www.jped.com.br
ORIGINAL
ARTICLE
Diabetic
ketoacidosis
in
a
pediatric
intensive
care
unit
夽
Clarice
L.S.
Lopes
∗,
Paula
Pitta
Pinheiro,
Luzia
S.
Barberena,
Guilherme
U.
Eckert
HospitaldaCrianc¸aConceic¸ão,GrupoHospitalarConceic¸ão,PortoAlegre,RS,Brazil
Received26January2016;accepted20May2016 Availableonline19October2016
KEYWORDS
Diabeticketoacidosis; Children;
Cerebraledema; Mortality; Diabetesmellitus
Abstract
Objective: Todescribethecharacteristicsofchildrenaged0---14yearsdiagnosedwithdiabetic ketoacidosisandcomparethefollowingoutcomesbetweenchildrenwithpriordiagnosisoftype 1diabetesmellitusandchildrenwithoutpriordiagnosisoftype1diabetesmellituslengthof hospitalstay,severityonadmission,insulindosage,timeofcontinuousinsulinuse,volumeof fluidsinfusedduringtreatment,andcomplications.
Methods: Aretrospectivedescriptivestudywithreviewofmedicalrecordsofpatientsadmitted tothepediatricintensivecareunitofareferralhospitalfromJune2013toJuly2015.The fol-lowingdataregarding52admissionswereanalyzed:age,sex,weight,bodysurfacearea,signs, symptomsandseverityonadmission,bloodgas,bloodglucose,glycatedhemoglobin, serum osmolarity,andindexofmortality.Theinsulindosage,timeofcontinuousinsulinuse,volume administered intheexpansionphaseandinthefirst 24h,lengthofstay,andcomplications such aselectrolytedisturbances,hypoglycemia,cerebraledema,anddeathwerecompared betweenthetwogroups.
Results: PatientswithoutapreviousdiagnosisofDM1wereyoungeratadmission,withmean age of8.4 years(p<0.01),reportedmorenausea orvomiting,polydipsia andpolyuria,and showedmoreweightloss(p<0.01).Thisstudyalsoobservedahigherprevalenceofhypokalemia (p<0.01)andlongerhospitalstayinthisgroup.
Conclusions: Nodifferencesinseveritybetweengroupswereobserved.Thestudyshowedthat children withoutpriordiagnosis oftype1diabetes mellituswereyounger atadmission, had morehypokalemiaduringthecourseoftreatment,andhadgreaterlengthofhospitalstay. ©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
夽
Pleasecitethisarticleas:LopesCL,PinheiroPP,BarberenaLS,EckertGU.Diabeticketoacidosisinapediatricintensivecareunit.J Pediatr(RioJ).2017;93:179---84.
∗Correspondingauthor.
E-mail:[email protected](C.L.Lopes).
http://dx.doi.org/10.1016/j.jped.2016.05.008
0021-7557/©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND
PALAVRAS-CHAVE
Cetoacidose diabética; Crianc¸as; Edemacerebral; Mortalidade; Diabetesmellitus
Cetoacidosediabéticaemumaunidadedeterapiaintensivapediátrica
Resumo
Objetivo: Descreverascaracterísticasdepacientesdezeroa14anosadmitidoscomdiagnóstico deCetoacidoseDiabéticaecomparardesfechosentreospacientescomdiabetemelitotipo1 prévioeaquelessemdiabetemelitotipo1prévio:tempodeinternac¸ão,gravidadenaadmissão, dosedeinsulinautilizada,tempodeinsulinizac¸ãocontínua,volumedelíquidoinfundidodurante otratamentoecomplicac¸ões.
Métodos: Estudo descritivo retrospectivocom revisão de prontuários de pacientes interna-dosnaUTIpediátricadeumhospitaldereferêncianoperíododejunho de2013ajulhode 2015. Analisamososseguintesdadosreferentes a52 internac¸ões:idade,sexo,peso, super-fíciecorporal, sinais,sintomas,gravidadenaadmissão, gasometrias,glicemia, hemoglobina glicada,osmolaridadeséricaeíndicedemortalidade.Ascrianc¸ascomdiabetejádiagnosticado foramcomparadascomaquelassemdiagnósticoprévioquantoàdosedeinsulina,tempode insulinizac¸ãocontinua,volumeinfundidonafasedeexpansãoenasprimeiras24horas,tempo deinternac¸ãoecomplicac¸õescomodistúrbioshidroeletrolíticos,hipoglicemia,edemacerebral emorte.
Resultados: OspacientessemdiagnósticopréviodeDMIerammais jovensnomomentoda admissão, commédiade idadede8,4anos(p<0,01).Relatarammaissintomascomo vômi-tos, polidipsia e poliúria e apresentaram mais perdade peso (p<0,01).Observamos maior prevalênciadehipocalemia(p<0,01)emaiortempodeinternac¸ãonogrupoacimacitado. Conclusões: Nãoobservamos diferenc¸as quanto agravidadeentreos grupos.Pacientes dia-béticos prévios eram mais jovens na admissão, apresentaram mais hipocalemia durante o tratamentoepermanecerammaistempointernados.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4. 0/).
Introduction
Diabeticketoacidosis(DKA)isapotentiallysevereand com-monconditioninemergencyroomsandpediatricintensive care units (PICU).It is one of the majorcomplications in patients with type 1 diabetes mellitus (DM1). In Brazil, approximately20%ofpatientswithpreviouslyundiagnosed DM1initiallypresentwithDKA.Itismorecommoninchildren under4yearsofageandaffects10/100,000children.1,2As acomplicationinchildrenalreadydiagnosedwithDM1,DKA occursin1---10%ofcases.2
HospitaldaCrianc¸aConceic¸ão(HCC),locatedinthecity of Porto Alegre, state of Rio Grande do Sul, Brazil, is a referencecenter for thetreatment of childrenwithDM1. PatientsadmittedforDKAarereferredfortreatmentinthe PICUof the institution, and after theinitial management andresolutionofacidosis,theyarefollowedatthe Outpa-tientClinicoftheInstituteforChildrenwithDiabetes(ICD). Althoughitisareferenceforthecareofthesepatients,the servicedoesnothaveacareprotocol.
DKA treatment has been widely studied and described intheliterature;however,therearefewstudiescomparing theclinicalcharacteristicsandoutcomesbetweenpatients admittedforDKAwithpreviouslydiagnosedDM1andthose withnopriordiagnosisofDM1.Theobjectiveofthisstudy istoevaluatethecharacteristicsandoutcomesofpatients admittedfor DKAin theintensive care unitof HCC, com-paringthefollowingvariables betweenthepatientwitha DM1diagnosisandthosewithoutpreviousdiagnosis:length of hospital stay, severity on admission, prognostic index
(PediatricIndexofMortalityII), insulindose, timeof con-tinuousinsulinuse,liquidvolumeinfusedduringtreatment, andcomplications.
Methods
Adescriptive,retrospectivestudywascarriedout,basedon areviewofmedicalrecordsofpatientswithDKAdiagnosis admittedtothePICUofHCC,PortoAlegre,fromJune2013 to July 2015. A total of 52 admissions of patients aged betweenzeroand14yearsadmittedforDKAtreatmentwere analyzed.DKAdiagnosiswasdefinedaccordingtothe crite-riaestablishedbytheInternationalSocietyforPediatricand Adolescent Diabetes(ISPAD) Consensusof 2014: venousor arterialbloodgaspH<7.3and/orbicarbonate<15mmol/L, glucoseorhemoglucotest>200mg/dL,presenceof ketone-miaorketonuria.3Patientswithotherdiseasesinaddition to metabolic acidosis were excluded. DKA cases were identified from the PICU database. Data collection was performed using a standardized tool that contained the followingvariables:age,gender,weight,bodysurfacearea, initialdiagnosisofDM1orpreviousDM1,signsandsymptoms on admission, blood gas data (pH, pCO2, HCO3−, BE) on
hypercalcemia, hypokalemia, hyponatremia, cerebral edema,anddeath).
DKAwasclassifiedasmild(pH<7.3orHCO3−<15),
mod-erate (pH<7.2 and HCO3−<10), or severe (pH<7.1 and
HCO3−<5) according to the ISPAD Consensus of 2014.3
Hypoglycemia was defined as blood glucose<60mg/dL, hypokalemia as serum potassium<3.5mEq/L,4 hyper-kalemia asserum potassium>5.0mEq/L,hyponatremia as serumsodium<135mEq/L,4 uncorrected by blood glucose value. Serum osmolality was calculated using the follow-ingformula:[(2×sodium)+(glucose/18)+(Urea/5.6)].4The prognosticindexusedinthisPICUisthePediatricIndexof Mortality(PIM2).5
The data were entered into an Excel spreadsheet for Windows(Microsoft,WA,USA)andanalyzedusingtheSPSS program,version22.0 (IBMCorp.Released2013. IBMSPSS StatisticsforWindows,Version22.0.NY,USA).Quantitative variablesweredescribedasmeansandstandarddeviations, ormediansandinterquartilerangeinasymmetricsituations. Categoricalvariablesweredescribedusingproportionsand percentages. The nonparametric tests used were Fisher’s exact test for comparison of categorical data and Stu-dent’s t-test for comparison of quantitative variables, or theMann---Whitneytestwhenasymmetrywasdetected.For
adjustments,analysisofcovariance(ANCOVA)wasusedfor quantitativedata. Asymmetric quantitative datareceived logarithmictransformation.Theadjustmentofthe categori-caldatawasperformedthroughlogisticregression.Thelevel ofsignificancewassetat˛=0.05.Themultivariateanalysis usedp=0.05fortheprobabilityofinclusionandp=0.1for theprobabilityofexclusion.
ThisstudywasapprovedbytheInstitutionalEthics Com-mittee.
Results
Atotal of 52 admissions wereanalyzed, corresponding to 50patientswhowereadmittedtothePICUofHCCduring a25-monthperiod.Ofthese,26werefemalesandtwo re-admissionswerealsofemalepatients;oneof thepatients hadapreviousdiagnosisofDM1andtheotherreceivedthe diagnosisatthefirsthospitaladmission.Forpurposesofdata analysis,thenumberdisplayedcorrespondstothehospital admissionsandnottothenumberofpatients.
Themeanagewas10.2±2.9years.In59.6%ofthe hos-pitaladmissions,patientshadnopreviousdiagnosisofDM1. Themost frequentlyobservedsymptomswerenauseaand
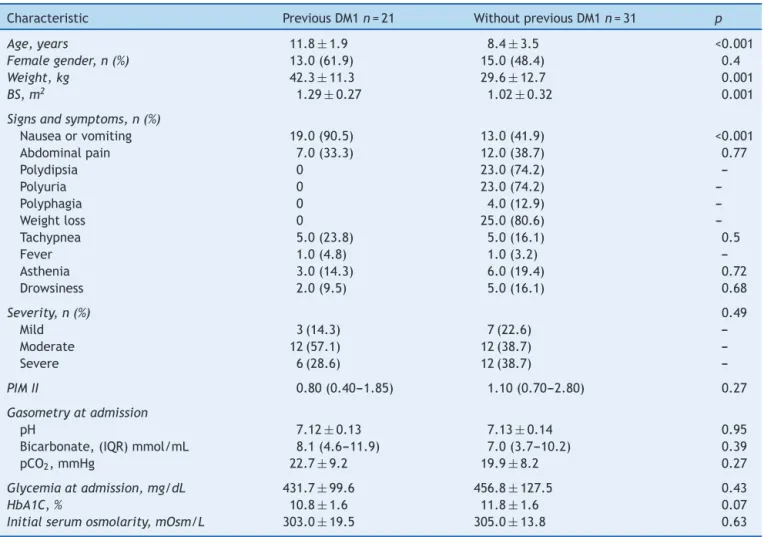
Table1 Baselinecharacteristicsofpatients.
Characteristic PreviousDM1n=21 WithoutpreviousDM1n=31 p
Age,years 11.8±1.9 8.4±3.5 <0.001
Femalegender,n(%) 13.0(61.9) 15.0(48.4) 0.4
Weight,kg 42.3±11.3 29.6±12.7 0.001
BS,m2 1.29±0.27 1.02±0.32 0.001
Signsandsymptoms,n(%)
Nauseaorvomiting 19.0(90.5) 13.0(41.9) <0.001
Abdominalpain 7.0(33.3) 12.0(38.7) 0.77
Polydipsia 0 23.0(74.2)
---Polyuria 0 23.0(74.2)
---Polyphagia 0 4.0(12.9)
---Weightloss 0 25.0(80.6)
---Tachypnea 5.0(23.8) 5.0(16.1) 0.5
Fever 1.0(4.8) 1.0(3.2)
---Asthenia 3.0(14.3) 6.0(19.4) 0.72
Drowsiness 2.0(9.5) 5.0(16.1) 0.68
Severity,n(%) 0.49
Mild 3(14.3) 7(22.6)
---Moderate 12(57.1) 12(38.7)
---Severe 6(28.6) 12(38.7)
---PIMII 0.80(0.40---1.85) 1.10(0.70---2.80) 0.27
Gasometryatadmission
pH 7.12±0.13 7.13±0.14 0.95
Bicarbonate,(IQR)mmol/mL 8.1(4.6---11.9) 7.0(3.7---10.2) 0.39
pCO2,mmHg 22.7±9.2 19.9±8.2 0.27
Glycemiaatadmission,mg/dL 431.7±99.6 456.8±127.5 0.43
HbA1C,% 10.8±1.6 11.8±1.6 0.07
Initialserumosmolarity,mOsm/L 303.0±19.5 305.0±13.8 0.63
Quantitativevariablesareexpressedasmean±standarddeviationormedianandinterquartilerange.
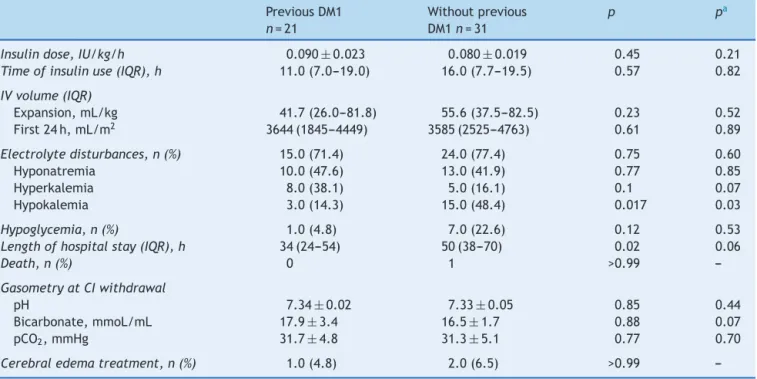
Table2 Outcomes.
PreviousDM1 n=21
Withoutprevious DM1n=31
p pa
Insulindose,IU/kg/h 0.090±0.023 0.080±0.019 0.45 0.21
Timeofinsulinuse(IQR),h 11.0(7.0---19.0) 16.0(7.7---19.5) 0.57 0.82
IVvolume(IQR)
Expansion,mL/kg 41.7(26.0---81.8) 55.6(37.5---82.5) 0.23 0.52 First24h,mL/m2 3644(1845---4449) 3585(2525---4763) 0.61 0.89
Electrolytedisturbances,n(%) 15.0(71.4) 24.0(77.4) 0.75 0.60
Hyponatremia 10.0(47.6) 13.0(41.9) 0.77 0.85
Hyperkalemia 8.0(38.1) 5.0(16.1) 0.1 0.07
Hypokalemia 3.0(14.3) 15.0(48.4) 0.017 0.03
Hypoglycemia,n(%) 1.0(4.8) 7.0(22.6) 0.12 0.53
Lengthofhospitalstay(IQR),h 34(24---54) 50(38---70) 0.02 0.06
Death,n(%) 0 1 >0.99
---GasometryatCIwithdrawal
pH 7.34±0.02 7.33±0.05 0.85 0.44
Bicarbonate,mmoL/mL 17.9±3.4 16.5±1.7 0.88 0.07
pCO2,mmHg 31.7±4.8 31.3±5.1 0.77 0.70
Cerebraledematreatment,n(%) 1.0(4.8) 2.0(6.5) >0.99
---Quantitativevariablesareexpressedasmean±standarddeviationormedianandinterquartilerange.
IU,internationalunits;IV,intravenous;IQR,interquartilerange;PIMII,PediatricIndexofMortalityII;CI,continuousinsulin. aStatisticalsignificanceadjustedforage,gender,severityofDKA,andPIMII.
vomiting,followedbyweightloss,polyuria,andpolydipsia. Patientslessfrequentlyreportedabdominalpain,asthenia, somnolence,tachypnea,andpolyphagia.
It was observed that children with no prior diagnosis of DM1 were younger at the time of hospital admission andmore frequentlyhad polydipsia, polyuria,and weight loss,whereaspatientswhoalreadyhadadiagnosisofDM1 morefrequentlyexperienced vomiting asthemost preva-lentsymptom.Table1showsthecomparisonbetweenthe basalcharacteristicsofthetwogroups.
Whenthegroupswerecomparedregardingoutcomes,no statisticallysignificantdifferencewerefoundwithregardto insulindoseandtimeofcontinuousinsulinuse,severityat admission,intravenous volumeadministeredinthe expan-sionphaseandinthefirst24h,andhypoglycemia(Table2). Also, there was no statistically significant difference in thenumber of patientswho required treatment for cere-braledema.Theprevalenceofelectrolytedisturbanceswas similarbetween thetwogroups; however,when analyzed separately, hypokalemia was more frequent in the group of patients withno previous diagnosis of DM1(p=0.017). Patients who did not know they were diabetics also had greaterlengthofhospitalstay,withameanof50h(p=0.02). Therewasonedeathinthegroupofpatientswithnoprior diagnosisofDM1andthecauseofdeathwascerebraledema.
Discussion
Hospitaladmissions forDKA accountforapproximately5% ofhospitalizationseachyearinthisservice.Theworldwide incidenceofDM1rangesfrom0.1to36.8casesper100,000 inhabitantsperyearand,despitetheeducationalprograms
and the numerous studies onthe subject, mortality from DKAhasremainedaround1---2%since1970.2
The present study included 52admissions, correspond-ingto50patients.Ofthese,40.4%hadapreviousdiagnosis ofDM1.Themeanageofadmissionwas11.8years,which demonstratestheimportanceofparentalinvolvementinthe treatmentoftheirchildrenandineducationalprograms.
As for the symptoms at admission, the most frequent werenauseaandvomiting.Patientswhodidnotknowthey werediabeticsmoreoftenhadrecordsintheirmedicalfiles oftheclassicsymptomsofDM1,suchaspolydipsia,polyuria, andweightloss.Thesefindingswerenotobservedinother studies.3,6Thismayhaveoccurredbecausethepatientswho werealreadyusinginsulinhadmoreacuteclinical decom-pensation,duetotheinappropriateuseofmedicationordue tothemoreobjectivemedicalapproachwhenadiagnosisof DM1hadalreadybeenestablished.7
ofinsulincanbesafe,promotingamoregradualreduction inserumosmolalityand,thus,reducingtheriskofcerebral edema.11Analysisofthepresentstudyshowednodifference betweenthetwogroupsregardingtheadministeredinsulin dose.
Astudy comparing117children hospitalizedforDKAin ahospitalin Pakistanshoweda longercontinuoustimeof insulinuseinpatientsthathadnodiagnosisofDM1at admis-sion. However, these patients were categorized as being more severe.14 A study in Campinas, state of Sao Paulo, Brazil,showedthatthetimeofcontinuousinsulinusewas directlyproportionaltolaboratoryabnormalitiesand,thus, toDKAseverity.2The timeofcontinuousinsulinuseinthe present study was slightly longer in patients who had no diagnosis of DM1prior totheDKA episode,but therewas nostatisticallysignificantdifference.
When the outcome electrolyte disturbance was evalu-ated,thegroupsshowednodifference;however,wheneach disorderwasanalyzed separately,hypokalemiawas signifi-cantlymorefrequentinpatientswithoutapriordiagnosisof DM1.Aninternationalstudyshowednodifferencebetween groupswhenhypokalemiawasevaluatedasacomplication oftreatment.14Inanotherstudy,inwhichmostofthe chil-drenhadDKAasthefirstmanifestationofDM1,hypokalemia wasdetectedin41%ofcasesduringtreatment.15 The chil-dren with DKA have a total body deficit of potassium of around3---6mmol/kg.8 Potassiumisusuallylostasaresult ofvomiting,osmoticdiuresis,andhyperaldosteronism sec-ondary tovolume depletion, which also promotes urinary excretionofpotassium.Insulinadministrationandacidosis correctioncausepotassiumtobedivertedtothe intracellu-larenvironment,furtherdecreasingserumlevelsofthision, whichmaypredisposetoarrhythmias.4,8
Fortheauthors,apossiblereasonwhythechildrenwith no diagnosis of DM1 had higher hypokalemia might have been the fact that they were exposed to the abovemen-tionedpathophysiological mechanismsfor alonger period oftime,withamoredepletedtotalbodypotassiumin rela-tiontochildrenalreadyundergoingtreatmentforDM1.More studiesareneededtoconfirmthisfinding.
Hypoglycemiaasacomplicationoftreatmentoccurredin 15%ofhospitalizations,whichissimilartootherstudies.14,15 Whenthetwogroupswerecompared,childrenwithoutDM1 hadmorehypoglycemia,butthisfindingwasnotstatistically significantandvariationsinglucoseinputusedinthisservice canprobablyexplainthisfact.
Regardinglengthofhospitalstay,thisstudyshowedthat patients without a previous diagnosis of DM1 remainedin thePICUfor alongerperiodoftime,aswasalsoobserved inastudy carriedoutin Pakistan.14 Thiscanbeexplained bythefactthatthesepatientsoftenrequiremoretimefor insulindoseadjustmentandforthefamilytogetusedtothe treatment.
Asgreaterseveritywasnotobservedinpatientswithout a previous diagnosis of DM1, nor a statisticallysignificant differenceintimeofinsulinuse,thesefactorsdonotseem tohaveinfluencedthelengthofhospitalstay.
Inthisstudy,threepatientsreceivedtreatmentfor cere-braledema(hypertonicsalinesolutionormannitol),which correspondsto5.7%ofthestudypopulation.Theliterature describesanincidenceof0.5---1%ofcerebraledemadueto DKA;however,changes inthe mentalstatuswithGlasgow
ComaScale score <14occur inapproximately15% of chil-drentreated forDKA andareassociatedwithevidenceof cerebraledemainimagingstudies.3,8Takingthesedatainto account,itcanbeconsidered thatthissample followsthe patternsreportedinotherstudies.
It is possible that more patients showed some degree of cerebral edema, characterized by symptoms such as headache,drowsiness,vomiting,andlethargy.Asthisstudy wasbased onchartreview,the datamayhave been lost, becauseclinical symptomsarefrequently notrecorded in themedicalfiles.
There was no statistically significant difference in the incidenceofcerebraledemabetweenthetwogroups,which wasexpected,sinceketoacidosisseverityatadmissionand theamountofadministeredvolumeweresimilar.Thereis evidencethatmoreseveredehydrationandrefractoryshock areriskfactorsfordevelopmentofcerebraledema.16
Thepresentstudyshowsthehighprevalenceof hospital-izationsdue toDKAinthisservice; thisfact indicatesthe needforpublicawarenessaboutthesymptoms,aswellas theimportanceoffamilyinvolvement inthemanagement ofthesepatients.
This PICU does not have a treatment protocol for DKA cases,whichmakesthemanagementheterogeneous, possi-blyinfluencingtheobservedclinicaloutcomes.This wasa retrospectivestudy,notriggerfactorswereidentified,and thesamplesizewassmall,alimitation.
Itwasconcludedthattherewerenodifferencesin sever-itybetweenthegroups.PatientswithapriorDM1diagnosis wereyoungerat admission,hadmore hypokalemiaduring treatment, and had greater length of hospital stay. Fur-therstudiesareneededtoperformabetterepidemiological assessmentofthesegroups.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.ICD. InstitutodaCrianc¸a comDiabetes ---RS--- Aspectos epi-demiológicos;2016.Availablefrom:http://www.icdrs.org.br/ aspectos.php[cited25.01.16].
2.CastroL,MorcilloAM,Guerra-JúniorG.Diabeticketoacidosisin children:treatmentprofileatauniversityhospital.RevAssoc MedBras.2008;54:548---53.
3.Wolfsdorf JI, Allgrove J, Craig ME, Edge J, Glaser N, Jain V, et al. ISPAD Clinical Practice Consensus Guidelines 2014. Diabetic ketoacidosisand hyperglycemic hyperosmolar state. PediatrDiabetes.2014;15Suppl20:154---79.
4.PivaJP,GarciaPC.Medicinaintensivaempediatria.2nded.Rio deJaneiro:Revinter;2014.
5.SlaterA,ShannF,PearsonG.PIM2:arevisedversionofthe Pae-diatricIndexofMortality.IntensiveCareMed.2003;29:278---85.
6.Calagua-Quispe M, Falen-BoggioJ, VillarrealUN, Del Águila-VillarC,Rojas-GabulliMI.Característicasclínicasybioquímicas deladiabetesmellitustipo2(DMt2)enelInstitutoNacionalde SaluddelNi˜no.AnFacMed.2012;73:141---6.
7.Kanwal SK, Bando A, Kumar V. Clinical profile of diabetic ketoacidosisinIndianchildren.IndianJPediatr.2012;79:901---4.
from the American Diabetes Association. Diabetes Care. 2006;29:1150---9.
9.OlivieriL,ChasmR.Diabeticketoacidosisinthepediatric emer-gencydepartment.EmergMedClinNorthAm.2013;31:755---73.
10.SteelST,ShaneM.Paediatricdiabeticketoacidosis.BJAEduc. 2009;9:194---9.
11.Al Hanshi S, Shann F. Insulin infused at 0.05 versus 0.1 units/kg/hrinchildrenadmittedtointensivecarewithdiabetic ketoacidosis.PediatrCritCareMed.2011;12:137---40.
12.Dunger DB, Sperling MA, Acerini CL, Bohn DJ, Daneman D, DanneTPA,etal.ESPE/LWPESconsensusstatementondiabetic ketoacidosisinchildrenandadolescents;2004.
13.Puttha R, Cooke D, Subbarayan A, Odeca E, Ariyawansa I, BoneM,etal.Lowdose(0.05units/kg/h)iscomparablewith
standard dose (0.1 units/kg/h) intravenous insulin infusion for theinitial treatmentofdiabetic ketoacidosis inchildren withtype1diabetes----anobservationalstudy.PediatrDiabetes. 2016;11:12---7.
14.LoneSW,SiddiquiEU,MuhammedF,AttaI,IbrahimMN,Raza J.Frequency,clinicalcharacteristicsandoutcomeofdiabetic ketoacidosisinchildrenwithtype-1diabetesatatertiarycare hospital.JPakMedAssoc.2010;60:725---9.
15.JayashreeM,SinghiS.Diabeticketoacidosis:predictorsof out-comeinapediatricintensivecareunitofadevelopingcountry. PediatrCritCareMed.2004;5:427---33.