Arq Neuropsiquiat r 2002;60(4):1000-1002
PATHOLOGICAL LAUGHTER IN A PATIENT
WITH TRIGEM INAL NEURINOM A
André G. M achado
1,
Paulo Henrique Aguiar
2, Raul M arino Jr
3ABSTRACT - We present a 47-year-old w oman w it h a long hist ory of anxiet y and a more recent hist ory of shock-like facial pain and episodes of laught er w it hout any mot ivat ion. She could not explain t he laughing burst s and did not have a sense of mirt h preceding it . On neurological examinat ion she present ed a VI nerve palsy and t rigeminal hypoest hesia (V2 and V3) on t he right side. M agnet ic resonance imaging exhibit ed a large cyst ic lesion on t he right m iddle f ossa causing signif icant com pression on t he brain st em . A front oorbit ozygomat ic and pret emporal combined approach w as performed. During int ra and ext radural explorat ion a large t umor w as found on t he t rigeminal nerve. The w hole lesion w as resect ed, revealing t o be a neurinoma on pat hological exhaminat ion. She maint ained a VI nerve palsy but had complet e remission of t he unmot ivat ed laughing episodes during t he one year follow up.
KEY WORDS: pat hological laught er, neurinoma, t rigeminal neuralgia.
Riso patológico em uma paciente com neurinoma de trigêmeo
RESUM O - Relat amos o caso de uma pacient e de 47 anos com hist ória de longa dat a de ansiedade que apresent ou início de dor facial em choques do lado direit o e episódios de riso sem mot ivação. Ela não podia explicar os episódios de riso e não percebia uma sensação de graça que os precedia. Ao exame neurológico apresent ava paresia do VI nervo e hipoest esia no t rajet o dos ramos oft álmico e maxilar do t rigêmeo. A ressonância magnét ica de encéfalo apresent ava uma lesão císt ica na fossa média direit a causando significat ivo efeit o de massa sobre o t ronco encefálico. Um acesso combinado front o-orbit o-zigomát ico e pré-t emporal foi realizado e a exploração int ra e ext ra-dural revelou um grande t umor no nervo t rigêmeo. Toda a lesão foi ressecada, revelando ser um neurinoma no exame pat ológico. A pacient e mant eve a paresia de VI nervo mas apresent ou remissão complet a dos episódios de riso imot ivado durant e o seguiment o de um ano.
PALAVRAS-CHAVE: riso pat ológico, neurinoma, neuralgia t rigeminal.
Division of Neurosurgery, Hospit al das Clínicas, Universit y of São Paulo M edical School, São Paulo SP, Brazil: 1Resident Physician; 2Assist ant Physician; 3Chairman.
Received 4 January 2002, received in final form 29 M ay 2002. Accept ed 10 June 2002.
Dr. André Guelman Gomes M achado - Rua M aranhão 531/121 - 01240–903 São Paulo SP - Brasil. E-mail: aggmachado@yahoo.com
Pat hological laught er is a condit ion associat ed w it h neurological lesions at various levels. Several structures have been involved as parts of the pathw ay responsible f or t he expression of laught er. There seems t o be no cort ical cent er for t he cont rol of laught er, but t he mot or, premot or and sensory areas are involved in t he volunt ary cont rol. Subcort ical st ru ct u res su ch as t h e h ip p o ccam p u s an d t h e dent eat e girus have been implicat ed as w ell1. The hypot halamus plays a cent ral role in t he cont rol and expression of emot ions, one of w hich is laught er. It receives af f erences f rom cort ical and subcort ical st ruct ures w hich w ork as modulat ors of emot ional r esp o n ses. Di f f u se l esi o n s t h at i n t er r u p t t h e cort icohypot halam ic t ract s produce neurological synd rom es m arked b y loss of cont rol over t he emot ional expressions, such as pseudobulbar palsy2.
Arq Neuropsiquiat r 2002;60(4) 1001
M any pat hological sit uat ions have been associa-t ed w iassocia-t h paassocia-t hological laughassocia-t er. Diffuse lesions such as produced by mult iple sclerosis and at herosclerosis are associat ed w it h int errupt ion of large descending t ract s. Various t umors, infarct s and degenerat ive le-sions have been associat ed w it h pat hological laugh-t er secondary laugh-t o larger focal lesions in any of laugh-t he ment ioned st ruct ures. Nevert heless, no previous re-port had linked t rigeminal neurinoma t o pat hologi-cal laught er as a sympt om, as in t he case w e report .
CASE
A 47-year-old w oman w as referred from a psychiat rist w it h a long hist ory of anxiet y and paranoid sympt oms. She had a more recent hist ory of headache and facial pain. The pain w as charact erized by shocks on her right facial side, w hich w ere frequent and w ould not improve w ith com-mon analgesics. On further questioning she complained of purposeless laughter, w hich w ould occur randomly, w ithout any motivation at any situation. There w as no sense of mirth preceding laughter and the patient could not give any expla-nation to the bursts. There w as no association to anxiety preceding laughter, w hich occurred spontaneously during rest as w ell. During the first and subsequent consultations, laughter w as observed either w hen the patient w as reporting her illness or sometimes w hile she aw aited (Fig 1). On neu-rological examination she seemed orientated and no neuro-psychological alterations could be detected. Although she pointed the pain to occur in the territory of all the three branches of trigeminal nerve, hypoesthesia w as found only in V2 and V3. A right VI nerve palsy w as detected as w ell as a vestibular syndrome characterized by disturbance in gait and balance tow ards the right side.
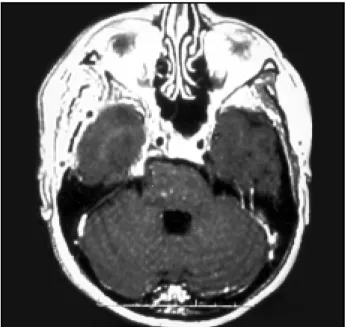
She w as submitted to a M RI (Fig 2) w hich reveled a le-sion w ith cystic characteristics in the middle fossa, causing brain stem compression. There w as no signal alteration in the brain stem w hich w ould suggest anatomical lesion.
She w as submitted to a frontoorbitozygomatic cranio-tomy, w ith a pretemporal extension. An extradural and in-tradural approach w as performed, allow ing identification of a tumor of the trigeminal nerve. Complete resection of the lesion w as achieved, as confirmed by M RI (Fig 3) and the pathological examination concluded it w as a neurinoma. The patient developed a w orsening of the VI nerve palsy and started to receive 200 mg of carbamazepine daily. She w as released from the hospital on the 10th post operative
day, presenting significant improvement of the vestibular symptoms. At one year after the operation she had no more trigeminal pain. Purposeless laughter had resumed as w ell.
DISCUSSION
In underst anding t he nosology of pat hological laught er one must first consider it s definit ion. As a w ider one, it is safer t o consider as pat hological any product ion of laught er w it hout t he appropriat e st i-mulus, eit her ext ernal (humorous) or int ernal (t hou-ght s), at inappropriat e sit uat ions and w it hout volun-t ary convolun-t rol1,2. Different iat ion must be made from em ot ional liabilit y or em ot ional incont inence, in w hich laught er and crying alt ernat e as an expression of the patient’s true (and pathological) affective state. Dementia may also be associated w ith inappropriate laughter w hich is usually not included in the series reporting pathological laughter, since it is believed to occur from the diffuse loss of higher function control over t he subcort ical circuit ry responsible f or t he expression of emotion and laughter. Finally, patho-logical laughter is associated w ith a structural lesions or functional disorders of the central nervous system.
Propedeut ically, it is import ant t o obt ain from t he pat ient if t here is a sense of mirt h preceding laught er or if it comes merely as a mot or phenomenon2,3. Pa-t ienPa-t s sensing mirPa-t h probably presenPa-t w iPa-t h a lesion af f ect ing higher levels of f unct ion, including t he circuit of Papez. Wit hout appropriat e st imulus, spon-t aneous mirspon-t h may occur from direcspon-t sspon-t imulaspon-t ion of subcort ical st ruct ures such as t he hypot halamus or t he hippoccampus and dent eat e girus, allow ing t he pat ient t o have a sensat ion compat ible t o t he facial an d resp irat o ry resp o n ses u n leash ed3. Co n co -mit ant ly, t he mot or response observed is far more realist ic (as a t rue laught er) t han in cases present ing pure mot or responses, w it hout t he sense of mirt h.
Low er lesions observed bot h in pat ient s and in experim ent al m odels produce m ovem ent s of t he facial muscles coordinat ed w it h respirat ory move-ment s t hat only resemble laught er, including t he sound produced. The facial expression may not be coherent w it h movement s of t he mout h and sounds from respirat ory movement s4,5.
1002 Arq Neuropsiquiat r 2002;60(4)
The pathological substrates for focal lesions asso-ciated w ith pathological laughter in the literature in-clude frontal (midline) and temporal gliomas1,3; free edge tentorial meningiomas compressing the hypo-thalamus, thalamus and cerebral peduncles1; other ten-torial edge tumors6, clival chordoma and pet roclival meningioma w ith marked compression of the pons and mesencephalon7,8; infarct s at t he diencephalic structures; multiple cerebrovascular lesions from em-bolic disease and demyelinating lesions affecting the central w hite matter and diencephalon. Removal of such lesions have been reported to resume
patholo-gical laughter1. Several epileptic disorders have been implicated w ith pathological laughter as w ell, w hich can be summarized as patients w ith complex partial seizures of suspected temporal origin and patients w ith hypothalamic hamartomas and gelastic seizures9.
We present ed a case of pat hological laught er in a pat ient w it h a large t rigeminal t umor. Besides non mot ivat ed laught er, t he pat ient also present ed sings of cerebelopont ine angle compression. There w as no sense of mirt h suggest ing not a disorder of higher neurological st ruct ures but a direct lesion on mot or effect ors of laught er. There w as no sign of hypoc-campal compression, w hile t he mass effect w as ma-inly upon t he brain st em. Compression at t his sit e w ould explain w hy laught er w as not comprehensible even t o t he pat ient as w ell as w hy it seemed not convincing t o t he examiner. The case illust rat es t hat the mass effect relief in this topography may improve t he pat ient ’s sympt oms of pat hological laught er.
REFERENCES
1. Davidson C, Kelman H: Pathological laughing and crying. Arch Neurol and psychiat 1939;42:595-643.
2. Ironside R. Disorders of laughter due to brain lesions. Brain 1956;79:589-609. 3. A rroyo S, Lesser R, Gordon B, et al. Mirth, laughter and gelastic
seazures. Brain 1993;116:757-780.
4. Cantu RC, Drew JH. Pathological laughter and crying associated with a tumor ventral to the pons. J Neurosurg 1966;24:1024-1026. 5. Stern WE, Brown WJ. Pathological laughter. J Neurosurg 1957;14:129-139. 6. Monteil P, Cohadon F. Pathological laughing as a symptom of tentorial
edge tumor. J Neurol, Neurosurg Psychiatry 1996;60:370.
7. Matsuoka S, Yokota A, Yasukoushi H, et al. Clival cordoma associated with pathological laughter. J Neurosurg 1993;79:428-433.
8. Shafqat S, Elkind MSV, Chio cca EA , Takeo ka M, Ko ro shetz WJ. Petro clival meningeo ma presenting w ith patho lo gical laughter. Neurology 1998;50:1918-1919.
9. Loiseau P, Cohadon F. Gelastic epilepsy, a review of five cases. Epilep-sia 1971;12:313-323.
Fig 2. A: T1-w eighed M R image show ing a large lesion w it h hyposignal cont ent and no cont rast enhancement . B: At T2-w eighed image, t he hypersignal core suggest s t he cont ent t o be cyst ic.