en 1980 220X reeusp 49 spe 0093
Texto
Imagem
Documentos relacionados
Considering that stress and burnout in nursing is a re- ality and that the literature has not yet provided a clear deinition of which factors are associated with them, this
1) Structure of PCIRAS (PCET): structural evaluation of its formation and technical operational support, such as human resources, infrastructure, and technical and adminis-
function, as shown by the clearance of creatinine, increased tubular function markers and fractional excretion of sodium, potassium, magnesium and oxidative metabolites..
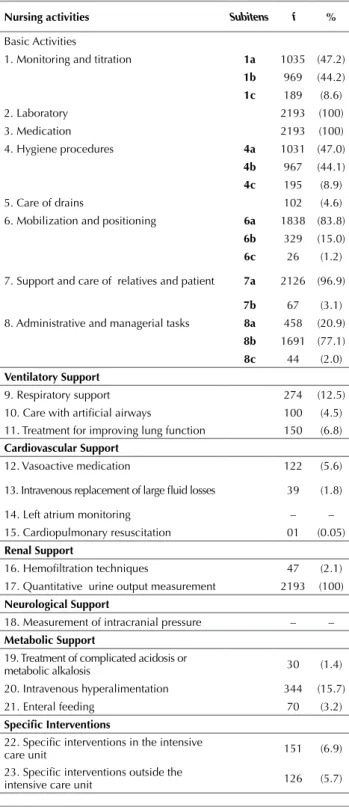
he identiication of factors associated with increased score of the NAS, which included increased length of stay in the ICU and the presence of complications, although re- stricted
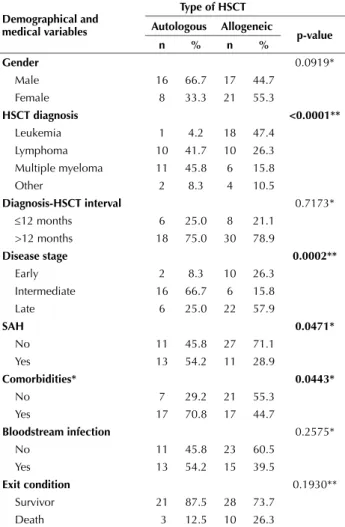
According to the decree, the allogeneic hematopoietic stem cell transplantation (HSCT) with related donor, of bone marrow, peripheral blood or umbilical cord blood,
The hematopoietic stem cell transplantation (HSCT) is the only curative alternative for Myelodysplastic Syndrome (MDS), but many patients are not eligible for this treatment, as
The highest number of episodes of neutropenia were observed in patients from the Hematology Service (48.1%), followed by patients from Hematopoietic Stem Cell Transplantation (HSCT
Patients undergoing transplantation of hematopoietic stem cell transplantation (HSCT) need special care due to the long period of hospitalization and social isolation.. This
