www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Cervical
vestibular
evoked
myogenic
potentials
in
children
夽
Alcione
Botelho
Pereira
a,∗,
Gabriela
Souza
de
Melo
Silva
a,
Aída
Regina
Monteiro
Assunc
¸ão
b,
Ciriaco
Cristóvão
Tavares
Atherino
b,
Fernando
Madalena
Volpe
c,
Lilian
Felipe
daUniversidadeVeigadeAlmeida(UVA),RiodeJaneiro,RJ,Brazil bHospitalUniversitárioPedroErnesto(UERJ),RiodeJaneiro,RJ,Brazil
cTeachingandResearchManagement,Fundac¸ãoHospitalardoEstadodeMinasGerais,BeloHorizonte,MG,Brazil dUniversidadeFederalFluminense(UFF),Niterói,RJ,Brazil
Received8January2014;accepted12August2014 Availableonline9June2015
KEYWORDS
Posturalbalance; Child;
Vestibularevoked myogenicpotentials; Diagnosis
Abstract
Introduction:Cervicalvestibular evokedmyogenic potentialisatestusedinneurotological examination.Itverifiestheintegrityofvestibularfunctionthroughamuscularresponseevoked byanacousticstimulationwhichactivatesthesaccularmacula.Normalstandardsinadultshave beenestablished,however,therearefewpublisheddataonthenormalresponsesinchildren.
Objective:Toestablishnormalstandardsforvestibularmyogenicresponsesinchildrenwithout neurotologicalcomplaints.
Methods:Thisstudy’sdesignisacohortwithcross-sectionalanalysis.Thesampleconsistedof 30subjects,15females(50%)and15males(50%).
Results:Theageofthesubjectsrangedbetween8and13years,withameanof10.2(±1.7). P1peakshowed anaveragelatencyof17.26 (±1.78)msandameanamplitudeof49.34(±
23.07)V,andtheN2peakshowedanaveragelatencyof24.78(±2.18)msandmeanamplitude
of66.23(±36.18)V.P1---N2meanamplitudewas115.6(±55.7)V.Therewerenostatistically
significantdifferenceswhencomparingbygenderorbylaterality.
Conclusion:Weestablishednormalvaluesofcervicalmyogenicvestibularresponsesinchildren between8and13yearswithoutneurotologicalcomplaints.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:PereiraAB,deMeloSilvaGS,Assunc¸ãoARM,AtherinoCCT,VolpeFM,FelipeL.Cervicalvestibularevoked myogenicpotentialsinchildren.BrazJOtorhinolaryngol.2015;81:358---62.
∗Correspondingauthor.
E-mail:[email protected](A.B.Pereira).
http://dx.doi.org/10.1016/j.bjorl.2014.08.019
PALAVRAS-CHAVE
Equilíbriopostural; Crianc¸a;
Potenciaisevocados miogênicos
vestibulares; Diagnóstico
Potencialevocadomiogênicovestibularcervicalemcrianc¸as
Resumo
Introduc¸ão: Opotencialevocadomiogênicovestibularcervical(cVEMP)vemsendoempregado comoexamecomplementaremestudosotoneurológicos.Avaliaafunc¸ãovestibularatravésda respostamuscularoriginadaapartirdeumaestimulac¸ãoacústicaqueativaamáculasacular. Oexamefoi padronizadoem adultos,entretanto,háescassezdedadospublicados sobreas respostasobtidasemcrianc¸as.
Objetivo: Estabelecer valores de normalidade das respostas miogênicas vestibulares em crianc¸assemqueixasotoneurológicas.
Método: Estudodecoortehistóricacomcortetransversal,de30sujeitossemqueixas otoneu-rológicas,8a13anos.
Resultados: Aamostrafoicomposta de15 meninose15 meninas,comidademédiade10,2 (±1,7anos).AcurvaP1apresentouumalatênciamédiade17,26(±1,78)eumaamplitude média-49,34(±23,07),enquantoacurvaN2apresentouumalatênciamédiade24,78(±2,18) eumaamplitudemédiade66,23(±36,18).AamplitudeP1---N2foi115,6(±55,7).Oíndice deassimetriafoide21,3%(±18,6).Nãoforamencontradasdiferenc¸asestatisticamente signi-ficativasquandocomparadosossexos.Damesmaforma,nãoseobservouefeitosignificativoda lateralidadenosresultados.
Conclusão:Foramestabelecidososvaloresdenormalidadedasrespostasmiogênicas vestibu-larescervicaisemcrianc¸asentre8e13anossemqueixasotoneurológicas.
©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Thecervicalvestibular-evokedmyogenicpotential(cVEMP) has been utilizedas a supplementary test in neurotologi-caldisordersandintheevaluationofvertigo.Thisisatest thatassessesthevestibularfunctionthroughareflexmuscle responseinresponsetoahigh-intensityacousticstimulation thatactivatesthesaccularmacula.
Thereflexthatoriginatesinthesacculusistransmitted toneuronsintheganglionofScarpa,advancesthroughthe inferiorvestibularnerve,vestibularnucleusand vestibular-spinal tract,andterminates in themotor neurons for the sternocleidomastoidmuscle.1---3
It is estimated thatchildhood vertigo represents1%of theconsultationsinpediatricneurology.Thisproblemisalso foundin13%ofchildrenreferredforaudiologicevaluation.4 Thatpercentagemaybeevenhigher,duetodifficultiesin establishingthediagnosisandobtaininganadequatehistory fromachild withdizziness, duetoadifficulty in describ-ingthediscomfort.However,pediatricvestibulardisorders areofgreatimportance,becausetheycancauseanumber of effects, such as delayed motor and learning develop-ment, potentially interferingin language,speech,writing andreading.4,5
Amongthecomplementarytestsinanotoneurologic eval-uation, advantages of VEMP are that it is an objective, reliable, noninvasive, inexpensive, easy to perform, and rapidtestthatcausesthepatientnodiscomfort.2,6---8
The test has been standardized in adults,and its nor-malvalueshave beendefined.8---11 However,therearefew publisheddataontheresponsesobtainedinchildren.There isnoBrazilianstandardizationforthistestinthepediatric population,whichlimitsitsapplicabilityinclinicalpractice.
The aim of this study was to establish normal values forvestibularmyogenicresponsesin8---13yearoldchildren withoutotoneurologiccomplaints.
Methods
ThestudywasapprovedbytheResearchEthicsCommittee (Opinionnumber421.510).Allparents/guardianssignedthe Free Informed Consent for participation of their children inthe research. This is a cross-sectionalhistorical cohort study.Thestudygroupconsistedof30subjectsofboth gen-derswithoutotoneurologiccomplaints,whowereaged8---13 years.
Exclusion criteria were: no agreement of par-ents/guardians and children to participate in the study; thepatientdid notfit tothestudied population; cervical rotationdifficulty;external-middleearmalformation; dizzi-ness,tinnitusorother otoneurologiccomplaints;presence ofconductivehearingalteration(typeBtympanogramand absenceofstapedialreflexes);andhearingloss.
All children’s parents and/or guardianswere informed aboutthestudyobjectivesand,afterdueauthorization,the examinationwasperformed.
The subjects were submitted to cVEMP in a quiet and comfortable room, previously reserved for the examina-tions. The tests were performed by two female speech therapists.
ToperformcVEMP,anInteracousticsEclipsedevicewith amoduleforcVEMPwasused.StimuliweresentthroughEar ToneABRinsertionheadphones.
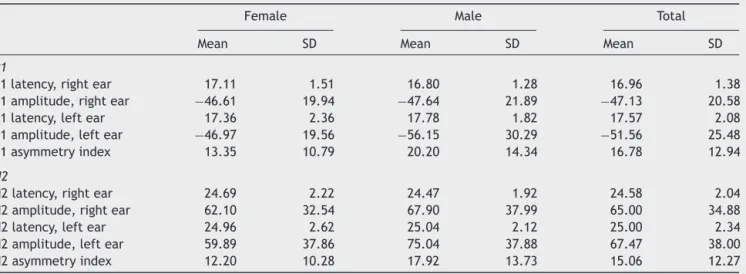
Table1 MeanvaluesandstandarddeviationsofcVEMPcurveparametersin30children.
Female Male Total Mean SD Mean SD Mean SD
P1
P1latency,rightear 17.11 1.51 16.80 1.28 16.96 1.38 P1amplitude,rightear −46.61 19.94 −47.64 21.89 −47.13 20.58 P1latency,leftear 17.36 2.36 17.78 1.82 17.57 2.08 P1amplitude,leftear −46.97 19.56 −56.15 30.29 −51.56 25.48 P1asymmetryindex 13.35 10.79 20.20 14.34 16.78 12.94
N2
N2latency,rightear 24.69 2.22 24.47 1.92 24.58 2.04 N2amplitude,rightear 62.10 32.54 67.90 37.99 65.00 34.88 N2latency,leftear 24.96 2.62 25.04 2.12 25.00 2.34 N2amplitude,leftear 59.89 37.86 75.04 37.88 67.47 38.00 N2asymmetryindex 12.20 10.28 17.92 13.73 15.06 12.27
PS,nosignificantdifferencesbetweengenders. Nosignificantdifferencebetweenbodysides(LandR).
Eletromedicina),electrodes(ECGConductiveAdhesive Med-itrace,Kendall)wereattached.Thesurfaceelectrodeswere placedonthefollowingpositions:activeelectrode onthe middlethirdofthesternocleidomastoid(SCM)muscle, ref-erenceelectrodeonthexiphoidofthesternum,andground electrodeonthe forehead.8 Afterplacement ofthe elec-trodes,theimpedanceamongtheelectrodeswasrecorded. Theimpedancevalueswerecheckedbeforeeachrecording, andimpedancevaluesbetweenelectrodepairsofupto3k wereaccepted.
Thevolunteerwasinstructedtoturnhis/herheadtothe oppositesideinrelationtothestimulatedear,resultingin SCMmusclecontraction.8,12---14Thestimuluswasinitiatedby rightafferencyandthen,leftafferency.Theresponseswere replicated,thatis, theywererecordedtwice ina row on bothsides.Itisimportanttodocumentthereliabilityofthe evokedpotential,sothatthesubjectivityandvariabilityof interpretationsareeliminated.15
cVEMP tracings were obtained in the form of biphasic waveforms: negative-positive, P1---N2. The results were obtainedaftermonauralstimulation.Theacousticstimulus usedwasararefiedtoneburst,withanintensityof100dB Na.Toobtainthewaveform,200stimuliwithfrequencyof 500Hzwerepresented.Theanalysiswindowwas80ms.
The variables studied were: gender; date of birth; latencytoonsetofP1wave;latencytoonsetofN2wave; valueofP1-andN2-amplitude;andasymmetryindex.
Forpurposesofdescriptiveanalysis,theproportionsof categorical variables were studied, and the measures of central tendency (mean, median) of continuous variables werecalculated,aswellastheirrespectivestandard devia-tions.ForcomparativeanalyzesconcerningcVEMPresponses (latencies and amplitudes) between the evaluated body sidesand also in relation to gender, the ANOVA test was used.Thelevelofsignificancewassetat5%(p=0.05).
Results
Thesampleconsistedof30subjects,15females(50%)and 15males(50%).Theageofthesubjectsrangedfrom8to13 years,withameanof10.2(±1.7)years.
Table 2 Correlations (Spearman) between latencies and amplitudesofcVEMPcurvesandageofparticipants.
rho p
P1latency(ms) 0.079 0.549 P1amplitude(V) −0.276 0.033
N2latency(ms) 0.339 0.008 AmplitudeN2(V) 0.383 0.003
In this sample, the P1 peak showed a mean latency of 17.26 (± 1.78)ms and a mean amplitude of 49.34 (±
23.07)V,while theN2peakhadameanlatencyof 24.78
(± 2.18)msand amean amplitudeof 66.23 (± 36.18)V.
TheP1---N2amplitudewas115.6(±55.70)V.The
asymme-tryindexwas21.3%(±18.6%).Themeanvaluesoflatencies andamplitudesofcVEMPcurves,accordingtothelaterality, areshowninTable1.
Statisticallysignificantdifferenceswerenotfound,when comparinggenders.Similarly,therewasnosignificanteffect oflateralityintheresults.
Increasingagewasaccompaniedbyasignificantincrease intheamplitudesofthepeaksP1andN2andbyanincrease inthelatencyofN2,butnotofP1(Table2).
Discussion
cVEMPisarelativelynewtest,whichisstillintheprocess ofvalidationinstudieswithpatientswithspecificvestibular disorders.
The selectedstimuluswasa tone burstat afrequency of500Hz,sincethisstimulusismoreeffectivethanclicks forobtainingcVEMP.16,17Frequencies≤500Hzarethemost often used,resulting in more homogeneous and constant responses.11,16---19
recording,11,20butinthisstudy,weusedthemostcommonly usedSCM.17,21
Several methods have been described for SCM muscle activation during the examination.8,12,22---24 We used head rotation. There are reports using either head rotation or elevation,12,16,17,25,26andtheresponsesaresimilar.26,27The headrotationmethodispreferredforyoungerorolder sub-jects,becauseoftheeaseofmaintainingthatposition.14,26 Thelow asymmetryindexwefound validatesthatmethod forcVEMPrecordinginthisagegroup.
Thelatencyandamplitudevalueswefoundinthisstudy are similar to those reported in the literature in similar age groups (4---19 years).In other pediatric samples with-outotoneurologicdiseaseusingtheheadrotationmethod, themeanlatencyofP1rangedbetween11.3and15.4ms, themeanlatencyofN2rangedfrom18.2to23.7ms,andthe meantotalamplituderangedfrom126.7to160.5V,with asymmetryindicesbetween16---20%.12---14,18Thedifferences observedamongstudiesareprobablyexplainedbytheuse ofdifferentdevices,hencetheimportanceofstandardizing thereferencevaluesbytypeofequipment.
Increasingagewasaccompaniedbyasignificantincrease inpeakP1andN2amplitudes,andbyanincreasedlatency ofN2,butnotofP1.Theeffectofageontheamplitudeof cVEMPwavesisprobablyrelatedtothechangeinthickness oftheSCMmuscle.28Thus,olderchildren,withmore devel-opedmuscles,exhibithigheramplitudes.Asnoageeffects wereobservedwithrespecttoP1latency,theincreaseof N2latencyisprobablyassociatedwithalongerdurationof P1wave.Thisalsomaydependonmuscularfactors,andnot ontheconductionvelocitythroughthenervepathway.
The samplesizewasadequatetoestimatethemeanof latenciesforthepopulation,assumingalessthan5% differ-encewithrespecttotheobservedmeanandwith80%power. Consideringthattheamplitudesshowedahighercoefficient ofvariation,thesamplesizewasadequatetoestimatetheir populationmeans,assumingdifferencesbelow30%.
Conclusion
Normal values for cervical vestibular myogenic responses were established in children aged 8---13 years without otoneurologiccomplaints.Givenitslimitedsamplesize,this studydeservesreplication.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.ColebatchJG,RothwellJC.VestibularevokedEMGresponsesin humanneckmuscles.JPhysiol.1993;473:18.
2.HalmagyiGM,ColebatchJG,CurthoysIS.Newtestsofvestibular function.BaillieresClinNeurol.1994;3:485---500.
3.MurofushiT,ShimizuK,Takegoshi H.Diagnosticvalueof pro-longedlatenciesinthevestibularevokedmyogenicpotential. ArchOtolaryngolHeadNeckSurg.2001;127:1069---72.
4.Gananc¸aFF,Gananc¸aCF.VertigemnaInfânciaena adolescên-cia.In: Gananc¸a MM, editor. Vertigem tem cura?São Paulo: Lemos;1998.p.37---47.
5.LavinskyL, AbelinAC, LavinskyM.Exame otoneurológicoda crianc¸a.In:CaldasN,NetoSC,SihT,editors.Otologiae Audi-ologia emPediatria. Rio deJaneiro: RevinterLtda;1999. p. 287---95.
6.ColebatchJG.Vestibularevokedpotentials.CurrOpinNeurol. 2001;14:21---6.
7.David R, Colafemina JF. Potenciais miogênicos evocados vestibulares(VEMP):umarevisãobibliográfica.RevBras Oto-rrinolaringol.2002;68:113---7.
8.FelipeL,SantosMA,Gonc¸alvesDU.Vestibularevokedmyogenic potential(Vemp):evaluationofresponsesinnormalsubjects. ProFono.2008;20:249---54.
9.Colebatch JG, RothwellJC, Bronstein AH, Ludman H. Click-evokedvestibularactivationintheTulliophenomenon.JNeurol NeurosurgPsychiatry.1994;57:1538---40.
10.Lim CL,CloustonP,Sheean G,Viannikas C.Theinfluenceof voluntaryEMGactivityandclickintensityonthevestibularclick evokedmyogenicpotential.MuscleNerve.1995;18:1210---3. 11.Wu CH, YoungYH, MurofushiT. Toneburst evoked myogenic
potentialsinhumanneckflexorandextensor.ActaOtolaryngol. 1999;119:741---4.
12.OzdekA,TulgarM,SaylamG,TatarE,KorkmazH.Comparison ofheadrotationversusheadelevationmethodsforvestibular evokedmyogenicpotentialsbyusinglogonstimulus.IntJ Pedi-atrOtorhinolaryngol.2009;73:645---9.
13.SinghS,GuptaRK,KumarP.Vestibularevokedmyogenic poten-tialsinchildrenwithsensorineuralhearingloss.IntJPediatr Otorhinolaryngol.2012;76:1308---11.
14.LeeSK,ChaCI,JungTS,ParkDC,YeoSG.Age-related differ-encesinparametersofvestibularevokedmyogenicpotentials. ActaOtolaryngol.2008;129:66---72.
15.MisulisKE.Descric¸ãogeraldospotenciaisevocados.In:Misulis KE,editor.PotencialevocadodeSpehlmamm:potenciaisvisual, auditivoesomatosensitivoevocadosnodiagnósticoclínico.2nd ed.RiodeJaneiro:Revinter;2003.p.5---10.
16.AkinFW,MurnaneOD,PanusPC,CaruthersSK,WilkinsonAE, Proffitt TM. The influence of voluntary tonic EMG level on thevestibular-evokedmyogenicpotential.JRehabilResDev. 2004;41:473---80.
17.MurofushiT,MatsuzakiM,WuC.Shorttoneburst-evoked myo-genicpotentialsonthesternocleidomastoidmuscle:arethese potentialsalsoofvestibularorigin?ArchOtolaryngolHeadNeck Surg.1999;125:660---4.
18.SheykholeslamiK,MurofushiT,KagaK.Theeffectof sternoclei-domastoid electrode locationon vestibularevoked myogenic potential.AurisNasusLarynx.2001;28:41---3.
19.RauchSD,ZhouG,KujawaSG,Guinan JJ,HerrmannBS. Ves-tibular evoked myogenic potentials show altered tuning in patientswithMeniere’sdisease.OtolNeurotol.2004;25:333---8. 20.SakakuraK,TakahashiK,TakayasuY,ChikamatsuK,FuruyaN. Novelmethodforrecordingvestibularevokedmyogenic poten-tial: Minimally invasiverecording onneck extensor muscles. Laryngoscope.2005;115:1768---73.
21.BastaD, TodtI,Ernst A. Normative datafor P1/N1 --- laten-ciesofvestibularevokedmyogenicpotentialsinducedby air-or bone-conductedtone bursts.ClinNeurophysiol. 2005;116: 2216---9.
22.VersinoM,ColnaghiS,CalliecoR,BergamaschiR,RomaniA,Cosi V.Vestibularevokedmyogenicpotentialsinmultiplesclerosis patients.ClinNeurophysiol.2002;113:1464---9.
23.WangCT,YoungYH.Comparisonoftheheadelevationand rota-tionmethodsinelicitingvestibularevokedmyogenicpotentials. EarHear.2006;27:376---81.
24.ItoK,KarinoS,MurofushiT.Effectofheadpositionon vesti-bularevokedmyogenicpotentialswithtoneburststimuli.Acta Otolaryngol.2007;127:57---61.
26.Mudduwa R, Kara N, Whelan D, Banerjee A. Vestibular evokedmyogenicpotentials:review.JLaryngolOtol.2010;124: 43---50.
27.Isaacson B, Murphy E, Cohen H. Does the method of sternocleidomastoid muscle activation affect the vestibular
evoked myogenicpotential response? J Vestib Res. 2006;16: 187---91.