A
management
model
applied
in
two
‘no
‐
kill’
dog
shelters
in
central
Italy:
use
of
population
medicine
for
three
consecutive
years
Paolo
Dalla
Villa,
Luigi
Iannetti,
Michele
Podaliri
Vulpiani,
Antonio
Maitino,
Roberto
Trentini
&
Stefania
Del
Papa
Summary
The principal tools currently used in Italy to limit stray dog populations are dog registration and identification, birth control and increasing public awareness. Since 1991, national legislation does not permit euthanasia of unwanted roaming dogs unless they have an incurable condition or are proven to be dangerous. Unattended dogs are placed in long‐term shelters in questionable conditions where they often remain for most of their lives. Kennel management is one of the most critical aspects of animal welfare, particularly as the number of stray dogs is rising faster than the current rate of adoption. The Istituto Zooprofilattico Sperimentale dell’Abruzzo e del Molise ‘G. Caporale’ (IZS A&M) manages two
kennels in Teramo and uses standard management procedures that include regular behavioural and physical examinations. All results recorded in a computer database were analysed to identify production goals and improve welfare, in line with a population medicine model. Prevalence and incidence of different pathologies were recorded and analysed to improve veterinary management and organisation. No new dogs were admitted from 2005 onwards, thereby producing an ideal ‘closed system’ where the effects of rational management can be studied in the absence of unpredictable risks from introduced pathologies. Statistical evaluations revealed major differences between 2006 and 2007. The
use of the ‘population medicine’ management system resulted in improved dog health and welfare, as indicated by the significant reduction in both the prevalence and incidence of major pathologies between 2006 and 2007. A significant improvement was also seen in the control of the incidence of leishmaniasis which reduced sharply during this period.
Keywords
Animal, Dog, No‐kill, Kennel, Management, Population medicine, Shelter, Welfare.
Il
management
di
due
canili
‘
no
‐
kill
’
in
Italia
centrale:
utilizzo
di
un
sistema
di
‘
population
medicine
’
nel
corso
di
tre
anni
Riassunto
Lo Stato Italiano prevede, quali mezzi per controllare la popolazione dei cani vaganti sul territorio, la sistematica identificazione dei cani di proprietà, il controllo delle nascite mediante sterilizzazione ed azioni educative sulla cittadinanza. Fin dal 1991 l’eutanasia dei cani privi di proprietario è consentita solo per soggetti gravemente malati o di comprovata pericolosità. I cani catturati sul territorio, se non immediatamente riconducibili ad un proprietario, vengono accolti in canili rifugio a lungo termine, dove finiscono per trascorrere la maggior parte della loro vita, spesso in situazioni ambientali discutibili. La gestione sanitaria di queste strutture può risultare molto
difficoltosa, considerando il costante aumento dei cani in ingresso, scarsamente controbilanciato da un numero sufficiente di adozioni. L’Istituto Zooprofilattico Sperimentale dell’Abruzzo e del Molise ‘G. Caporale’ (IZS A&M) gestisce due canili rifugio siti a Teramo, applicando un modello centrato sulla sistematica rilevazione di parametri clinici e comportamentali. I dati ottenuti dagli esami di laboratorio ad essi associati vengono raccolti in uno specifico database per essere analizzati secondo un approccio di ‘population
medicine’ (gestione sanitaria di una popolazione animale confinata), al fine di identificare i ‘traguardi produttivi’ e migliorare la condizione di benessere degli animali. In questo studio retrospettivo sono stati descritti i dati raccolti durante un periodo di tre anni. La prevalenza e l’incidenza delle diverse patologie/lesioni sono state calcolate al fine di raggiungere risultati migliori attraverso azioni mirate al miglioramento continuo delle condizioni strutturali, gestionali ed organizza‐ tive. Non sono stati ammessi nuovi cani in canile fin dal 2005: in questo ideale ‘sistema chiuso’ è stato possibile verificare i reali effetti dell’applica‐ zione del nostro sistema gestionale, in assenza dei variabili ed imprevedibili rischi di introduzione di nuove patologie dall’ambiente esterno. Sono state effettuate valutazioni statistiche; le principali differenze sono state evidenziate tra il 2006 ed il 2007, in modo particolare per le ferite da morso, le lesioni cutanee e le patologie dell’apparato locomotore. Pertanto, l’impiego del sistema gestionale descritto nel presente lavoro è risultato in un effettivo miglioramento delle condizioni di salute e, conseguentemente, di benessere dei cani presenti nei canili sottoposti allo studio, come indicato dalla significativa riduzione della prevalenza e dell’incidenza delle principali classi di patologie dal 2006 al 2007. Altri significativi miglioramenti sono stati evidenziati nel controllo della leishmaniosi, una zoonosi endemica la cui prevalenza nei canili ha subito una netta riduzione nel corso dei tre anni ai quali si riferisce il nostro studio retrospettivo.
Parole chiave
Animale, Benessere, Cane, No‐kill, Manage‐
ment, Population medicine, Rifugio.
Introduction
In Italy, companion animal welfare and urban animal control are managed by the competent
authorities (municipalities and veterinary
services), in accordance with national and local regulations. In particular, regional laws were promulgated after the adoption of national
framework legislation 281/1991 (1) which
prescribes general principles in this field. These laws stipulate that canine population control be pursued through the identification of dogs using microchips so as to discourage the abandonment of animals and through the capture and sterilisation of unwanted dogs. Unwanted animals cannot be euthanised or used for scientific purposes and their future management is decided in accordance with the provisions of the various regional regulations. In most cases, after identification and surgical sterilisation, dogs are placed in long‐term shelters where they remain until adoption or death. In Italy, dogs can only be euthanised if they have an incurable condition or are proven to be dangerous (30). This does not happen in many other countries, where euthanasia is routinely employed to control overcrowding and disease (7, 9, 25, 32). Some regional laws, such as those that govern the Abruzzo region, also utilise the catch‐neuter‐release option (2, 3, 4, 5, 6). This formally recognises the so‐
called ‘block dog/community dog’ as a
years in overcrowded shelters. The
Companion Animal Welfare Council
recommends euthanising animals that show
abnormal behaviour and in cases where
relocation to a more suitable environment is not feasible or would cause unacceptable suffering (10). In Italy, since these options are not available, we attempt to provide the best possible level of welfare to sheltered dogs in accordance with the ‘five freedoms’, widely recognised as baseline criteria to guarantee physical health, freedom from disease and pain and distress and the provision of behavioural and environmental needs for the animals (10). To achieve these objectives, a strategy of continuous improvement in shelter management systems is essential. This should
include consideration of how to manage
increasing numbers of aged, non‐adoptable dogs in a situation of limited resources.
We propose that an innovative approach to canine health management be adopted, in line with the concept of ‘shelter medicine’ which could be viewed as ‘small animal herd health’ or a form of population medicine (24). Population medicine (as it relates to both companion and production animals) is based on setting production goals, identifying risk factors for disease, preventing disease and
maximising production. Production goals,
which are well defined for farm animals, are different from those for companion animals where the main ‘production’ goal is an acceptable level of welfare and consideration of the incidence and prevalence of clinical and behavioural disease. According to Hurley (24), it is possible to establish performance measures in an animal shelter using the example of a dairy herd. For example, to identify objectives and achieve better results, the incidence and prevalence of disease or the number of adopted animals can be considered. In such a system, record keeping is of a paramount importance, so that major risks can be easily identified and eliminated.
In this retrospective study, the employment of a ‘population medicine’ system, over a three‐ year period in two ‘no‐kill’ and limited admission dog shelters is described. New dogs were not admitted from June 2005 onwards,
which made it possible to apply population medicine practices in a ‘closed system’. This ‘ideal’ condition provided an opportunity to investigate the effects of the application of a rational population medicine system, where all changes in the health status of the dogs could be related to either the management or slight reduction in the number of dogs over time. Data on the prevalence and incidence of different pathological conditions recorded over
three consecutive years (2005‐2007) is
described and discussed. The differences
between the two kennels and the
improvements achieved during these years are highlighted.
Materials
and
methods
Animals
The study was conducted in two long‐term canine shelters managed by the Istituto Zooprofilattico Sperimentale dell’Abruzzo e del Molise ‘G. Caporale’ (IZS A&M), both located in Teramo (Abruzzo, Italy), one in contrada Gattia, 265 m above sea level (kennel A) and one in contrada Carapollo, 205 m above sea level (kennel B). In 2007, a total of 204 dogs were given shelter in kennel A (229 in 2005, 219 in 2006). In kennel B, 360 dogs were given shelter in 2007 (401 in 2005, 373 in 2006). All individuals were neutered or spayed. The two kennels were structurally very different; kennel A had been built more recently and was better designed than kennel B.
Kennel A dogs generally lived in pairs and were allowed out to exercise for two hours each day in specific fenced areas. In contrast, kennel B dogs were kept indoors, in pens of different sizes (that housed between 4 to 7 dogs). The number of animals in each pen was decided according to the area of the pen. However, particularly in 2005 and 2006, many pens routinely sheltered more than 10 animals. Both kennels had facilities with rehabilitation
areas where dogs were treated (wound
Shelter
management
The IZS A&M has always tried to employ the same kind of management in both kennels, despite the structural differences. Standard operating procedures (SOPs) were regularly updated, according to an internal quality system. Moreover, all major activities had been planned since 2005 for both kennels. Daily
management was performed in accordance
with the most recent available knowledge on canine behaviour. Central to this was the belief that in every shelter, dogs should live in an
adequate physical and psychological
environment, as social isolation and restricted
space promote stress, with consequent
undesirable behavioural changes (8). In the past, shelter animals were traditionally housed in single boxes or cages to prevent disease spread and to avoid fighting (26, 27). Studies of group‐ and individually housed shelter
dogs revealed that group‐housed dogs
vocalised less, were more active, showed less inter‐dog aggression, no stereotypes and fewer
behavioural problems in comparison with
individually housed dogs. Furthermore,
group‐housed dogs also had fewer
behavioural problems after adoption and re‐ homing (28). Social isolation or restriction is considered a major stressor for social species, such as the dog (37). As stated above, in kennel A, dogs confined in boxes are released into exercise areas once a day for two hours together with dogs from other boxes, so as to give them a better social and physical environment, albeit for a limited period of time. This practice is believed to contribute to the improvement of dog welfare (36). In kennel B, all dogs were kept in pens, so the presence of exercise pens was not considered crucial.
In both kennels, operators were instructed on how to interact with the dogs (playing, walking on a leash and appropriate verbal and tactile contact). Human/animal interaction is considered to be a good tool to reduce stress in
kennelled dogs, which also reduces
behavioural problems and increases the overall adoption rate (26).
Other studies have shown that interaction with humans can reduce the stress response in shelter dogs (12, 19, 20). Social isolation is believed to be the most stressful factor in a kennel and people are an important resource for sheltered dogs, particularly for dogs that are housed singly (11, 12, 22).
A balanced diet is also of utmost importance to prevent health disorders, but it has also been demonstrated that a combination of human interaction and high quality diet can positively affect the behaviour of kennelled dogs (21). Studies have shown differences in dogs that were subjected to a programme of regular
supplemental human interaction and
differential diets (maintenance versus
premium quality). Results suggested that both human interaction and a high quality diet had moderating effects on hypothalamic‐pituitary‐ adrenal (HPA) axis activity. In kennels A and B, the same maintenance quality dog food was used but was administered in different ways.
In kennel A, food was administered
individually to each dog and with regard to the animal’s size. In kennel B, because of the ratio of carers to the number of dogs, food was administered ad libitum in common feeding troughs. It should be noted that in both kennels, dogs on a prescribed veterinary diet were always fed individually.
To increase the number of adoptions and to minimise the risk of reassignment (29, 31, 34), attention was paid to the behavioural training of dogs. Veterinarians and dog trainers managed risky behaviour, such as bites and aggression with ad hoc training sessions. Temperament tests were applied to all dogs to identify aggressive individuals which were then removed from the adoption pools. In kennel A, adoptable dogs were placed in pens with good exposure to visitors. Wells and
Hepper noted that kennelled dogs
(particularly ‘single‐box’ dogs) spent most of their time in the rear of their boxes, which did not encourage adoption (35). Following work by Marston and Bennett (26), dogs in the adoption pool had their daily food supply placed outside the run and potential adopters were encouraged to feed them. This approach
encouraged the animal to the front of the kennel run.
Health
data
collection
The health of the dogs was managed using a model developed by the IZS A&M which utilised a database recording system to collect relevant animal health data. A Microsoft Access database (Microsoft® Corporation) was
specifically designed for this purpose.
Under the requirements of Italian law (1, 4), new dogs can only be admitted to long‐term shelters from ‘healthy’ shelters where they
have previously been identified with a
microchip, recorded on the regional register and neutered. When the dogs arrived at kennel A or B, a registration number for internal use was assigned to each animal and all known data was entered into the database. New dogs were left alone in a single box during the ‘adaptation period’ (seven days) and were physically examined and received anti‐parasitic treatment and their behaviour
was profiled. Based on the information
available, veterinarians and dog trainers then
allocated individual dogs to the most
appropriate group.
Data was originally collected in hard copy format and then entered into the database. A single form was given to each operator working in the kennel. This form (‘reporting disease symptoms’) (Fig. 1) was divided into two parts. One area (white) was completed by kennel operators when they noted signs of a possible disease incident. This part of the form was designed for simplicity, with checklists of the most frequent canine disease symptoms and a diagram of a dog’s body on which the operator could identify the location of any visible lesions. Space was also provided to enable the operator to communicate relevant information about the dog (e.g. anamnesis, anomalies). The operator was required to sign the sheet so that he/she could be contacted in case further details were required. These forms were used by veterinarians during their twice daily routine kennel checks. Any referred animals were subsequently examined.
Veterinarians completed the second part of the form (grey) with the results of any physical examinations, prescribed therapy, the need for possible additional or specialist examinations or testing (e.g. X‐rays), prognosis and the date of the next examination. The veterinarian also completed a second form (‘therapy form’) (Fig. 2), where information on any therapy administered (e.g. drugs, doses, duration of the therapy) was provided. This form was
designed to assist operators with drug
administration (always conducted under
veterinary control). Completed forms were collected at the end of each month and data were entered into the database. At the same time, a digital photo of each dog was included in the database. At the end of the month, data on all diagnosed cases were extracted from the database in order to calculate parameters such as disease incidence and prevalence (23). This
was done to identify the degree of
compatibility with the main production goal
which was to reduce the frequency of
pathological conditions resulting from adverse health and social problems and the factors associated with such conditions (e.g. injuries or behaviour associated with kennel design, dog grouping criteria, etc.). As a basic policy, blood from each dog was tested at least once a year
for haemachrome, clinical chemistry and
protidogram and serologically tested for
Leishmania infantum which was endemic in the region (17). These results were also entered
into the database. The prevalence of
L. infantum had been calculated on a monthly basis since 2004 and continued to be evaluated from 2005 to 2007, to address management of disease within the kennels. As a preventive
measure, anti‐parasitic treatment was
administered regularly during the spring and summer. In addition, specific drugs against disease vectors (imidacloprid/pemethrin) were administered, thorough cleaning of the kennel was undertaken regularly and treatment with
antimonial drugs, allopurinol or metro‐
RNDog Name Chip
Date _____ / _____ / _____ Kennel: A B No. pen/box
NB: The area in white is for the operator, the area shaded in grey is for the veterinarian
Intensity Low Medium High
Cause Bite Environment Dermatitis Neoplasia Other
Intensity Low Medium High
Intensity Low Medium High
Operator Date / /200_
Left Right
Date __ / __ / __ Veterinarian Symptoms, diagnosis
Therapy Prognosis (days)
Additional examinations or tests
Weight loss
Notes Claudication
Pain
Apathy
Abnormal behaviour Vomiting
Inappetence
Re porting dise a se symptoms
Other Coughing Abnormal hair or skin
Otitis
Nasal discharge
Ocular discharge Abnormal faeces
Figure 1
RNDog Microchip Name Kg Box-Pen Year Sheet No. __________
Treatment Dosage From (date) To (date) Vet Diagnosis
1)
2)
3)
4)
5)
Date 1 2 3 4 5 Date Note Vet
Figure 2 Therapy form
Results
Since January 2005, the system described above was applied to all dogs in kennels A and B. All data described were collected and entered into the database. A SPSS software program (SPSS 16.0, SPSS Inc., Chicago) was used to perform statistical analysis.
As stated above, the number of sheltered dogs reduced slightly and progressively during the three years under consideration. This was because the initial lack of space in both kennels in year one (2005) meant that they were turned into ‘limited admission’ shelters, with no new dogs being admitted from June 2005. Since that time, an annual reduction of about 5% of the canine population was observed, mainly due to the success of adoption campaigns. This reduction resulted in a slight increase in the ratio of operator working hours/dog. In 2005, these were 0.12 h/dog per day in kennel A and 0.07 h/day in kennel B. In 2007 the ratios were 0.13 and 0.08, respectively.
The age of the dogs was usually unknown. However, it was believed that in 2005, the majority (>60%) ranged from 3 to 7 years old in kennel A and from 5 to 9 years old in kennel B.
Considering the absence of newly admitted dogs from June 2005, there were no changes to these figures during the study (with the exception of the three years of natural aging of
the population). Male/female ratios also
remained stable, with about two males to three females in kennel A and one male to two females in kennel B.
The mean space available for each dog differed between kennels and in both cases increased progressively. In kennel A (considering both
boxed and fenced areas), there were
3.93 m2/dog in 2005, 4.10 m2/dog in 2006,
4.41 m2/dog in 2007. In kennel B, mean values
were 3.24 m2/dog in 2005, 3.48 m2/dog in 2006
and 3.61 m2/dog in 2007.
Prevalence and incidence of different lesions were calculated each year; χ2 (Chi‐square) and
Table I
Prevalence of most frequent classes of diseases observed in kennels A and B
2005 2006 2007 Disease/disorder
Total ‘A’ ‘B’ Total ‘A’ ‘B’ Total ‘A’ ‘B’
Bite wounds 11.42% 9.60% 12.46% 13.68% 12.32% 14.47% 7.97% 8.33% 7.77%
Skin disease 8.25% 8.29% 8.22% 10.13% 8.21% 11.26% 6.20% 6.37% 6.11%
Otitis 4.28% 1.31% 5.98% 6.25% 2.73% 8.31% 3.54% 0.49% 5.27%
Diseases/disorders of the
locomotor apparatus 3.49% 3.05% 3.74% 6.92% 4.56% 8.31% 3.88% 2.94% 4.44%
Ocular disease 2.06% 2.62% 1.74% 2.02% 0.45% 2.94% 1.24% 0.98% 1.38%
Neoplasiae* 1.90% 2.62% 1.49% 1.52% 0.91% 1.87% 3.19% 1.47% 4.16%
Respiratory disease 1.58% 0.49% 2.24% 4.89% 4.56% 5.09% 1.41% 2.94% 0.55%
Gastrointestinal disease 1.42% 0.87% 1.74% 1.52% 1.36% 1.60% 1.41% 0.49% 1.94% Genital/urinary disease 0.95% 0.87% 0.99% 1.18% 0.91% 1.34% 1.24% 0.49% 1.66%
Oral disease 0.47% 0.00% 0.47% 1.18% 0.91% 1.34% 0.88% 0.49% 1.11%
* neoplasiae from every apparatus are included in this class
Table II
Incidence of the most frequent classes of diseases observed in kennels A and B
2005 2006 2007 Disease/disorder
Total ‘A’ ‘B’ Total ‘A’ ‘B’ Total ‘A’ ‘B’
Bite wounds 11.78% 9.82% 12.91% 13.98% 12.79% 14.67% 8.15% 8.45% 7.97%
Skin disease 8.51% 8.48% 8.52% 10.36% 8.53% 11.41% 4.71% 4.97% 4.55%
Otitis 4.41% 1.33% 6.20% 6.39% 2.84% 8.42% 1.18% 0.49% 2.56%
Diseases/disorders of the
locomotor apparatus 3.60% 3.12% 3.87% 7.25% 4.73% 8.42% 3.07% 1.99% 3.70%
Ocular disease 2.12% 2.67% 1.80% 2.07% 0.47% 2.98% 1.26% 0.99% 1.42%
Neoplasiae* 1.96% 2.67% 1.55% 1.20% 0.94% 1.35% 2.71% 0.99% 3.70%
Respiratory disease 1.63% 0.44% 2.32% 5.00% 4.73% 5.16% 1.44% 2.84% 0.56%
Gastrointestinal disease 1.47% 0.89% 1.80% 1.55% 1.42% 1.63% 1.44% 0.49% 1.99%
Genital/urinary disease 0.98% 0.89% 1.03% 1.20% 0.94% 1.35% 1.26% 0.49% 1.70%
Oral disease 0.49% 0.00% 0.77% 1.20% 0.94% 1.35% 0.90% 0.49% 1.13%
* neoplasiae from every apparatus are included in this class
0 2 4 6 8 10 12 14
2005 2006 2007
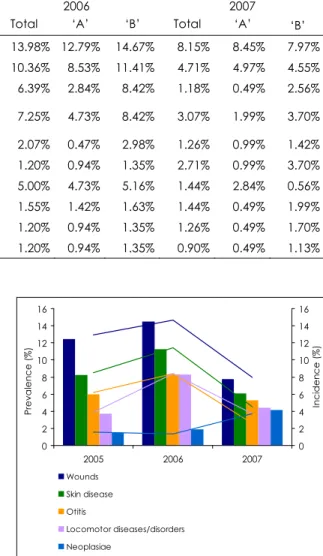
Pre v a len ce ( % ) 0 2 4 6 8 10 12 14 In c id e n c e ( % ) Wounds Skin disease Otitis Locomotor diseases/disorders Neoplasiae Figure 3
Prevalence (bars) and incidence (lines) of the major classes of pathology studied in kennel A
0 2 4 6 8 10 12 14 16
2005 2006 2007
Prev a len ce ( % ) 0 2 4 6 8 10 12 14 16 In c id e n c e ( % ) Wounds Skin disease Otitis Locomotor diseases/disorders Neoplasiae Figure 4
Bite wounds showed the highest prevalence and incidence, followed by skin lesions and pathologies of the locomotor apparatus, as shown in Tables I and II. Significant annual differences (p<0.05) in the incidence and
prevalence of lesions were reported in
kennel B. Incidence (χ2=7.97, p=0.004) and
prevalence (χ2=8.28, p=0.004) of bite wounds
from 2006 to 2007 in kennel B, incidence (χ2=11.38, p=0.001) and prevalence (χ2=6.09,
p=0.01) of skin lesions from 2006 to 2007, incidence (χ2=11.74, p=0.001) of otitis from 2006
to 2007, incidence (χ2=6.97, p=0.008) and
prevalence (χ2=4.56, p=0.03) of locomotor
apparatus pathologies from 2006 to 2007, incidence (χ2=4.05, p=0.04) of neoplasiae from
2006 to 2007. No other significant differences were highlighted from 2006 to 2007 or from 2005 to 2006.
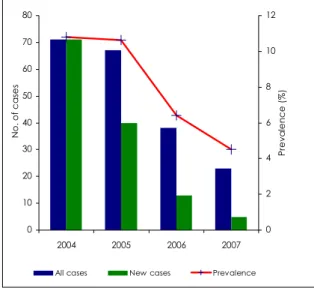
With regard to L. infantum, positive cases were recorded since 2004. Data on positive dogs from 2004 to 2006 from the entire dog population present in both kennels (33) were combined with results from 2007 and are presented in Table III, along with serological
antibody concentrations and corresponding
prevalence by year. Improvements from 2004 to 2007 are detailed in Figure 5. During the three‐year period under study, there was a significant reduction in the prevalence of positive cases (χ2=18.23; p=0.000).
Discussion
Results collected during the first year of the study (2005), were probably influenced by the need of the operators to become familiar with
the new system, as forms were not
systematically filled in initially. For this reason, the number of ‘reporting disease symptoms’ forms collected in 2005 (280 vs 412
in 2006 and 360 in 2007) were probably not indicative of the health conditions of all kennelled dogs during that year. However, the system gained efficiency throughout 2005 and could be considered fully operational by 2006. Improvements in the prevalence and incidence of different classes of pathological conditions, as noted by progressive reductions, were recorded between 2006 and 2007, particularly in kennel B, possibly due also to the redistribution of dogs.
Inside our ‘closed system’, all changes in the health conditions of the dogs during the three‐ year period could be associated primarily to the employment of a rational management system, in particular: pathology classes and incidence and prevalence information were regularly studied to identify causes and remove them. The reduction in dogs, due to restricted intake and to adoption initiatives, also had an important impact, but probably this reduction would not have been as
0 10 20 30 40 50 60 70 80
2004 2005 2006 2007
No
. o
f c
a
se
s
0 2 4 6 8 10 12
Pr
ev
a
len
ce
(
%
)
All cases New cases Prevalence
Figure 5
Cases (>1:80) and prevalence of Le ishma nia
infa ntum from 2004 to 2007
Table III
Prevalence of Le ishma nia infa ntum, 2004-2007
No. of infected dogs Serological
antibody 2004 2005 2006 2007
≥1:640 20 28.2% 18 26.9% 2 5.3% 1 4.4%
1:320 17 23.9% 5 7.7% 7 18.4% 8 34.7%
1:160 18 25.4% 19 28.3% 8 21.0% 5 21.8%
1 :80 16 22.5% 25 37.3% 21 55.3% 9 39.1%
significant without regular ethological studies and proper grouping criteria. Results from the
population medicine system constantly
determined our actions, including the ‘social’ activities which were made possible mainly by the progressive reduction of the total dog population. On this basis, in 2007, new and smaller groups were created in kennel B, as a result of a high prevalence of bite wounds recorded in 2006. The improvement in the ratio of operators’ working hours/dog was likewise critical in improving the daily management of the dogs. The reduction in the number of bite wounds in kennel B between 2006 and 2007 was statistically significant (14.47% to 8.33%;
χ2=8.28, p=0.004), while that in kennel A was
not (12.32% to 8.33%; χ2=1.81, p=0.17).
In general, kennel B, which was less organised, seemed to have benefited more from the reduction in dog population and subsequent pen rearrangements. Nearly all lesion classes reduced sharply in incidence and prevalence from 2006 to 2007 in kennel B (Fig. 4). Skin lesions in particular showed reduced incidence (2007=4.55%, 2006=11.41%, χ2=11.38, p=0.001)
and prevalence (2007=6.11%, 2006=11.26%,
χ2=6.09, p=0.01). In the same kennel, otitis and
locomotor apparatus lesions also showed a sharp decline, particularly in incidence: the former from 8.42% to 2.56% (χ2=6.97, p=0.008)
and the latter from 8.42% to 3.70% (χ2=6.97,
p=0.008). Regarding otitis, the decreasing
tendency could have been due to the
systematic use of antibiotics (local and/or parenteral administration) after sensitivity
tests, if warranted. Similar but minor
improvements were recorded in kennel A
(Fig. 3), where the reduction in dog population was probably of lesser impact, considering the better structures and the larger areas available to animals.
Tumour data from kennel B were particularly interesting, as these were the only classes of pathology in which incidence significantly increased from 2006 to 2007 (1.35% to 3.70%;
χ2=4.05; p=0.04). In contrast, only a slight
increase was recorded in kennel A (0.94% to 0.99%, χ2=0.00; p=0.96, not significant). These
results were greater than those reported in a
study on the total non‐kennelled dog
population in Great Britain (13), where total
tumour incidence was reported to be
2.54%/year. In this study, the percentage of neoplasiae of lymphoid tissues was most
unusual: post‐mortem examinations showed
that in kennel B over 20% of all new tumours (3 cases out of 13) diagnosed in 2007 were
haemo‐lymphopoietic neoplasiae (lymphoma),
with a yearly incidence of 0.85%. In the study
referred to above (13), these tumours
accounted for only 5.2% of the total, with a yearly incidence of 0.13%, approximately six times less than in kennel B. Epidemiological studies are required to clarify this matter.
Noticeable improvements were made in
L. infantum control throughout the three‐year
retrospective study period. This endemic
zoonotic disease was managed by using
specific drugs against disease vectors
(imidacloprid/pemethrin), environmental
hygiene and treatment with antimonial drugs, allopurinol or metronidazole which led to a major reduction in the prevalence to 3.70% in 2007, from 10.63% in 2005 (χ2=18.23; p=0.000).
The mean regional prevalence outside the kennels remained between 10% and 20% (17).
Conclusions
A good canine shelter management
programme is important to maximise the
quality of life of unwanted dogs in a confined and restrictive environment. Italian laws do not currently foresee euthanasia as a suitable method to control shelter populations; so many dogs spend most, if not all, of their life in confinement. In the future, this situation could extend to other countries, considering the increasing demand for ‘no‐kill’ laws from both within Europe and abroad (15, 16). Growing public awareness of the welfare of dogs in shelters is gaining momentum and attention to ethological needs must now be considered as an integral part of canine shelter
management operations.
be linked to good general management. Efficient record keeping is fundamental to identify ‘production’ goals (e.g. reduction of prevalence and incidence of different diseases) and achieve better welfare standards. The employment of a ‘population medicine’ system in the kennels studied has made it possible to focus on both managerial and medical actions,
resulting in significant improvements in
animal health and welfare, as shown by a reduction in the prevalence and incidence of different classes of pathology. The presence of a ‘closed system’ without external influences (e.g. introduction of infectious disease from new puppies) made it possible to associate
these improvements with the actions
performed following the indications of the
population medicine database. To achieve
these results, the reduction in animal numbers
was an opportunity that enabled the
redistribution of animals in pens/boxes
according to their social needs, in the light of
results from data collection. The challenge now is to make further improvements through the collection of other types of data, such as those derived from the use of ambulatory monitors and video recordings, as suggested by Harris et al. (18). Such an approach could help to solve or prevent behavioural problems caused by the shelter environment itself. More data can be studied with a risk analysis approach to identify critical points and control them. This could be particularly useful in an ‘open
system’; population density, cleaning
techniques, air exchange and turnover rates are recognised to be critical environmental issues in an ‘open’ dog shelter system (14). In this context, information from the internal
population medicine database, which our
study demonstrated to be important to identify and remove risks related to the daily management of a ‘closed’ kennel, could be combined with data from other critical points to deal with the threat of new diseases.
References
1. Anon. 1991. Legge 14 agosto 1991, n. 281. Legge quadro in materia di animali d’affezione e prevenzione del randagismo. G a zz Uff, 203, 30 August.
2. Anon. 1995. Legge Regionale del 3 aprile 1995 n. 12. Interventi per la tutela degli animali d’affezione e prevenzione del randagismo. Bo ll UffRe g Pug lia, 39, 18 April.
3. Anon. 1997. Legge Regionale 21 ottobre 1997, n. 34. Tutela degli animali d’affezione e prevenzione del randagismo. Bo ll UffRe g La zio, 30, 30 October.
4. Anon. 1999. Legge regionale 21 settembre 1999, n. 86. Norme sul controllo del randagismo, anagrafe canina e protezione degli animali da affezione. Bo ll UffRe g Ab ruzzo, 39, 13 October. 5. Anon. 2001. Legge regionale 24 novembre 2001, n. 16. Tutela degli animali d’affezione e
prevenzione del randagismo. Bo ll UffRe g C a mp a nia, Speciale, 29 November.
6. Anon. 2001. Ministero della Sanità. Circolare 14 maggio 2001, n. 5. Attuazione della legge 14 agosto 1991 n. 281. G a zz Uff, 144, 23 June.
7. Bartlett P.C., Bartlett A., Walshaw S. & Halstead S. 2005. Rates of euthanasia and adoption for dogs and cats in Michigan animal shelters. J Ap p l Anim We lf Sc i, 8, 97-104.
8. Beerda B., Schilder M.B., van Hooff J.A., de Vries H.W. & Mol J.A. 1999. Chronic stress in dogs subjected to social and spatial restriction. I. Behavioural responses. Physio l Be ha v, 66, 233-242. 9. Clevenger J. & Kass P.H. 2003. Determinants of adoption and euthanasia of shelter dogs spayed or
neutered in the University of California veterinary student surgery program compared to other shelter dogs. J Ve t Me d Educ, 30, 372-378.
10. Companion Animals Welfare Council (CAWC) 2004. The report on companion animal welfare
establishments: sanctuaries, shelters and re-homing centres. CAWC, Bourn, Cambridge, 59 pp (www.cawc.org.uk/sites/default/files/CAWCRepsanctuaries.pdf accessed on 26 May 2008).
11. Coppinger R. & Zuccotti J. 1999. Kennel enrichment: exercise and socialization of dogs. J Ap p l Anim
We lf Sc i, 2, 281-296.
12. Coppola C.L., Grandin T. & Enns R.M. 2006. Human interaction and cortisol: can human contact reduce stress for shelter dogs? Physio l Be ha v, 87, 537-541.
14. Ford R.B. 2004. Vaccination strategies in the animal shelter environment. In Shelter medicine for veterinarians and staff (L. Miller & S. Zawistowski, eds). Blackwell Publishing Professional, Oxford, 285-304.
15. Frank J. 2004. An interactive model of human and companion animal dynamics: the ecology and economics of dog overpopulation and the human costs of addressing the problem. J Hum Ec o l, 32, 107-130.
16. Frank J. & Carlisle-Frank P. 2003. Companion animal overpopulation: trends and results of major efforts to reach a ‘no-kill’ nation. In Proc. Annual meeting of the American Sociological Association (ASA), Atlanta Hilton Hotel, 16 August, Atlanta. ASA, Washington, DC (www.allacademic.com/ meta/p107788_index.html accessed on 26 May 2008).
17. Gradoni L., Gramiccia M., Khoury C. & Maroli M. 2004. Linee guida per il controllo del serbatoio canino della leishmaniosi viscerale zoonotica in Italia. Rapporti ISTISAN 04/12. Istituto Superiore di Sanità, Dipartimento di Malattie Infettive, Parassitarie ed Immunomediate, Rome, 20 pp (www.iss.it/publ/rapp/cont.php?id=20&tipo=5&lang=1&ccss=000 accessed on 26 May 2008).
18. Harris P.J., Schaare P.N., Cook C.J. & Henderson J.D. 2001. An ambulatory physiological monitor for animal welfare studies. C o mp ut Ele c tro n Ag ric, 31, 181-194.
19. Hennessy M.B., Davis H.N., Williams M.T., Mellott C. & Douglas C.W. 1997. Plasma cortisol levels of dogs at a county animal shelter. Physio l Be ha v62, 485-490.
20. Hennessy M.B., Miller D.D., Douglas C.W., Voith V.L. & Williams M.T. 1998. Influence of male and female petters on plasma cortisol and behaviour: can human interaction reduce the stress of dogs in a public animal shelter. Ap p l Anim Be ha v Sc i, 61, 63-77.
21. Hennessy M.B., Voith V.L., Hawke J.L., Travis B.S., Young T.L., Centrone J., McDowell A.L., Linden F. & Davenport G.M. 2002. Effects of a program of human interaction and alterations in diet composition on activity of the hypothalamic-pituitary-adrenal axis in dogs housed in a public animal shelter.
J Am Ve t Me d Asso c, 221, 65-91.
22. Hubrecht R.C. 1993. Dog housing and welfare. Universities Federation for Animal Welfare (UFAW), Animal Research Report No 6, Potters Bar, 13 pp.
23. Hurley K.F. 2004. Disease recognition and diagnostic testing In Shelter medicine for veterinarians and staff (L. Miller & S. Zawistowski, eds). Blackwell Publishing Professional, Oxford, 307-314.
24. Hurley K.F. 2004. Implementing a population health plan in an animal shelter: goal setting, data collection and monitoring, and policy development. In Shelter medicine for veterinarians and staff (L. Miller & S. Zawistowski, eds), Blackwell Publishing Professional, Oxford, 211-234.
25. Lepper M., Kass P.H. & Hart L.A. 2002. Prediction of adoption versus euthanasia among dogs and cats in a California animal shelter. J Ap p l Anim We lf Sc i, 5, 29-42.
26. Marston L.C. & Bennett P.C. 2003. Reforging the bond – towards successful canine adoption. Ap p l
Anim Be ha v Sc i83, 227-245.
27. Marston L.C., Bennett C. & Coleman G.J. 2005. What happens to shelter dogs? Part 2. Comparing three Melbourne welfare shelters for nonhuman animals. J Ap p l Anim We lf Sc i, 8, 25-45.
28. Mertens P.A. & Unshelm J. 1996. Effects of group and individual housing on the behaviour of kennelled dogs in animal shelters. Anthro zo o s, 9, 40-51.
29. Mondelli F., Prato Previde E., Verga M., Levi D., Magistrelli S. & Valsecchi P. 2004. The bond that never developed: adoption and relinquishment of dogs in a rescue shelter. J Ap p l Anim We lf Sc i, 7, 253-266.
30. Passantino A., Fenga C., Morciano C., Morelli C., Russo M., Di Pietro C. & Passantino M. 2006. Euthanasia of companion animals: a legal and ethical analysis. Ann Ist Sup e r Sa nità, 42, 491-495. 31. Patronek G.L., Glickman L.T., Beck A.M., McCabe G.P. & Ecker C. 1996. Risk factors for
relinquishment of dogs to an animal shelter. J Am Ve t Me d Assoc, 209, 572-581.
32. Peracho V., Villalbi J.R., Llebaria X., Armengou J.M. & Guix J. 2003. De la perrera municipal al centro de acogida de animales de compañía de Barcelona [From the municipal dog pound to the pet shelter in Barcelona, Spain]. G a c Sa nit, 17, 515-519 (www.scielo.br/pdf/gs/v17n6/notacampo2.pdf accessed on 26 May 2008).
34. Salman M.D., Hutchinson J., Ruch-Gallie R., Kogan L., New J.G. & Kass P.H. 2000. Behavioural reasons for relinquishments of dogs and cats to 12 selected shelters in the United States. J Ap p l Anim We lf Sc i,
3, 96-101.
35. Wells D.L. & Hepper P.G. 1992. The behaviour of dogs in a rescue shelter. Anim We lfa re, 1, 171-186. 36. Wells D.L. & Hepper P.G. 1998. A note of the influence of visual conspecific contact on the
behaviour of sheltered dogs. Ap p l Anim Be ha v Sc i, 60, 83-88.