SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Stand-alone
anterior
lumbar
interbody
fusion
–
complications
and
perioperative
results
夽
Rodrigo
Amaral
a,
Ronaldo
Ferreira
a,
Luis
Marchi
a,∗,
Rubens
Jensen
a,
Joes
Nogueira-Neto
a,
Luiz
Pimenta
a,baInstitutodePatologiadaColuna(IPC),SãoPaulo,SP,Brazil
bUniversityofCaliforniaSanDiego(UCSD),SanDiego,UnitedStates
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received18August2016 Accepted6September2016 Availableonline4September2017
Keywords: Spine Spinalfusion Arthrodesis Lumbarvertebrae
a
b
s
t
r
a
c
t
Objectives: Historically,anteriorlumbarinterbodyfusion(ALIF)wasrelated tohighrates ofintraoperativecomplicationsandadverseeventsrelatedtointerbodydevices.Inrecent decades,therehavebeentechnical adjustments,andcagesthataremoresuitablehave emerged.Theaimofthisstudyistoevaluatetheefficacyandcomplicationrateoftheuse ofstand-alonemini-ALIFusingaself-lockingcage.
Methods:Retrospective single centerstudy. Inclusion criteria:retroperitoneal mini-ALIF forsingle-levelfusion(L5S1);self-lockingcage;DDD/stenosisandgradeI spondylolisthe-sis.Exclusioncriteria:posteriorsupplementation,previousfusion/arthroplasty.Endpoints: surgerydata,intraoperativeandperioperativeadverseeventsrelatedbothtosurgicalaccess andtotheintersomaticdevice.
Results:Eighty-sevencaseswereenrolled.Mediansurgicaltimewas90min;medianblood losswas100mL.ThemedianlengthofstayintheICUwaszerodays;medianhospitalstay wasoneday.Tencaseshadanadverseevent(11.5%):fourmajoradverseevents(4.6%;3L bleeding;DVT;retroperitonealhaematoma;incisionalhernia),andsevenminorevents(8%; peritoneuminjury;minorvascularinjury;eventsrelatedtothecage).Nocasesofretrograde ejaculationwereobserved.Therewasimprovementinpain,physicalrestriction,andquality oflife(p<0.001).
Conclusions: Themini-ALIFprocedureperformedforsingle-levelfusionatthedistallumbar leveldemonstratedlowadverseeventratesrelatedtoboththesurgicalapproachandto theintersomaticdevice,withreducedhospitalstayandsatisfactoryperioperativeclinical results.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
PaperdevelopedattheInstitutodePatologiadaColuna(IPC),SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](L.Marchi).
http://dx.doi.org/10.1016/j.rboe.2017.08.016
Palavras-chave: Colunavertebral Fusãoespinal Artrodese
Vértebraslombares
Objetivos: Historicamente,afusãointersomáticalombaranterior(ALIF)esteverelacionada aaltastaxasdecomplicac¸õesintraoperatóriaseeventosadversosrelacionadosaos dispos-itivosintercorporais.Nasúltimasdécadas,ocorreramajustestécnicosquepropiciaramo surgimentodecagesmaisadequadas.Esteestudotevecomoobjetivoavaliarascomplicac¸ões eeficáciadousodeviaúnicapormini-ALIFcomusodecageautobloqueante.
Métodos: Estudoretrospectivodecentroúnico.Critériosdeinclusão:mini-ALIF retroperi-toneal para a fusão de nível único (L5S1); cage autobloqueante; DDD/estenose e espondilolistesede baixograu(grauI).Critérios deexclusão: suplementac¸ãoposterior; fusão/artroplastiaprévia.Foramanalisadosdadosdecirurgia,complicac¸õesintrae peri-operatóriasrelacionadasaoacessocirúrgicoeaodispositivointersomático.
Resultados: Foramincluídos87casos,todosnonívellombardistal.Medianadetempo cirúr-gico: 90min;mediana deperdasanguínea:100mL.Amedianadotempodeinternac¸ão na UTI foi zero dia; a mediana de internac¸ão hospitalar foi de um dia. Dez casos (11,5%)apresentarameventosadversos,quatromaiores(4,6%;sangramentode3L;TVP; haematoma retroperitoneal; hérnia incisional) e sete menores(8%; lesão de peritônio; lesãovascularmenor;ocorrênciasrelacionadasaoimplante).Nenhumcasodeejaculac¸ão retrógrada foi observado. Houve melhoriaem dor,restric¸ão física equalidade de vida (p<0,001).
Conclusões: O procedimento mini-ALIF feito em um único nível distal lombar apre-sentou baixas taxas de eventos adversos intra e perioperatórios, tanto quanto à abordagem e ao dispositivo, reduzida estada hospitalar e bons resultados clínicos perioperatórios.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Lumbar interbody fusion canbe performed through differ-ent accesses (anterior,anterolateral,lateral, transforaminal and posterior). The advantages of the anterior approach (anterior lumbar interbody fusion, ALIF) include the pos-sibility of disc space re-expansion, lumbar lordosis recov-ery, indirect decompression, prevention of damage to posterior structures (paravertebral and osteoligamentous muscle) and morbidity and immediate perioperative pain reduction.1–5
Theanteriorinterbodylumbarfusiontechniquewas ini-tiallyusedbyBurns6andCapener,7developedasoneofthe predominanttechniquesforthetreatmentofdiscogenic lum-barpain.Historically, ALIFhasbeenlinkedtohighratesof intraoperativecomplications,becauseofthetransperitoneal pathwayandadverseeventsrelatedtofusiondevicesdueto lackofadequatecages.8–10
Recently, with the adaptation of surgical access tech-niques and better interbody devices, it has been possible to obtain satisfactory rates of complications and high fusion rates.11 Thus, it may be advantageous to perform arthrodesiswithadequatecagesbyalesstraumaticanterior approach.
Theobjective ofthe present study was to evaluatethe complicationsandperioperativeresultsofmini-ALIFanterior
stand-alone interbody fusion surgery withthe use of self-lockingcageatL5S1level.
Materials
and
methods
Thisisaretrospectivestudywithdatacollectedprospectively fromasinglemedicalcenter.Itwassubmittedtoandapproved by the Research Ethics Committee (52909516.3.0000.5551). PatientsselectedhadundergoneALIFtechniquebythesame spine surgeryteamfrom 2009to2016.Inclusion: retroperi-tonealmini-ALIFforsingle-levelfusion;self-lockingALIFcage; degenerative disc disease (DDD, withor without stenosis), orlowgradespondylolisthesis(gradeI).Exclusion:posterior oranterioradditionalsupplementation;fusion/prior arthro-plasty; cages with angulation greater than 15 degrees of lordosis.
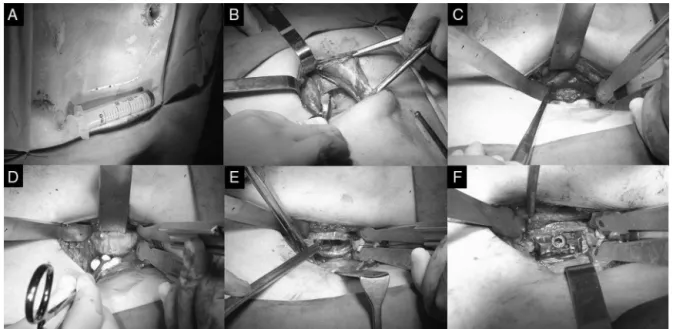
Fig.1–ImagesrepresentinganteriorretroperitonealaccesstotheL5-S1discspace.(A)Abdominalincision;(B)passage throughtheabdominalmuscles;(C)identificationofthebifurcationofthegreatvesselsinfrontofthediscspaceofL5S1;(D) exposureoftheanteriorfaceoftheintervertebraldisc;(E)discectomyandpreparationofthediscspaceforarthrodesisand (F)interbodyimplantsecuredwithlockingscrewsintothediscspace.
analyzedintheperioperativeperiodanduptothreemonthsof follow-up.
Surgicaltechnique
Themodernsurgicaltechniqueofananterioraccesswiththe useofabluntpassagethroughtheabdominalmusculature, retroperitonealsurgicalapproach,anddirectviewtoaccess theL5S1discspacehasbeencalledmini-ALIF.Thepatientis placedinasupinepositiononastandardradiolucent surgi-caltable.Thedegreeoflumbarlordosisshouldbeobserved, andapadplacedunderthepatientatthelevelofthelumbar spinetoraiseit,whichnotonlyopenstheanteriorspaceto facilitatediscectomybutalsoallowseasierplacementofthe implantwithsomedegreeofangulation(lordosis).Allpatients underwenttheanteriorapproachtothelumbosacralspine.A mini-PfannenstielincisionwasusedtoaccessL5-S1level.
Bluntdissectionisusedtomobilize the anteriorsheath of the rectus abdominis muscle to access the retroperi-tonealspace.Palpationoflargevesselshelpspreventvascular lesions.Theuretershouldbeidentifiedtoavoidits inadver-tentdamage,andthisistypicallyfoundontheperitonealside oftheexposure.
Autostaticretractorsaredeeplyplaced,andattachedtoa deviceassembledonthesurgicaltabletokeeptheviewofthe spineinmidline.Theuseofcurare-likedrugsfacilitates expo-sureandensurescorrectpositioningoftheretractors.Forthe exposureofL5-S1space,thedisccanbenormallyaccessed belowthebifurcationofthelargevessels.Thetransverse seg-mentalarteriestothediscspaceorthearterialbranchesofthe aortaneedtobesecurelyligated.Iliolumbarveinscanalsobe thecauseofproblemsrelatedtobleeding.Themediansacral arteryanditsveinneedtobeligatedtoallowaccessbelowthe bifurcation.
Theexcessiveuseofelectrocauteryalongtheanterior lon-gitudinalligamentmustbeavoidedtopreventsympathetic hypogastricplexusinjury,whichmayresultinretrograde ejac-ulation. Theanterior longitudinalligament is thenopened withascalpel,andthecompleteremovaloftheintervertebral discwithcurettesisperformed.Theposteriorlongitudinal lig-amentismaintainedandthelateralringportionsareopened to the level that allows insertion of the interbody spacer implants.Followingextensivediscectomyandremovalofthe endplate,theintervertebralimplantsareimpactedand lock-ingscrewsarepassedthroughthecagestowardstheadjacent vertebralbodies.Illustrativeimagesofthesurgicalprocedure areshowninFigs.1and2.
Results
Weanalyzed 87cases (50female individuals,mean age 44 years,meanBMI26.6kg/m2).Allcaseswereatthemostdistal lumbarlevel(L5S1orbetweenL5/L4andtransitionalvertebra). ThedataofthestudiedgroupareshowninTable1.Average casefollow-upwas46monthsaftersurgery(minimum3and maximum84months).
Informationregardingthesurgicalprocedureand hospi-taladmissionareshowninTable2.Meansurgicaltimewas 98min(SD 24; 40–150); medianblood loss100mL (SD 455; 50–3000);meantimeofadmissioninanICUwaszeroday(SD 0.3;0–1);medianhospitalstayofoneday(SD0.6;1–3).
Fig.2–Imagesofintraoperativefluoroscopyshowingfinalpositioningoftheinterbodyspacer.(A)Lateralviewand(B) anteroposteriorviewevidencingthetitaniumspacerandthelockingscrewstowardstheadjacentvertebralbodies.
Table1–Demographicandpreoperativedata.
Total(n) 87
Age(years) 44±11
Gender(female) 50(64%)
BMI(kg/m2) 26.6±4.1
Levelstreated 87
Discdegenerativedisease 45(51%)
DDD+stenosis 19(22%)
Spondylolisthesis 16(18%)
Postdiscectomy 8(9%)
L5S1 81(93%)
L4TV 2(2%)
L5TV 4(4%)
BMI,bodymassindex;DDD,discdegenerativedisease.
Valuesshowninmedian±standarddeviationorinabsolute num-ber(andpercentage).
Table2–Surgicalandperioperativedata.
Duration 90(98)±24min
Bloodloss 100(171)±455mL
ICUadmission 0(0.2)±0.2dia
Hospitaladmission 1.5(1.6)±0.6dia
Valuesshowninmedian(mean)±standarddeviation.
controlledlesion).Postoperativeeventswereone(1.1%)deep veinthrombosis,one(1.1%)retroperitonealhaematoma (addi-tional surgery required for drainage), one (1.1%) incisional hernia (requiredsurgical repair),and one (1.1%)superficial intraoperativewoundinfection.Therewasnocaseof retro-gradeejaculationinthisseries.Regardingthetwocases(2.3%) ofpostoperativeeventsrelatedtotheimplant,wereportone caseofsinkingandoneofpoorpositioning.Nocasesof expul-sionormigrationoftheimplantwereobserved.Therewereno casesofdeath.
Short-termclinicalresultsshowedastatisticallysignificant clinical improvement inthe cases treated. Pain symptoms
Table3–Adverseevents.
INTRAOP Vascular
Venousdamage(1a) 2(1a) 2%
Arterialdamage 0 0%
Accidentalopeningoftheperitoneum 2 2%
Viscerallesion 0 0%
PERIOP Infection
Superficial 1 1%
Deep 0 0%
DVTa 1a 1%
Retroperitonealhematomaa 1a 1%
Incisionalherniaa 1a 1%
Retrogradeejaculation 0 0%
Implant 2 2%
TOTAL 10 11%
Majoradverseevents 4 5%
Minoradverseevents 7 8%
Valuesshowninabsolutenumbersandpercentage.
a Majoradverseevents.
Table4–Short-termclinicalresults.
Preop 1week 6weeks 3months
BackVAS 7.4 4.0a 3.7a 4.2a
LowerlimbsVAS 5.1 3a 2.9a 2.8a
ODI 44 39 34a 31a
EQ-5D 0.59 0.65 0.70a 0.76a
Valuesshowninmean.
a Statisticallylowerthanthepreoperativevalue.
improvementinsymptomsirradiatedtothelowerlimbs.The ODIscaleshoweda30%improvementinphysicalrestraint, anda29%improvementinqualityoflife.
Discussion
Thisstudy evaluated theuse ofthe mini-ALIF stand-alone approachregardingitscomplicationsanditsintraand peri-operativeresults.An11%rateofadverseevents(minorand major) with only 4% of major adverse events was found, whichresultedinreducedhospitalstay(average1.6days)and improvementofpainafteraweekofsurgery.Itisworth men-tioningthatthepresentstudy analyzedonlycaseswithout previousarthrodesisorinterbodysurgery,andonlyinthelast mobilelevel ofthespine(L5S1);this isthetechnically less challenginglevel,withfasteraccess(about20min)andthat potentiallyleadstofewercomplications.12
Theoverloadofsegmentsadjacenttoafusionisduetopoor alignmentinthesagittalplane,13proceduresthatcause pos-teriordestabilization(damage tothe paravertebralmuscles andosteoligamentarystructures),14andviolationoftheupper articularfacetsbytheshaftandscrews(kickingspine).15The stand-aloneoption (withno furthersupplementation)with onlyimpactedorthreadedcagesinthediscspacehasshown manyflawsinthehistoryofspinalsurgery.8,16Currently,the traditionaloptionsforinstrumentationinALIFshortfusions are cage and transpedicular screws or cage and anterior plate.
The most modern form of instrumentation in ALIF is the stand-alone option with self-locking cages. The great advantage of this option would be the possibility to per-form the procedure through an anterior approach, in a stand-alone procedure, without injury or iatrogenesis of the posterior elements of the spine. Thus, the procedure becomesless invasiveand allowsthe patient the opportu-nityoflowperioperativemorbidityandrapidpostoperative mobilization.1,17
Unliketheoldstand-aloneoption,self-lockingspacersnow provideverysatisfactorybiomechanicalstability,with charac-teristicsthataresimilartoconstructionwithtranspedicular screws15,18,19 and different from only impacted cages.20 Obviously,theuseofthestand-aloneoptionshouldbe recom-mendedforlessunstablelumbarlevels,itmayeveninclude spondylolisthesis,21–24 butincaseswithbonefailures(such asparslysis),theymaygenerateanabnormalmovement,and resultinarthrodesisfailure.25
ThedisadvantagesofALIFarerelatedtopossibleadverse eventsrelatedtoperitonealandretroperitonealstructures.In Brazilandinothercountriestheaccesstotheintervertebral discinanALIFisusuallyobtainedbyanaccesssurgeon (gen-eralorvascularsurgeon)26inordertoreducethepossibilityof intraandperioperativecomplications.However,thispractice isnotmandatoryanddependsonwhetherthesurgeonhas thetrainingandtheabilitytodoso.Historically,theEuropean schoolofspinesurgeryhasabasictrainingforanterioraccess surgeries,27andtheAmericanschoolisbeginningtoembark onthispractice.ThisfactisevidencedbyJarretetal.28inan articlethatevaluatestheincidenceofcomplicationsinthe presenceorabsenceofaccesssurgeonsinspinesurgeries.No
differenceswereobserved.Thisshowsthatitdependsaloton thespinesurgeon’sexperienceandtraining.
Thevascularlesionsarepotentiallyamongthemostsevere intraoperativecomplications.Theyare consideredtobethe mostdevastatingcomplicationswithaninjuryratereported intheliteratureof1–40%,12,26,27,29dependingonthe experi-enceofthegroupandthetypeofcasetreated;occurrences atL4L5levelaremorefrequent.30Inthisstudy,withaccess onlytoL5S1,wenoted2.3%ofvascularlesionsobserved dur-ingsurgery,andprobablyonemoreeventnotobservedduring the procedure(total3.4%),but thatled toaretroperitoneal haematomanoticedsomedaysaftersurgery.Arteriallesions occurlessfrequentlythanvenouslesions,andthemost com-montypesofvascularinjuryarelacerationoftheiliacvein, inferiorvenacavaandileolumbarvein.Notallvascularlesions aresevere,andsomeofthemcanbesimplysolvedduringthe procedure, asweobservedwithminorlesionsinourstudy. InthearticlebyQuraishietal.,27inwhichtherewere24/304 (7.8%)vascularproblemsofdifferentmagnitudes,9/304(3% ofthetotalor38%ofthelesions)thepresenceofavascular surgeonwasrequired.
Someattitudescanhelpavoidinginjuries,suchastheuse ofacurvedhaemostaticforcepswithasmallpieceofgauze or cotton woolon its tip. Thisforceps isused atthe time ofdissectionoftheanteriorlongitudinalligamentanddisc, forbettervisualizationofthediscspace.Themediansacral arteryandveinaredividedwithvascularclips,orligated.12 Oneofthepossibleadverseeventsisthatofretrograde ejac-ulationifthereisupperhypogastricplexusinjury.Although being feared, the reportedincidenceis low,as observedin thisstudyandintheliterature,0.1–8%ofthecases, depend-ing onthe techniqueused.12Withamorerefinedexposure technique,andcurrentlylessuseofelectrocautery,therateof retrogradeejaculationisthelowestobservedinthehistoryof spinalsurgery.Althoughpossible,incisionalherniasarerare complicationsifameticulousclosureinplanesisperformed afterthemini-ALIF.12
Conclusion
The procedure oflumbar interbody arthrodesisata single lumbardistallevelviaananteriormini-openaccess demon-stratedlowratesofadverseevents,bothregardingthesurgical approach and the interbody device. Theperioperativedata showedashorterhospitalization,rareuseofICU,and good improvement of clinical parameters and quality of life. A surgicalgroupwithprofessionalswithaccessexperienceis necessarytokeepthereproducibilityofthesurgicalprocedure.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
2015;15(5):817–24.
3. KimJS,KangBU,LeeSH,JungB,ChoiYG,JeonSH,etal. Mini-transforaminallumbarinterbodyfusionversusanterior lumbarinterbodyfusionaugmentedbypercutaneouspedicle screwfixation:acomparisonofsurgicaloutcomesinadult low-gradeisthmicspondylolisthesis.JSpinalDisordTech. 2009;22(2):114–21.
4. StrubeP,HoffE,HartwigT,PerkaCF,GrossC,PutzierM. Stand-aloneanteriorversusanteroposteriorlumbar interbodysingle-levelfusionafterameanfollow-upof 41months.JSpinalDisordTech.2012;25(7):362–9.
5. UribeEV,AmaralR,MarchiL,JensenR,OliveiraL,ForttiF, etal.Immediatereciprocalchangesatadjacentlevel
followingsingle-levelALIF.Coluna/Columna.2015;14(4):286–9.
6. BurnsB.Anoperationforspondylolisthesis.Lancet. 1933;1:1233.
7. CapenerN.Spondylolisthesis.BrJSurg.1932;19(75):374–86.
8. DennisS,WatkinsR,LandakerS,DillinW,SpringerD. Comparisonofdiscspaceheightsafteranteriorlumbar interbodyfusion.Spine(PhilaPa1976).1989;14(8):876–8.
9. SamudralaS,KhooLT,RhimSC,FesslerRG.Complications duringanteriorsurgeryofthelumbarspine:ananatomically basedstudyandreview.NeurosurgFocus.1999;7(6):e9.
10.ChoiJY,SungKH.Subsidenceafteranteriorlumbarinterbody fusionusingpairedstand-alonerectangularcages.EurSpine J.2005;15(1):16–22.
11.ZhangJ,PoffynB,SysG,UyttendaeleD.Arestand-alonecages sufficientforanteriorlumbarinterbodyfusion?OrthopSurg. 2012;4(1):11–4.
12.BrauSA.Mini-openapproachtothespineforanteriorlumbar interbodyfusion:descriptionoftheprocedure,resultsand complications.SpineJ.2002;2(3):216–23.
13.AkamaruT,KawaharaN,TimYoonS,MinamideA,SuKimK, TomitaK,etal.Adjacentsegmentmotionafterasimulated lumbarfusionindifferentsagittalalignments:a
biomechanicalanalysis.Spine(PhilaPa1976). 2003;28(14):1560–6.
14.BisschopA,HolewijnRM,KingmaI,StadhouderA, VergroesenP-PA,vanderVeenAJ,etal.Theeffectsof single-levelinstrumentedlumbarlaminectomyonadjacent spinalbiomechanics.GlobSpineJ.2015;5(1):39–48.
15.PatelRD,GrazianoGP,VanderhaveKL,PatelAA,GerlingMC. Facetviolationwiththeplacementofpercutaneouspedicle screws.Spine(PhilaPa1976).2011;36(26):E1749–52.
16.BeutlerWJ,PeppelmanWC.Anteriorlumbarfusionwith pairedBAKstandardandpairedBAKproximitycages: subsidenceincidence,subsidencefactors,andclinical outcome.SpineJ.2003;3(4):289–93.
17.UdbyPM,Bech-AzeddineR.Clinicaloutcomeofstand-alone ALIFcomparedtoposteriorinstrumentationfordegenerative
fusion:stand-aloneinterbodycageversusinterbodycage withpediclescrewfixation–afiniteelementanalysis.BMC MusculoskeletDisord.2013;14:220.
19.CainCMJ,SchleicherP,GerlachR,PflugmacherR,ScholzM, KandzioraF.Anewstand-aloneanteriorlumbarinterbody fusiondevice:biomechanicalcomparisonwithestablished fixationtechniques.Spine(PhilaPa1976).2005;30(23):2631–6.
20.ChoCB,RyuKS,ParkCK.Anteriorlumbarinterbodyfusion withstand-aloneinterbodycageintreatmentoflumbar intervertebralforaminalstenosis:comparativestudyoftwo differenttypesofcages.JKoreanNeurosurgSoc.
2010;47(5):352–7.
21.IshiharaH,OsadaR,KanamoriM,KawaguchiY,OhmoriK, KimuraT,etal.Minimum10-yearfollow-upstudyofanterior lumbarinterbodyfusionforisthmicspondylolisthesis. JSpinalDisord.2001;14(2):91–9.
22.RaoPJ,GhentF,PhanK,LeeK,ReddyR,MobbsRJ.Stand-alone anteriorlumbarinterbodyfusionfortreatmentof
degenerativespondylolisthesis.JClinNeurosci. 2015;22(10):1619–24.
23.OliveiraL,MarchiL,CoutinhoE,PimentaL.Standalone anteriorinterbodyfusionprocedureforthetreatmentof low-gradespondylolisthesis:acaseseries.SciWorldJ. 2012;3(1):194–200.
24.RaoPJ,LoganathanA,YeungV,MobbsRJ.Outcomesof anteriorlumbarinterbodyfusionsurgerybasedonindication: aprospectivestudy.Neurosurgery.2015;76(1):7–23.
25.LastfogelJF,AltstadtTJ,RodgersRB,HornEM.Sacralfractures followingstand-aloneL5-S1anteriorlumbarinterbodyfusion foristhmicspondylolisthesis.JNeurosurgSpine.
2010;13(2):288–93.
26.MobbsRJ,PhanK,DalyD,RaoPJ,LennoxA.Approach-related complicationsofanteriorlumbarinterbodyfusion:resultsof acombinedspineandvascularsurgicalteam.GlobSpineJ. 2016;6(2):147–54.
27.QuraishiNA,KonigM,BookerSJ,ShafafyM,BoszczykBM, GrevittMP,etal.Accessrelatedcomplicationsinanterior lumbarsurgeryperformedbyspinalsurgeons.EurSpineJ. 2013;22Suppl.1:S16–20.
28.JarrettCD,HellerJG,TsaiL.Anteriorexposureofthelumbar spinewithandwithoutan“accesssurgeon”:morbidity analysisof265consecutivecases.JSpinalDisordTech. 2009;22(8):559–64.
29.IkardRW.Methodsandcomplicationsofanteriorexposureof thethoracicandlumbarspine.ArchSurg.
2006;141(10):1025–34.