Int J Anat Res 2014, 2(4):633-35. ISSN 2321-4287 633
Original Article
STUDY ON NECK SHAFT ANGLE AND FEM ORAL LENGTH OF SOUTH
INDIAN FEM URS
Shakil M ohamad Khan
1, Shaik Hussain Saheb *
2.
ABSTRACT
Address for Correspondence: Shaik Hussain Saheb,Assistant Professor, Depart ment of Anat omy, JJM M edical College, Davangere, Karnataka - 577004, India. E-M ail: anat [email protected]
Access this Article online
Quick Response code Web site:
1Assistant Professor, Depart ment of Ort hopedics, JJM M edical College, Davangere, Karnataka, India
* 2 Assistant Professor, Depart ment of Anat omy, JJM M edical College, Davangere, Karnataka, India.
Background: Fem oral nek ant eversion describes t he angle subt ended by t he fem oral neck w it h reference t o t he t ranscondylar plane of t he distal end of t he fem ur and is usually 15° t o 45°. This along w it h t he neck shaft angle, hip axis lengt h, fem oral neck w idt h inf luence t he risk of fem oral neck fract ure. Fem oral neck ant eversion angle has t o be t aken int o considerat ion w hen reduct ion and fixat ion is select ed as a m et hod of t reat m ent .
Objectives: The object ives of present st udy t o f ind out t he m easurem ent s of Neck shaft angle, Fem oral Lengt h and Neck Lengt h of fem ur.
M aterials and M et hods: In present st udy have used 250 fem urs from different colleges in sout h India. The follow ing m easurem ent s w ere conduct ed Neck shaft angle, Fem oral Lengt h and Neck Lengt h of fem ur.
Result s: Th e r esult s o f presen t st u dy are t he len gt h o f f em ur w as 446.2 +26.39m m , r ight fem ur w as 446.6+26.66m m and left fem ur w as 445.8+26.12m m , t he Neck Lengt h fem ur w as 36.3+4.2m m , right fem ur w as 36.1+4.1m m and lef t fem ur w as 36.4+4.3m . t he neck shaft angle of fem ur w as 137.10 , r ight fem ur w as
137.30 and left fem ur w as136.90.
Conclusion:There is no significance difference bet w een right and left fem ur m easurem ent s. Ort hopaedist s and Radiologist s use t he norm al range and m eans of t he neck shaft angle in t he diagnosis and t reat m ent of t he disease of t he hip. The angle is increased in congenital subluxat ion and dislocat ion of t he hip, poliom yelit is, cerebral palsy and idiopat hic scoliosis and decreased in t he congenital coxavara , post t raum at ic coxa vara due t o m alunit ed fem oral neck and int er t rochant er ic fract ures.
KEY W ORDS:Fem oral Lengt h, Neck Lengt h, Neck Shaft angle and Fem ur.
INTRODUCTION
Int ernat ional Journal of Anatomy and Research, Int J Anat Res 2014, Vol 2(4):633-35. ISSN 2321- 4287 DOI: 10.16965/ ijar.2014.512
Received: 01 Oct 2014
Peer Review : 01 Oct 2014 Published (O):31 Oct 2014 Accepted: 15 Oct 2014 Published (P):31 Dec 2014
Internat ional Journal of Anat omy and Research ISSN 2321-4287
w w w.ijmhr.org/ ijar.ht m
Anat omical st udy of femur bone serves helpful data t o understand different aspect of clinical disease condit ions, including com mon sit e of fract ure, changes in osteoporosis, associated congenit al anom alies as w ell as m edicolegal cases. The femur is t he longest & st rongest bone in t he body. Its lengt h is associated w it h a st riding gait , it s st rengt h w it h t he w eight and muscular forces which it must withstand. It s shaft is almost cylindrical. It has a proximal rounded art icular head project ing medially from it s short neck.
The femoral neck lengt h is approximately 5cm long and connect s t he head t o shaf t at an average angle of 135o. This angle facilit at es
movement s at t he hip joint , enabling t he limb t o sw ing clear of t he pelvis[1].
Ost eoporosis is generally considered t o be a condit ion affect ing w omen, but up t o 30% of fragilit y fract ures occur in men. The lifet ime risk of fract ure at t he age of 50 years has been est im at ed t o be 20% for m en. Bone m ineral d ensi t y h as l o ng b een reco gn i sed as an important skelet on determinant of fract ure risk,
Int J Anat Res 2014, 2(4):633-35. ISSN 2321-4287 634 Shakil M ohamad Khan, Shaik Hussain Saheb. STUDY ON NECK SHAFT ANGLE AND FEM ORAL LENGTH OF SOUTH INDIAN FEM URS.
M ATERIALS AND M ETHODS
RESULTS b ut i t is b eco m i ng ap parent t hat skelet al
geomet ry also influences t he risk. This has been most extensively st udied in w omen at t he hip, in terms of hip axis lengt h , femoral neck axis lengt h , neck shaft angle and femoral neck w idth. The role of all of t hese fact ors as independent predict ors of hip fract ure risk is cont roversial in bot h sexes, w it h st udies giving conflicting results. This uncertaint y may have arisen part ly because of dif ferences in st udy design, num bers of pat ient s st udied, and also because of w ide variat ions in geomet ric parameters in different count ries and races. Given t his variat ion, it may be necessary t o generat e data specific t o t he populat ion under considerat ion. According t o st udy of S. P. Tuck et al, show ed t hat men had a mean femoral NSA of 1300%+ 3.3, range 121–
1380%, w hilst w omen had a significant ly smaller
mean femoral neck shaft angle of 1280% + 1.7,
range 119–1370%[2].
The neck shaft angle varies wit h age, stature and w idth of pelvis. When t his angle >135 o, condit ion
is know n as coxavalga. When angle <120 o, it is
know n as coxa vara. The angle of femoral neck is reduce w it h aging. In early infancy t he neck shaft angle is about 150 o, in childhood 140 o, in
adult about 125o and in elderly about 120o3. Operat ions on proximal femur are one of t he commonest in ort hopaedic surgical pract ice. The aim of t hese operat ions is t o remove pat hology & rest ore anat omy t o t he norm al as far as possible. Since build, physique, habit s & genet ic makeup vary markedly in different et hnic groups, it is possible t hat ant hropomet ric dimensions describe as normal for proximal end of femur for w est ern region be quite different from t hese encountered amongst Indian[3,4,5].
The know ledge of t he angle of inclinat ion is a valuable aid in t he diagnosis and t reat ment of t he fract ures of upper end of femur. The lengt h of t he fem ur and st at ure are of forensic & ant hropological significance. Bony markers such as t he head & neck of femur can be used in det erm ining t he fem oral lengt h w hen only a fragment of proximal femur is available & t he required size of lengt h of t he neck can be determined t o design prost hesis for rest orat ion of normal neck shaft angle. The present st udy aim is t hat t o find out fem oral lengt h, Neck lengt h and Neck shaft angle.
In present st udy have used 250 femurs from different colleges in sout h India. The follow ing measurement s were measured Neck shaft angle, Femoral Lengt h and Neck Lengt h of femur.
Inst r um ent s Used for t his st udy are Sliding Caliper, Osteomet ric Board and m esurement s m easu r ed acco r di n g t o st an dar d an t hr o -pomet rical met hod[6,7].
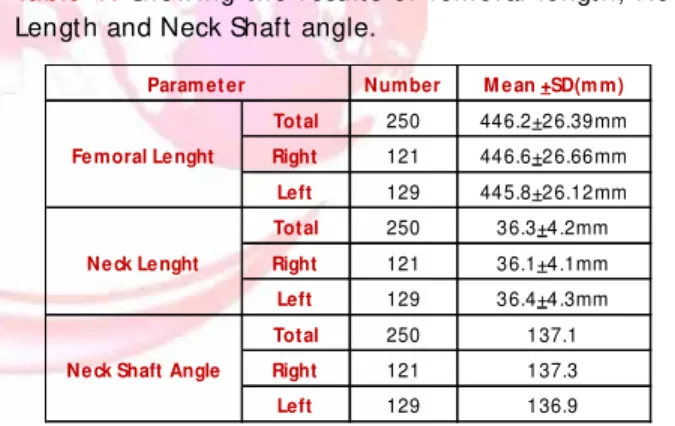
The result s of present st udy are t he lengt h of fem ur w as 446.2+26.39m m , right fem ur was 446.6+26.66m m an d lef t fem u r w as 445.8+26.12mm , t he Neck Lengt h femur w as 36.3+4.2mm, right femur was 36.1+4.1mm and left femur was 36.4+4.3m. The neck shaft angle of femur was 137.10 , right femur was 137.30 and
left femur was136.90(Table 1).
Table 1: Show ing t he result s of fem oral lengt h, Neck
Lengt h and Neck Shaft angle.
Number M e an +SD(m m)
Total 250 446.2+26.39mm
Right 121 446.6+26.66mm
Left 129 445.8+26.12mm
Total 250 36.3+4.2mm
Right 121 36.1+4.1mm
Left 129 36.4+4.3mm
Total 250 137.1
Right 121 137.3
Left 129 136.9
Fe moral Le nght
Ne ck Le nght
Ne ck Shaft Angle Param et er
DISCUSSION
Int J Anat Res 2014, 2(4):633-35. ISSN 2321-4287 635 Shakil M ohamad Khan, Shaik Hussain Saheb. STUDY ON NECK SHAFT ANGLE AND FEM ORAL LENGTH OF SOUTH INDIAN FEM URS.
Conflicts of Interests: None
REFERENCES
How to cite t his article:
Shakil M oham ad Khan, Shaik Hussain Saheb. STUDY ON NECK SHAFT ANGLE AND FEM ORAL LENGTH OF SOUTH INDIAN FEM URS. Int J Anat Res 2014;2(4):633-635.
DOI: 10.16965/ ijar.2014.512 476.70 m m , sexing w as not possible[8]. The
present st udy femur lengt h is correlated w it h st ud y of Raj esh w ar i S B[ 9] . Acco rd i n g t o Rajeshwari S B, t he calculat ed range for right male was 379.88-523.33 mm and t hat for right female it was 358.16-476.80 mm.
The mean femur neck lengt h of present st udy was 36.3+4.2 mm, t he right femur neck lengt h was 36.1+4.1 mm and the left femur neck lengt h was 36.4+4.3 mm, our result s are in agreement w it h Ravichandran et al st udy, in t heir st udy t he mean femur neck length was 31.88mm[10]. Our result s also in correlat ion w it h Siwach RC[11] st udy in his st udy t he mean femur neck lengt h was 37.2 mm and minimum effect ive neck length was 22.6 mm.
The m ean Neck shaft angle of present st udy 137.10, t he right femur neck shaft angle 137.30
and t he left w as 136.90. Our result s are in
agreement w it h Ravichandran et al st udy, in their st udy t he neck shaft angle was 126.550[10]. Our
result s also in agreement w it h st udy of Subhash Gujar, in t heir study t he average neck shaft angle was 136.20. The average neck shaft angle of Isaac
et al st udy was 126.70[1], In Siwach RC st udy it
was 123.50. in our st udy t he neck shaft angle
correlat es posit ively w it h lengt h of neck of femur[12].
CONCLUSION
In t he present st udy t he m ean fem oral neck angle was 137.10, was 9.8°. mean femur neck
lengt h was 36.3+4.2 mm and t he mean lengt h of femur was 446.2+26.39 mm. There was no significant difference bet w een right and left femur bones. Therefore t his st udy w ill be of use in t he fields of ort hopaedic surgery t o diagnose var i o u s h i p p at h o l ogi es an d i n pl an ni n g derotat ion osteot omy of femur, forensic ant hro-pology t o determine t he racial variat ions of t he femoral anteversion and also t o t he anat omist s.
[ 3] . W i lliam s Per t er L. War w ick Roger. Dyson M ar y Bannist er Law rence H. Gray’s Anat omy.. Churchill livingst one London. Edit or J. 40t h e 1989;434. [4] . R A Dut hie, M F Bruce, J D Hut chison - Changing
proxim al fem oral geom et ry in nor t h east Scot land: an ost eom et r ic st udy. BM J 1998;316:16.
[5] . Norkin, C.C. and P.K. Levangie. The hip com plex. In Joint St r uct ure and Funct ion. Phi ladelphia: F.A. Davis. 1983;255–289.
[ 6] . Si n gh IP, Bh asi n M K. A m an u al o f Bi o l ogi cal Ant hropology. 1st edi, Kam la Raj Ent erprices. 1970. [7] . Singh SP, Ekandem GJ, Ani EO. Ident ificat ion of sex from t he head of t he fem ur- dem arking point s for Calabar, Cross-River Stat e Nigeria. West Afr J Anat . 1986;1:16-23.
[8] . Pandya A M , Singel T C, akbar i V J, Dangar K P, Tank K C, Pat el M P . Sexual dim orphism of m axim um f em o r al Len gt h . Nat i o n al j o u r n al o f m ed i cal research. 2011;1(2).
[ 9] . Rajesh w ar i S. Bhosal e, Dr. B. R. Zam bare. Sex det erm inat ion from fem ur using lengt h of fem ur in M aharasht ra. Jour nal of Dent al and M edical Sciences. 2013;3(4):01-03.
[10]. Ravichandran D et al. Proxim al fem oral geom et ry in Indians and it s clinical applicat ions. J. Anat . Sco. India 2011;60(1):6-12.
[ 11] .Siw ach RC, Dahiya S. Ant hro pom et r ic st udy of proxim al femur geom et ry and it s clinical apllicat ion. Indian journal of Ort hopaedics. 2003;37(4):247-51.
[1]. Subhash Gujar, Sanjay Vi kani, Jigna Par m ar, K V Bondre. A correlat ion bet w een fem oral neck shaft angle t o fem oral neck lengt h. IJBAR;2013:04(05). [2] . S. P. Tuck, D. J. Raw lings, A. C. Scane, I. Pande, G. D.