Arq. Bras. Cardiol. vol.98 número4 en v98n4a13
Texto
Imagem
Documentos relacionados
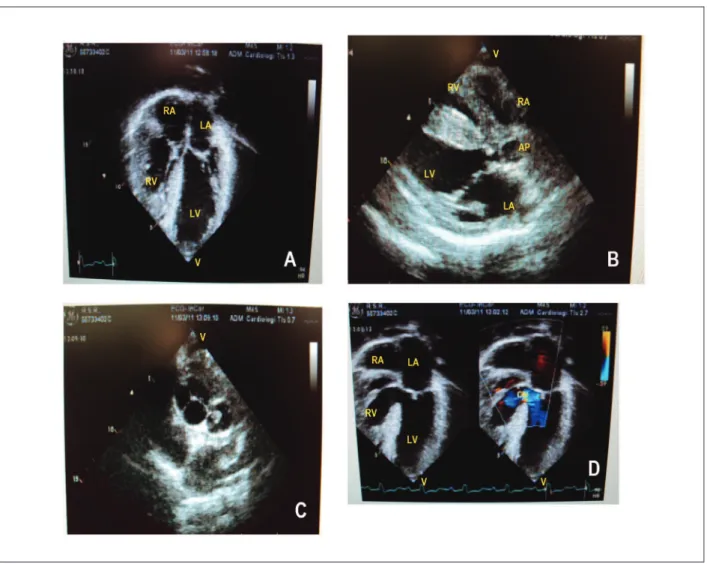
An 11-year-old female, 24.9 kg, with a diagnosis of transposition of great arteries with hypoplastic left ventricle and pulmonary stenosis, who underwent atrial septostomy
ches in the preoperative period, association with atrioventri- cular septal defect or agenesis of the pulmonary valve, significant residual ventricular septal defect, residual
In this study, we assessed the clinical evolvement, the echo- cardiographic, cineangiographic, and surgical characteristics of children with perimembranous ventricular septal defect
Based on the analysis of the cineangiocardiographic studies of patients with pulmonary atresia, ventricular septal defect, and aorto- pulmonary collateral arteries (group B),
Our management for patients with transposition of the great arteries with intact ventricular septum was to indicate systematic primary anatomic correction in all patients in
Clinical fi ndings strongly suggest the diagnosis of pulmonary atresia with ventricular septal defect because of the presence of an early systolic click in the aortic area and
The connection between the pulmonary arteries and the right ventricular outflow tract (RVOT) in pulmonary atresia (PA) with ventricular septal defect (VSD) may be corrected
Clinical findings are consistent with the diagnosis of atrial septal defect, considering the split second heart sound, the soft murmur in the pulmonary area, the right
