such findings s u g g e s t a g r o u p of entities not yet correctly defined but with
the autoimmune p h e n o m e n a playing an i m p o r t a n t role 5>7. Antimitochondrial antibodies
negativation after a n t i p a r a s i t a r y t r e a t m e n t sets forth the possibility t h a t some of the
patients with elevated titles of them without an evident p a t h o l o g y migth c o r r e s p o n d
to a s y m p t o m a t i c p a r a s i t o s i s b e a r e r s
2. T h e pathological finding of a n o n c a s e o u s g r a n u
-lomatous process with meningeal involvement a n d l y m p h a d e n o p a t h i e s , even if it m a k e s
us consider sarcoidosis diagnosis, t h i s seems to be slightly p r o b a b l e due to the abscence
of associated thoracic involmement, lack of r e s p o n s e to steroids and the possibility
of a t t r i b u t i n g the histopathological findings to multiple etiologies 24 P r e s e n c e of
eosinophilic infiltrates m a k e s us finally consider this case a s a lesion caused by direct
cellular infiltration or t h r o u g h n e u r o t o x i n s a s it w a s a l r e a d y mentioned.
By w h a t h a s been s t a t e d , w e believe t h a t this case r e p r e s e n t s chronic p a c h y
-meningitis of a p r o b a b l e p a r a s i t a r y etiology. Nevertheless this c a n n o t be certainly
s t a t e d in a n a l o g o u s w a y a s it h a p p e n e d with other a u t h o r s 9.17, and it must be a d d e d
to other descriptions in which t o m o g r a p h i c findings similar to those observed in this
patient guide the d i a g n o s i s to tentorial pachymeningitis 17.
R E F E R E N C E S
1. A c k e r m a n S J , L o e g e r i n g DA, V e n g e P , Oisen I , H a r l e y J B , F a u c i AS, Gleich G J — D i s t i n c t i v e cationic p r o t e i n s of t h e h u m a n eosinophil g r a n u l e : m a j o r b a s i c p r o t e i n , eosinophilic c a t i o n i c p r o t e i n a n d e o s i n o p h i l d e r i v e d n e u r o t o x i n . J I m m u n o l 131 : 2977, 1983.
2. B a u m H, P a l m e r C — Significance of a n t i m i t o c h o n d r i a l a n t i b o d i e s . L a n c e t 2 : 1411, 1981. 3. B i a F J , B a r r y M — P a r a s i t i c infection of t h e c e n t r a l n e r v o u s s y s t e m . I n B o o s s J , T h o r n t o n G F (eds) : I n f e c t i o u s D i s e a s e s of t h e C e n t r a l N e r v o u s S y s t e m . N e u r o l o g i c Clinics Vol 4 No
1. S a u n d e r s , P h i l a d e l p h i a , 1986, p g 193-195.
4. C h u s i d M J , D a l e DC, W e s t BC, Wolff SM — T h e h y p e r e o s i n o p h i l i c s y n d r o m e : a n a l y s i s of f o u r t e e n c a s e s w i t h r e v i e w of t h e l i t e r a t u r e . Medicine 54 : 1, 1975.
5. Danzi J T — M u l t i o r g a n g r a n u l o m a s a n d m i t o c h o n d r i a l a n t i b o d i e s . N E n g l J Med 309 : 436, 1983.
6. D e f e n d i n i R, H u n t e r SB, S c l e s i n g e r E B , L e i f e r E , R o w l a n d L P — E o s i n o p h i l i c m e n i n g i t i s in a case of d i s s e m i n a t e d g l i o b l a s t o m a . A r c h N e u r o l 38 : 52, 1981.
7. F a g a n EA, MooreGillon J C , T u r n e r W a r w i c k M — M u l t i o r g a n g r a n u l o m a s a n d m i t o -c h o n d r i a l a n t i b o d i e s . N E n g l J Med 308 : 572, 1983.
8. F a u c i AS, H a r l e y J B , R o b e r t s WC, F e r r a n s B J , G r a u n i c H R , B j o r n s o n B J — T h e i d i o p a t h i c h y p e r e o s i n o p h i l i c s y n d r o m e : clinical, p a t h o l o g i c a l , a n d t h e r a p e u t i c c o n s i d e -r a t i o n s . A n n I n t e -r n Med 97 : 78, 1982.
9. F e r i n g a E R , W e a t h e r b e e L — H y p e r t r o p h i c g r a n u l o m a t o u s c r a n i a l p a c h y m e n i n g i t i s c a u s i n g p r o g r e s s i v e b l i n d n e s s in a c h r o n i c d i a l y s i s p a t i e n t . J N e u r o l N e u r o s u r g P s y c h i a t 38 : 1170, 1975.
10. F o x AS, K a z a c o b K R , Gould N S , H e y d e m a n P T , T h o m a s C, B o y e r K M — F a t a l eosinophilic m e n i n g o e n c e p h a l i t i s a n d v i s c e r a l l a r v a m i g r a n s c a u s e d b y t h e r a c o o n a s c a r i d . N E n g l J Med 312 : 1619, 1985.
11. G a r d n e r - T h o r p e C, H a r r i m a n D G F , P a r s o n M — L o e f f l e r ' s eosinophilic e n d o c a r d i t i s w i t h B a l i n t ' s s y n d r o m e (optic a t a x i a a n d p a r a l y s i s of v i s u a l f i x a t i o n ) . Q u a r t J Med 158 : 249, 1971.
13. Hardy WR, Anderson R E — The hypereosinophilic syndrome. Ann Intern Med 68:1220, 1968.
14. Hollister D, Clements M, Colerman M, P e t i t o F — Eosinophilic meningitis in Hodgkin's d i s e a s e : report of a case and review of the literature. Arch Intern Med 143:590, 1983. 15. K a w a m u r a J, Yoshiaki K, Nobuyuki O — Eosinophilic meningoradiculomyelitis caused
by Gnasthostoma spinigerium: a case report. Arch Neurol 40:583, 1983.
16. K i n g DK, Loh KK, Ayala AG — Eosinophilic meningitis and lymphomatous meningitis. Ann Intern Med 82:228, 1975.
17. Kobayashi N, H o n g o K, Kawauchi M, K o b a y a s h i M, Sukita K — Chronic m e n i n g i t i s with marked unilateral tentorial pachymeningitis. Surg Neurol 23:529, 1985.
18. Kuberski T — Eosinophils in the cerebrospinal fluid. Ann Intern Med 91:70, 1979. 19. Moore P M , H a r l e y J B , F a u c i AS — N e u r o l o g i c d y s f u n c t i o n in t h e i d i o p a t h i c h y p e r - e o - ¬
s i n o p h i l i c s y n d r o m e . A n n I n t e r n Med 102 : 109, 1985.
20. R o n g x u n Z — C h r o n i c a r a c h n o i d i t i s in t h e p o s t e r i o r f o s s a : a s t u d y of 82 cases. J N e u r o l N e u r o s u r g P s y c h i a t 45 : 598, 1982.
21. S c h a n t z P M , G l i c k m a n L T — C u r r e n t c o n c e p t s in p a r a s i t o l o g y : t o x o c a r a l visceral l a r v a m i g r a n s . N E n g l J Med 298 : 436, 1978.
22. S m i t h H V , K u s e l J R , G i r d w o o d R W A — T h e p r o d u c t i o n of h u m a n A a n d B blood g r o u p like s u b s t a n c e b y in v i t r o m a i n t e d second s t a g e T o x o c a r a canis l a r v a e : t h e i r p r e s e n c e on t h e o u t e r l a r v a l s u r f a c e s a n d in t h e i r e x c r e t i o n s / s e c r e t i o n s . Clin E x p I m u n o l 54 : 625, 1983.
23. S p r y C J F , D a v i e s J , T a i P C , Olsen O G J , O a k l e y CM, Goodwin J F — Clinical f e a t u r e s of fifteen p a t i e n t s w i t h t h e h y p e r e o s i n o p h i l i c s y n d r o m e . Q u a r t J Med 205 : 1, 1983. 24. S t e r n B J , K r u m h o l z A, J o h a s C, Scott P , Missoni J — S a r c o i d o s i s a n d i t s n e u r o l o g i c a l
m a n i f e s t a t i o n s . A r c h N e u r o l 42 : 909, 1985.