w w w . r b o . o r g . b r
Review
Article
There
have
been
changes
in
the
incidence
and
epidemiology
of
pelvic
ring
fractures
in
recent
decades?
Cláudia
Diniz
Freitas
a,∗,
José
Eduardo
Rosseto
Garotti
a,
Juliana
Nieto
a,
Rodrigo
Pereira
Guimarães
b,
Nelson
Keiske
Ono
a,b,
Emerson
Honda
a,b,
Giancarlo
Cavalli
Polesello
a,baDepartamentodeOrtopediaeTraumatologia,SantaCasadeMisericórdiadeSãoPaulo,SãoPaulo,SP,Brazil
bFaculdadedeCiênciasMédicas,SantaCasadeMisericórdiadeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30August2012 Accepted3October2012
Keywords:
Pelvicbones Epidemiology Hipfractures Meta-analysis
a
b
s
t
r
a
c
t
Thepelvicringfracturescomprise2–8%ofallskeletalinjuries.Astheincidencerisesto 25%inpolytraumaandrepresentsanegativeprognosticfactorwithregardtomorbidityand mortalityofpatients,wesoughtwiththisworktoestablishtheprofileofthese,compared toanalterationintheprofileofpatientswithpelvicringfracturesinrecentdecades.Tothis end,weevaluatedtheepidemiologicalprofile,mechanismofinjuryandtypesoffractures. Byreviewingtheliteratureindexedinthedatabasesrelatedtothetheme,20paperswere selectedthatcontainedtherequirementsforthestudy.FortheperiodbetweenJanuary1987 andDecember1999(firstdecade),andanotherperiodinJanuary2000andDecember2010 (seconddecade),datawereanalyzedbyMann–Whitneytest.TheratingsTile,Youngand BurgessAOwereadequatetopermittheircategorization.Theresearchineachdecadewas homogeneous.Atfirstthelesionsweremoreprevalentinmenwith62.5%withatendency toreversethispatterngiventheincreaseofwomenintheseconddecade(p=0.286).The averageageinthefirstdecadewas39.3years,anincreaseinthesecond(p=0.068).Themost prevalentmechanismsoftraumawererelatedtotrafficinbothperiodsaswellasfractures classifiedastypeA(p=0.203andp=0.457,respectively),havingmortalityratesdecreased (p=0.396).Weconcludethattherewasatendencytoincreaseintheaverageageofpatients (p=0.068);howevertheincreasinginvolvementofwomen(p=0.286)anddecreasedmortality (p=0.396)werenotsignificant.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Houve
mudanc¸as
na
incidência
e
na
epidemiologia
das
fraturas
do
anel
pélvico
nas
últimas
décadas?
Palavras-chave:
Ossospélvicos
r
e
s
u
m
o
Asfraturasdoanelpélvicocompõemde2%a8%detodasaslesõesdoesqueleto,incidência quesobepara25%nospolitraumatizadoserepresentafatorprognósticonegativonoque
∗ Correspondingauthor.
E-mail:[email protected](C.D.Freitas).
2255-4971/$–seefrontmatter©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
analisadosecomparadosestatisticamentepeloTestedeMann–Whitney.Asclassificac¸ões deTile,YoungBurgesseAOforamadequadasparapermitirsuacategorizac¸ão.Aspesquisas emcadaumadasdécadasforamhomogêneas.Naprimeira,aslesõesforammais preva-lentesemhomens,com62,5%,comtendênciaainversãodessepadrão,dadooaumentode mulheresacometidasnasegundadécada(p=0,286).Amédiadeidadenaprimeiradécada erade39,3anoserevelouumaumentonasegunda(p=0,068).Osmecanismosdetrauma maisprevalentesforamaquelesrelacionadosaotráfegonosperíodos,assimcomoas frat-urasclassificadascomo dotipoA (p=0,203ep=0,457,respectivamente).Osíndices de mortalidadediminuíram(p=0,396).Conclui-sequehouvetendênciaaoaumentonamédia deidadedospacientes(p=0,068).Jáocrescenteacometimentodasmulheres(p=0,286)ea diminuic¸ãodamortalidade(p=0,396)nãoforamsignificantes.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Traumaisaworldwidepublichealthproblemandithasbeen estimatedthatintrafficaccidentsalone, traumais respon-sible for around 1.2 million deaths around the world.1 It
presents great morbidity that today affects more than 50 millionpeople.2Thissituationisworseinurbancenters,
espe-ciallyincapitalsandmetropolitanregions,wherethegrowing vehiclefleetandgreateraggressivenessintrafficcause high-energyaccidentsand consequentlyincreasethenumber of deaths.3,4
In the young and economically active population, the maincauseofdeathisexternalagents.Incomparisonwith other age groups, this population is seen to have a more audaciousprofile,whichraisestheratesofmortalitydueto accidentsandurbanviolence.5–11Withinthisscenario,
traf-ficaccidents are amongthe mainhealth hazards,and the risk factors for such accidents are young age group, male sexand lowsocial level.12 The severityof these accidents
givesrisetolongperiodsofhospitalization,withademand forhigh-costresourcesandconsequentlygreaterexpenditure ofpublicandprivatefunds.12–16 Inanattempttominimize
thecatastrophicrepercussionsoftrafficaccidentson Brazil-ianpublic health, medicaland governmental entities have beenincreasinglyadoptingpreventivemeasuresoverrecent years,withtheaimsofdiminishingtheabsolutenumberof accidents and minimizing their consequences. Installation ofmedicalrescueservices onhighways andalsoin Brazil-ian cities, from the 1980sonwards, is an example of this measures.17
Otherwell-knownadvanceswerethecreationofthe Brazil-ianNationalTrafficCodeof1998(Law9503ofSeptember23, 1997),18 whichledtoareductioninthe number ofdeaths,
and also legislation ofgreater rigor, suchas Law 11705 of June 19,2008,19 popularly known asthe “Dry Law”, which
showedaproportionaldecrease inthe riskofdeath.These measureshavebeenshowntobeeffective,althoughtheystill needimprovementandupdating,suchashigherenforcement
levelsanddeepeningoftheeducationalprocessamongthe Brazilianpopulation.20
In parallel with the implementation of these laws that werecreatedinanattempttodiminishthefrequencyofthese accidents,thevehiclefleethasbeenincreasingprogressively. AccordingtoDENATRAN,thenumberofmotorvehicleshas increased by around 300% over the last ten years. In the municipalityofSãoPaulo,themortalityrateamongvictims ofvehicleaccidentsincreasedfrom0.4/100,000inhabitantsto 1.4/100,000inhabitantsovertheperiodfrom1996to2005.21
Today,thereisstillalackofdetaileddataregardingtrauma severity,injuriesmostfrequentlyobserved,sequelaeand com-plicationsspecificallyrelatedtoaccidentsinvolvingvehicles around the world. Such information could help in imple-mentingpreventivemeasuresand providingattendancefor thesepatients,throughdirectingphysiciansintheir diagnos-ticinvestigationsandindeterminingpriorities.
Withthe aimofunderstanding the changesinbehavior within society over recent decades, withregard to trauma mechanismsandconsequentlythetypesofpelvicring frac-ture (Fig. 1A–D), the diagnosis,morbidity and mortalityof pelvicfractureshavebeenwidelydiscussedbyvarious med-icalsocieties,governmentsandthegeneralpopulation.17–19
Pelvicringfracturesaccountfor2–8%ofallskeletalinjuries, which increases to 25% among multiple trauma patients. Withinthiscontext,theyrepresentanegativeprognostic fac-torwithregard tomorbidityand mortalityamongmultiple traumapatients.Thus,thissituationstimulatedusto estab-lish the epidemiological profile of these fractures through reviewingtheliterature.22
Objective
Fig.1–Radiographsofpelvicringfracture.(A)PelvisfractureofTiletypeB,frontalradiograph.Imagefromthefilesofthe HipGroupofDOT-ISCMSP.(B)PelvisfractureofTiletypeB,inletradiograph.ImagefromthefilesoftheHipGroupof DOT-ISCMSP.(C)PelvisfractureofTiletypeB,outletradiograph.ImagefromthefilesoftheHipGroupofDOT-ISCMSP.(D) PelvisfractureofTiletypeB,postoperativeradiograph.ImagefromthefilesoftheHipGroupofDOT-ISCMSP.
Material
AfterobtainingapprovalfromtheResearchEthics Commit-teeofIrmandadedeMisericórdiadaSantaCasadeSãoPaulo (51/2012),abibliographicreviewwasconductedinthe Med-line,PubMed, Lilacsand Cochranedatabasesand literature relating to this topic over the last two decades, searching fordescriptionsoftheepidemiologyofpelvicringfractures. Thesearticleswouldneedtopresentsomeofthefollowing keywords in their content:fractures, pelvic ring; epidemi-ology; pelvic bones, injuries; fractures, bone/epidemiology; accidents,traffic;prospectivestudies;andretrospective stud-ies. The data were gathered between December 2011 and March2012.
Thearticleswereselectedaftercriticalassessmentofthe strength ofevidenceand were onlyacceptedif theimpact wasaminimumof2A.Articlesinwhich,despitetheir appear-anceinthesearchresults,themethodologydidnotinclude completeevaluationofdatabasedonage,sex,trauma mech-anism,mortalityandfracturetype(refinementcriteria)were discarded.
In evaluating the fracture types, we compared the Tile, Young-BurgessandAOclassifications.Weclassifiedfractures astypeAiftheywereTiletypeAandAOtypeA;typeBifthey wereTiletypeB,Young-BurgessgroupsAandBandAOtype B;andtypeCiftheywereTiletypeC,Young-BurgessgroupC andAOtypeC.23
Thesearchlocated152articles,ofwhich73metthe refine-mentcriteria. From these,textsthat appearedinduplicate (totalof52articles)were excluded.Afterreadingthetotals andabstracts,20studiesthatcontainedthedataneededfor thisstudywereselected(Tables1and2).
Method
These articleswere divided into twoperiods:between Jan-uary1987andDecember1999(namedthefirstdecade);and betweenJanuary2000and December2010(namedthe sec-onddecade).Thedatawere analyzedstatisticallyusingthe Mann–Whitneytest.
For thisstudy,the significancelevelwas definedas0.05 (5%), and confidence intervals were constructed over the lengthofthestudy,with95%statisticalconfidence(Table3).
Inthisstatisticalanalysis,thefollowingsoftwarewasused: SPSSV17,Minitab16andExcelOffice2010.
Results
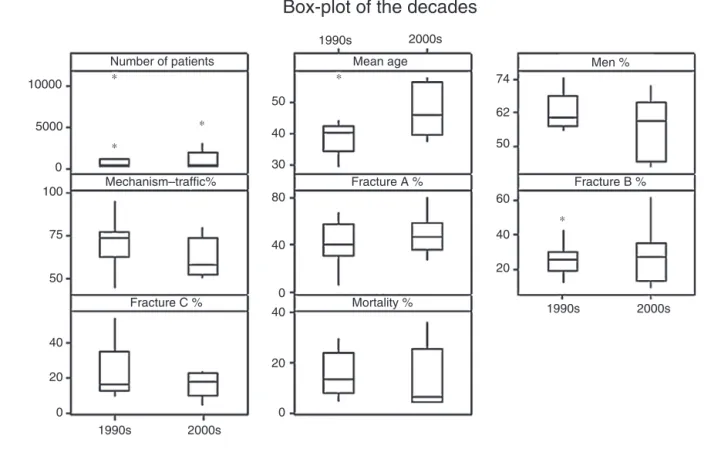
Basically,wecansay (withtheexception ofthe numberof patients)thatstudygroupsineachdecadepresentedlow vari-abilityregardingtherefinementcriteria,sincethecoefficients ofvariancewerelowerthan50%anddemonstratedthatthe studiesineachofthedecadeswerehomogenous(Table3and
Fig.2).
Inthefirstdecade,pelvicringinjuriesweremore preva-lentamongmen(62.5%)thanamongwomen(37.5%).However, inthe seconddecade,agreater proportionofwomenwere affected(43.3%),althoughwithoutexpressingasignificant dif-ference(p=0.286).
Themeanageinthefirstdecade was39.3years,witha tendencytowardincreasedmeanage,ofuptosevenyears,in theseconddecade(p=0.068).
5000
100 Mechanism–traffic%
Mortality % Fracture C %
Fracture A % Fracture B %
75
50
40
40 80 30 40 50
62
50
60
40
20 40
20
0
20
0 0
1990s 2000s
1990s 2000s 0
∗
∗
∗
Fig.2–Box-plotofthedecades,forallvariables.
vehicleaccidents,motorcycleaccidentsandbeingrunover. Thispredominance wasmaintainedthroughouttheperiod, with70.7%and62.7%,respectively(p=0.203),andwas there-forenotshowntobesignificantdata.
Wealsofoundthatmostofthefractureswereclassifiedas typeA(40.5%),followedbytypeB(26.7%)andtypeC(23.5%) inthefirstdecade.TherewereslightincreasesinthetypesA andBinjuries(48.6%and28%)intheseconddecade,butthese findingsdidnothavestatisticalvalidity(p=0.457andp=0.967, respectively).
Themortalityratewas15.1%inthefirstdecadeandthis decreasedto13.6%intheseconddecade.Thisdifferencewas notfoundtobesignificant,afteranalysis(p=0.396).
Discussion
Withregardtoattendanceformultipletraumavictimsinthis city,wehavenotedchanges intheepidemiologicalpattern ofpelvicringfracturesinpatientstreatedatourserviceover recentyears.Thishasgivenrisetotheneedforusto inves-tigate whether such changes have also been noted in the specializedliterature.
Westudied20articlesthatcoveredtheperiodfrom1995 to2012,respectingthecriteriaenumeratedearlier.Through ATLSandpublichealthmeasuresthatwereimplementedat the beginning ofthe 1980s, multipletrauma patients have becomebetterunderstood,withcaredeveloped,implemented andsystematizedoverthelast20years.Byfocusingonthis period,wesoughttoinvestigatetheepidemiologicalprofileof pelvicringinjuries.22
Atendencytowardinversionoftheproportionsregarding thegendermostaffectedwithpelvicringfractures,giventhat thepresentreviewfoundthatfemalesbecamemoreaffected inthelastdecade,althoughthisincreasewasnotsignificant (p=0.286).Thissituationmayberelatedtowomen’s consoli-dationintheworkplaceandwithinsocialstructures,whichis increasinglyactiveandeconomicallyparticipative,thus lead-ingtogreaterexposuretotraumaticevents.
The aging of the population, with increasing life expectancy worldwide, is leading to a need for effective participationinday-to-dayactivitiesamongindividualsover the ageof60 years,who nowadaysseemtobemore inde-pendent and self-sufficient.Theimproved abilitytoaccess appropriate healthcare services, which formerly did not provideadequateortimelycareforsurvivalwithinthisage group, andoptimizationofattendanceformultipletrauma victims, corroborate the findings of increased mean age for pelvicring injuries, comparingthe two periods),which expressedastatisticaltendencyafteranalysis(p=0.068).
Inthe studiesevaluatedhere, thetraumawas predomi-nantlyduetovehicletraffic-relatedaccidents,inbothperiods, eventhoughthisfindingdidnothavevalidation(p=0.203).On theotherhand,therewasnostratificationamongthe differ-entpossibilitiesforthistypeofevent,suchas:beingrunover, motorcycleaccidentsorcaraccidents.Thisgivesrisetoa cer-tainamountoffrustration,giventhatinmakingananalysis onthedata,itwasnotpossibletomakeinferencesregarding whichvectorsweremoreprevalent.
Table1–Studiesanalyzedinthefirstdecade. Reference
(1) BrennemanFD,KatyalD,BoulangerBR,TileM, RedelmeierDA.Long-termoutcomesinopenpelvic fractures.SourceDepartmentofSurgery,
SunnybrookHealthScienceCenter,Universityof Toronto,Ontario,Canada.JTrauma.1997 May;42(5):773–7.
(2) LindseyM,KohlRW3rd.Pelvicfractureamong polytraumadecedents:trauma-basedmortalitywith pelvicfracture–acaseseriesof74patients.TheBen TaubGeneralHospital,BaylorCollegeofMedicine, Houston,Texas,USA.ArchOrthopTraumaSurg. 2001;121(1–2):43–9.
(3) GrotzMRW,AllamiMK,HarwoodP,PapeHC,Krettek C,GiannoudisPV.Openpelvicfractures:
epidemiology,currentconceptsofmanagementand outcome.Injury.2005;36(1):1–13.
(4) ChongKH,DeCosterT,OslerT,RobinsonB.Pelvic fracturesandmortality.IowaOrthopJ.1997;17:110–4. (5) GurevitzS,BenderB,TytiunY,VelkesS,SalaiM,
SteinM.Theroleofpelvicfracturesinthecourseof treatmentandoutcomeoftraumapatients.IsrMed AssocJ.2005;7(10):623–6.
6) BarzilayY,LiebergallM,SafranO,KhouryA, MosheiffR.PelvicfracturesinalevelItrauma center:atestcasefortheefficacyoftheevolving traumasysteminIsrael.IsrMedAssocJ.2005 Oct;7(10):619–22.
(7) GiannoudisPV,GrotzMR,TzioupisC,DinopoulosH, WellsGE,BouamraO,LeckyFJ.Prevalenceofpelvic fractures,associatedinjuries,andmortality:the UnitedKingdomperspective.Trauma.
2007;63(4):875–83.
(8) GänsslenA,PohlemannT,PaulC,LobenhofferP, TscherneH.Epidemiologyofpelvicringinjuries. Injury.1996;27Suppl.1:S-A13-20.
(9) SchmalH,MarkmillerM,MehlhornAT,SudkampNP. Epidemiologyandoutcomeofcomplexpelvicinjury. ActaOrthopBelg.2005;71(1):41–7.
(10) PohlemannT,TscherneH,BaumgärtelF,EgbersHJ, EulerE,MaurerF,FellM,MayrE,QuiriniWW, SchlickeweiW,WeinbergA.Unfallchirurg.Pelvic fractures:epidemiology,therapyandlong-term outcome.Overviewofthemulticenterstudyofthe PelvisStudyGroup.1996;99(3):160–7[German] (11) ParreiraJG,HaddadL,RasslanS.Abdominalinjuries
inpatientssustainingpelvicfractures.RevColBras Cir.2002;29(3):mai/jun.
conducting clinical studies on this topic but also making correlations between the mechanisms and the fracture classification, severity, evolution, complications and prog-nosis. The relevance of these data lies in their ability to help implement preventive public health measures, par-ticularlywith regard to traffic education and the need for referralandspecializationcentersfortreatinginjuriesofthis type.
TypeAfractureswerethemostprevalenttypeduringboth oftheperiodsanalyzed,whichmaybeexplainedbyaccepting thatthistypeofinjurydoesnotprogresstodeath,thusmaking itpossibleforallcaseswiththisdiagnosistobeincludedinthe databases(p=0.457).Therewasanincreaseinthenumbers offracturesclassifiedasB(p=0.967),comparingthedecades
Table2–Studiesanalyzedintheseconddecade. Reference
(1) HolsteinJH,CulemannU,PohlemannT.Whatare predictorsofmortalityinpatientswithpelvic fractures?Symposium:DisruptionsofthePelvic Ring:AnUpdate.ClinOrthopRelatRes. 2012;470:2090–20977(8).
(2) OoiCK,GohHK,TaySY.Patientswithpelvic fracture:whatfactorsareassociatedwithmortality? IntJEmergMed.2010;3(4):299–304.
(3) TosounidisG,HolsteinJH,CulemannU,
HolmenschlagerF,StubyF,PohlemannT.Changesin epidemiologyandtreatmentofpelvicringfractures inGermany:ananalysisondataofGermanPelvic MulticenterStudyGroupsIandIII(DGU/AO).Acta ChirOrthopTraumatolCech.2010;77(6):450–6. (4) SharmaOP,OswanskiMF,RabbiJ,GeorgiadisGM,
LauerSK,StombaughHA.Pelvicfracturerisk assessmentonadmission.AmSurg. 2008;74(8):761–6.
(5) ChienLC,ChengHM,TsaiMC.Pelvicfractureand riskfactorsformortalityApopulationbased.EurJ TraumaEmergSurg;2010;2:131–138.
(6) Je ˇzekM,D ˇzupaV.Theinfluenceofpatientageand mechanismofinjuryonthetypeofpelvicfracture: epidemiologicalstudy.ActaChirOrthopTraumatol Cech.2012;79(1):65–8.
(7) CordtsRMF,ParreiraJG,Perlingero,JAG,SoldáSC,de CamposT,AssefJC.Pelvicfracturesasamarkerof injuryseverityintraumapatients.RevColBrasCir 2011;38(5):310–315.
(8) SiegmethA,MüllnerT,KuklaC,VécseiV.Associated injuriesinseverepelvictrauma.Unfallchirurg. 2000;103(7):572–81.
(9) ChueireIAG,FilhoGC,dosSantosAFI,PockelIKP. Fraturasdoanelpélvico:estudoepidemiológico. ActaOrtop.Bras.2004;12(1),SãoPaulo,Jan./Mar.
analyzed.Thisresultwasexpectedbecauseofthe improve-ment of pre-hospital care, which ensured these patients’ survivalbyimprovingtheirarrivalattheemergencyservice. Withattendanceatthehospitalthatwasmoreappropriate and increasedadmission ofthese patients, the number of patientstreatedincreased.However,theseresultswerenot statisticallysignificantovertheperiodanalyzed.
Despitetheslightdecreaseinthemortalityrateoverthe last decade (p=0.396), it can be inferred that even with-out statisticalsignificance,anddespitepoliciesforaccident prevention,attendance logisticsandinitialmanagementof multipletraumapatients,andwithstructuralimprovements tovehiclesand public highways,humans continueto seek tosurmountlimits,thusofteninsistingonriskingtheirown lives,andthelivesofothers.Thisresultsinsevereandoften fatalaccidents.
Meanage 1990s 39.3 40.0 7.8 20% 35.0 41.2 29.0 58.0 11 4.6 0.068
2000s 46.8 45.6 8.2 18% 39.8 52.8 37.0 58.0 8 5.7
Men% 1990s 62.5 60.1 6.6 11% 57.5 66.2 55.0 75.0 12 3.7 0.286
2000s 55.7 59.0 11.1 20% 45.0 64.0 42.0 72.1 9 7.3
Mechanism–traffic% 1990s 70.7 73.0 13.6 19% 63.8 76.2 44.0 95.5 10 8.5 0.203
2000s 62.7 58.0 11.6 18% 53.9 71.4 50.0 80.0 7 8.6
FractureA% 1990s 40.5 40.6 19.9 49% 30.4 55.9 5.0 68.0 11 11.8 0.457
2000s 48.6 46.4 17.1 35% 38.7 56.3 25.7 81.0 8 11.9
FractureB% 1990s 26.7 25.0 10.9 41% 20.0 28.5 11.6 49.0 11 6.4 0.967
2000s 28.0 26.7 17.1 61% 17.6 34.4 8.7 62.3 8 11.8
FractureC% 1990s 23.5 16.0 15.0 64% 13.3 30.7 9.0 55.0 11 8.8 0.433
2000s 16.2 17.5 7.3 45% 11.4 22.3 3.8 24.0 8 5.1
Mortality% 1990s 15.1 13.5 8.6 57% 9.7 22.8 4.3 30.0 12 4.8 0.396
2000s 13.6 6.5 12.7 94% 4.8 20.5 3.8 37.0 8 8.8
CV,coefficientofvariance;Q1,1stquartiledistributionofupto25%ofthesample;Q3,3rdquartile,distributionofupto75%ofthesample;CI, confidenceinterval;p-value,resultfromeachcomparison.
Conclusion
Weobservedthattheepidemiologicalprofileofthepelvicring fracturesinthetwodecadesdidnotpresentanysignificant changes.Thegrowingtrendforwomentobemoreaffected, theincreaseinthemeanage,andthedecreaseinmortality overtheperiodanalyzedwere thefindingsobservedinour study,butwithoutstatisticalsignificance.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
We thank Prof Dr. Walter Riccioli Junior, Dr. Daniel Dani-achi and Dr. Marcelo Queiroz, attending physiciansin the HipSurgeryGroupofIMSCSP,forperformingtheoperations correlatedwiththistopicthatinstigatedthepresentlineof research.
r
e
f
e
r
e
n
c
e
s
1. AbreuAM,deLimaJM,MatosLN,PillonSC.Alcoholuseand
trafficaccidents:astudyofalcohollevels.RevLatAm
Enfermagem.2010;18.SpecNo.:513-20.
2. MelloJorgeMH,LatorreMR.TrafficaccidentsinBrazil:data
tendencies.CadSaúdePublRiodeJaneiro.1994;10Suppl.
1:19–44.
3. MarinL,QueirozMS.Caraccidentsintheageofspeed:an
overview.CadSaúdePublRiodeJaneiro.2000;16(1):7–21.
4. RodriguesNB,GimenesCM,LopesCM,RodriguesJM.Death,
injuriesanpatternofmotorcycleaccidentvictimsinthecity
ofSorocaba,SãoPaulo,Brazil.RevFacCiêncMédSorocaba.
2010;12(3):21–5.
5. Carlini-CotrimB,Gazal-CarvalhoC,GouveiaN.
Comportamentosdesaúdeentrejovensestudantesdasredes
públicaeprivadadaáreametropolitanadoEstadode,São
Paulo.RevSaúdePúbl.2000;34(6):636–45.
6.LaurentiR,JorgeMH,GotliebSL.Epidemiologicalprofileof
men:morbidityandmortality.CiêncSaúdeColetivaRiode
Janeiro.2005;10(1):35–46.
7.BarrosMD,XimenesR,LimaML.Childandadolescent
mortalityduetoexternalcauses:trendsfrom1979to1995.
RevSaúdePúbl.2001;35(2):142–9.
8.ModelliMES,PratesiR,TauiPL.Alcoolemiaemvítimasfatais
deacidentesdetrânsitonoDistritoFederal.BrasRevSaúde
Públ.2008;42(2):350–2.
9.FariasGM,RochaKM,FreitasMCS,CotaKF,DantasRA.
Acidentesdetrânsitodecorrentesdainfluêncadousodo
álcool.InterSciPlaceRevCientíficaInt.2009;2(9).
10.AbreuAM,LimaJM,SilvaLM.Alcoholemylevelsand
mortalitybytrafficaccidentsinthecityofRiodeJaneiro.Esc
AnnaNeryEnfermagem.2007;11(4):575–80.
11.Gazal-CarvalhoC,Carlini-CotrimB,SilvaOA,SauaiaN.Blood
alcoholcontentprevalenceamongtraumapatientsseenata
level1traumacenter.RevSaúdePúbl.2002;36(1):47–54.
12.SantosAM,MouraME,NunesBM,LealCF,TelesJB.Profileof
motorcycleaccidentvictimstreatedatapublichospital
emergencydepartment.CadSaúdePúblRiodeJaneiro.
2008;24(8):1027–38.
13.ParreiraJG,CoimbraR,RasslanS,RuizDE.Politraumatizados
comtraumacraniencefálicograve:importânciadaslesões
abdominaisassociadas.RevColBrasCir.2001;28(5):336–41.
14.ParreiraJG,HaddadL,RasslanS.Lesõesabdominaisnos
traumatizadoscomfraturasdebacia.RevColBrasCir.
2002;29(3):153–60.
15.JorgeMH,KoizumiMS.GastosgovernamentaisdoSUScom
internac¸õeshospitalaresporcausasexternas:análiseno
EstadodeSãoPaulo,2000.RevBrasEpidemiol.
2004;7(2):228–38.
16.MartinsCB,AndradeSM.Causasexternasentremenoresde
15anosemcidadedoSuldoBrasil:atendimentosem
pronto-socorro,internac¸õeseóbitos.RevBrasEpidemiol.
2005;8(2):194–204.
17.MalvestioMA,SousaRM.Advancedlifesupport:care
providedtomotorvehiclecrashvictims.RevSaúdePúbl.
2002;36(5):584–9.
18.MaltaDC,SilvaMM,LimaCM,SoaresFilhoAM,Montenegro
restrictioninthemorbidityandmortalitybytransport-related
injuries–Brazil,2008.EpidemiolServSaúde.2010;19(1):77–8.
19.MaltaDC,SoaresFilhoAM,MontenegroMM,Mascarenhas
MD,SilvaMMA,LimaCM,etal.Mortalityanalysisoftraffic
accidentsbeforeandafterBrazil’sdrylaw,from2007to2009.
EpidemiolServSaúde.2010;19(4):317–28.
20.SouzaMF,CarvalhoMD,SouzaCG,SilvaMM,CarvalhoCG,
MoraisNetoOL.Descriptiveandtrendanalysesofland
transportaccidentsforpublicpoliciesinBrazil.Epidemiol
ServSaúde.2007;16(1):33–44.
21.Denatran(DepartamentoNacionaldeTrânsito).Frotaantes de2000efrota2011.Disponívelem:http://www.denatran.
gov.br/frota.htm/publicacoes/showpublic.asp?cod=
22.BucholzRW,Court-BrownCM,HeckmanJD,TornettaP.
RockwoodandGreen’sfracturesinadults.3rd.Philadelphia:
Lippincott;2010.
23.OlsonSA,BurgessA.Classificationandinitialmanagementof
patientswithunstablepelvicringinjuries.InstrCourseLect.