Rev. Saúde Pública vol.44 número4
Texto
Imagem

Documentos relacionados
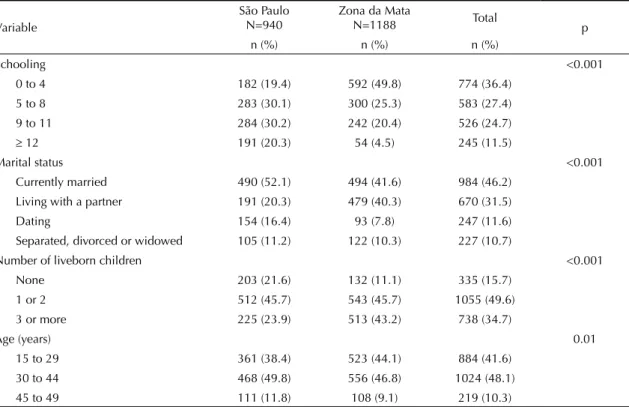
A study done in two Brazilian regions as part of the WHO Multi-country Study on Women’s Health and Domestic Violence against Women, 19 identiied that having up to eight years
Intimate partner violence com- mitted against women in the previous 12 years presented a prevalence of 21.0%, 90.6% and 39.1%, for the categories of physical assault,
Intimate partner violence (IPV) re- fers to physical, sexual and psychological abuse (or threat of such abuse) and violence against women and girls that is perpetrated by intima-
OBJECTIVE: To estimate the prevalence of (physical, psychological, and sexual) violence against women by an intimate partner and non-partner perpetrators among users of public
The present study was the fi rst known Brazilian cohort to estimate the prevalence and incidence of violence against women perpetrated by an intimate partner and assess
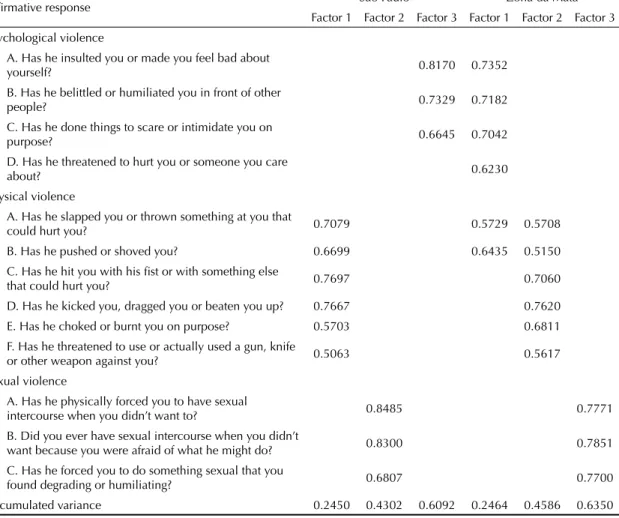
The study investigated the presence of gender violence through the Brazilian version of the World Health Organization Violence against Women instrument, and suicidal ideation
Objective: To analyze the social representations of the Nursing Technicians and Community Health Agents about domestic violence against women.. Method: A
Results were gathered in three thematic groups: women killed with cruelty, sexual violence against women regardless of age, and violence against women and the limitations of the
