www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Does
stapes
surgery
improve
tinnitus
in
patients
with
otosclerosis?
夽
Onur
Ismi
a,∗,
Osman
Erdogan
a,
Mesut
Yesilova
a,
Cengiz
Ozcan
a,
Didem
Ovla
b,
Kemal
Gorur
aaUniversityofMersin,FacultyofMedicine,DepartmentofOtorhinolaryngology,Mersin,Turkey bUniversityofMersin,FacultyofMedicine,DepartmentofBiostatistics,Mersin,Turkey
Received23May2016;accepted11July2016 Availableonline2August2016
KEYWORDS
Otosclerosis; Tinnitus; Stapedotomy; Lowpitch; Highpitch
Abstract
Introduction:Otosclerosis(OS)istheprimarydiseaseofthehumantemporalbone character-izedbyconductivehearinglossandtinnitus.Theexactpathogenesisoftinnitusinotosclerosis patientsisnotknownandfactorsaffectingthetinnitusoutcome inotosclerosispatientsare stillcontroversial.
Objectives:Tofindtheeffectofstapedotomyontinnitusforotosclerosispatients.
Methods:Fifty-sixotosclerosispatientswithpreoperativetinnituswereenrolledtothestudy. PuretoneaverageAir-BoneGapvalues,preoperativetinnituspitch,Air-BoneGapclosureat tinnitusfrequencieswereevaluatedfortheireffectonthepostoperativeoutcome.
Results:Low pitch tinnitus had more favorable outcome compared to high pitch tinnitus (p=0.002).PostoperativeaveragepuretonethresholdsAir-BoneGapvalueswerenotrelatedto thepostoperativetinnitus(p=0.213).Therewasnostatisticallysignificantdifferencebetween postoperativeAir-BoneGapclosureattinnitusfrequencyandimprovementofhighpitchtinnitus (p=0.427).TherewasastatisticallysignificantdifferencebetweenAir-BoneGapimprovement intinnitusfrequencyandlowpitchtinnitusrecovery(p=0.026).
Conclusion:Lowpitch tinnitusis morelikelyto beresolvedafter stapedotomy for patients withotosclerosis.HighpitchtinnitusmaynotresolveevenafterclosureoftheAir-BoneGapat tinnitusfrequencies.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:IsmiO,ErdoganO,YesilovaM,OzcanC,OvlaD,GorurK.Doesstapessurgeryimprovetinnitusinpatientswith
otosclerosis?BrazJOtorhinolaryngol.2017;83:568---73.
∗Correspondingauthor.
E-mail:[email protected](O.Ismi).
http://dx.doi.org/10.1016/j.bjorl.2016.07.001
1808-8694/©2016Associac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.PublishedbyElsevierEditoraLtda.Thisisanopen
PALAVRASCHAVE
Otosclerose; Zumbido; Estapedotomia; Grave;
Agudo
Aestapedotomiamelhoraozumbidoempacientescomotosclerose?
Resumo
Introduc¸ão: Otosclerose(OS)éaprincipaldoenc¸adoossotemporalhumanocaracterizadapor perdaauditivacondutivaezumbido.Apatogeniaexatadozumbidoempacientescom otoscle-rosenãoéconhecidaefatoresqueafetamodesfechodezumbidoempacientescomotosclerose aindasãocontroversos.
Objetivos: Encontraroefeitodaestapedotomiasobreozumbidoempacientescomotosclerose.
Método: Foramincluídosnoestudo56pacientescomotosclerosecomzumbidopré-operatório. Osvaloresmédiostonaisdogapaero-ósseo,otomdezumbidonopré-operatório,ofechamento dogapnasfrequênciasdoszumbidosforamavaliadosquantoaoseuefeitosobreodesfecho pós-operatório.
Resultados: Ozumbido em tom grave tevedesfecho maisfavorável em comparac¸ãocom o zumbidoagudo(p=0,002).Osvaloresmédiosdosgapspós-operatóriosnãoforamrelacionados comozumbidopós-operatório(p=0,213).Nãohouvediferenc¸aestatisticamentesignificativa entreofechamentopós-operatóriodogapnafrequênciadozumbidoemelhoradozumbidode tomagudo(p=0,427).Houvediferenc¸aestatisticamentesignificativaentreamelhoranogap nasfrequênciasdozumbidoerecuperac¸ãodozumbidodetommaisgrave(p=0,026).
Conclusão:Ozumbidodetommaisgraveparecesermelhorresolvidodepoisdeestapedotomia empacientescomotosclerose.Ozumbidodetomagudopodenãodesaparecer,mesmoapóso fechamentodogapnasfrequênciasdozumbido.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Otosclerosis(OS)istheprimarydiseaseofthehuman tem-poralbone.Itisanautosomal-dominanthereditarydisease withvariablepenetrance.Clinically,progressiveconductive hearinglossandtinnitusarethemainsymptoms.Themost common area for stapedial fixation is the anterior crura. Sensorineuralhearinglosscandevelopiftheplaquesinvolve thecochlea.1
Otosclerosis was described about two centuries ago; however, the exact pathogenesis is not fully understood. Although hearing AIDS and medical therapy have been recommendedin certainconditions,smallfenestra stape-dotomy still remains the main choice in patients with conductivetypehearingloss.1Thesuccessofstapessurgery inpatientswithOSisevaluatedwiththeresultsof postop-erativehearingandtherateofAir-BoneGapclosure.
Tinnitusisalsoacommonandunderestimatedsymptom beside conductive hearing loss in OS.2 Satisfaction rates afterstapessurgeryisdirectlyrelatedtothepostoperative tinnituscessation.OS patientswithunresolved tinnitusin the postoperative periodreported significantly lower sat-isfactionscoresfromsurgery.3 Theestimated incidenceof subjectivetinnitusinOSpatientsis56---84.5%.2,4
The exact pathogenesisof tinnitusin OSis notknown. Several authors have reported different possible mecha-nisms as follows: reduction of inner ear fluid vibration, unmaskedmuscularorvascularnoiseswithconductive hear-ing loss, intravascular agglutination of red blood cells in thevesselsofthe cochlea,toxicmetabolites producedby the otosclerotic foci, pathological vascularization of the
otoscleroticboneandirritationofthenervefibers by oto-scleroticbone.4,5
Althoughtherehavebeenseveralpublishedstudies,the effect of stapes surgery on tinnitus is still a subject of debate.Someauthorsreportedthatpreoperativelowpitch tinnitusis morelikelytoberesolvedby stapessurgery,5,6 whereasGersdorffetal.7andAyacheetal.8foundno sta-tistical significance between low and high pitch tinnitus recovery.Apartfromtinnitusfrequency,preoperative non-compensated tinnitus9 and postoperative high frequency hearingloss3wereclaimedtohaveanunfavorableoutcome. Furthermore,theeffectof Air-Bone Gap(ABG)closure at tinnitusfrequenciesonthepostoperativetinnitusoutcome hasnotbeendiscussedinanyofthestudies.
Different from other studies, in this manuscript, we evaluated the effect of Air-Bone Gap closure at tinnitus frequenciesonthelow,middleandhighpitchtinnitusstatus.
Methods
OSwasconfirmedduringsurgery.Allofthepatients under-went smallfenestra stapedotomy and hearing restoration withTeflonpistonbysinglesurgeon.Patientshavingother possibleetiologyfortinnitussuchasacoustictrauma,blood biochemistryabnormalities includinganemia, vitamin B12 deficiency,thyroidfunctiontestabnormalities,andprevious earsurgeryhistorywereexcludedfromthestudy.
Surgicaltechnique
All patients were operated under the general anesthe-sia with endaural incision. Briefly; after modified Rosen incision, tympanomeatal flap elevation and chordal bony removalwithacuretteordrill,mobility ofossicularchain wasinspected andpalpatedtoestablish thediagnosis.All patientswereoperatedusingFisch’sreversalsteps stapedo-tomytechnique.10 Thedistancebetweenlateralsurfaceof theincuslong processandstapesfootplatewasmeasured witha malleable measuring rod. Smallfenestra was per-formedwith0.5or0.7mmdrills.Meticulouscarewastaken topreventtheaspirationofthefenestraandplacementof theprosthesisimmediatelyafterformingthefenestra.Small fenestrawasnotsealedbeforeplacementoftheprosthesis. Themobilityofprosthesisisassessedbygentlepalpationof malleus.
Patientcharacteristicsandplanning
Therewere42(60.8%)femalesand27(39.1%)males.Mean agewas42years(range32---57years).56(81.1%)patients hadpreoperativetinnituscomplaint.Thepreoperative tinn-itus frequency wasmeasured by the pitch-matching test, wascalibratedasfollow:Highfrequencies(4kHz,6kHz,and 8kHz),middlefrequencies(1kHz,2kHz,and3kHz)andlow frequencies(125Hz,250Hz,and500Hz).11Forpitch-match testingtheadaptive(bracketing)methodwasused.Briefly, thetonewassetsuccessivelyto9audiometricfrequencies between0.125 and 8kHz (0.125,0.25, 0.5, 1,2, 3, 4,6, and8kHz),andthesubjectwasaskedtoindicatewhichof thesefrequencies mostclosely matchedthepitchoftheir tinnitus.Thefrequencyofthetesttonewasthenadjustedin half-octavestepsaboveandbelowtheselectedfrequency, andthesubjectwasaskedtoindicatewhichofthe frequen-ciesbestmatched thetinnituspitch.The finalmatchwas takenasthe frequency that thesubjectjudged to match mostcloselytheirtinnitus.Thistechniqueisrecommended forroutineclinicaluseandseemstoproducefeweroctave errorsthanotherprocedures.12,13
These patients were divided in four groups regarding their postoperative tinnitus status. Group I, completely recovered;GroupII,Improved;GroupIII,Unchanged;Group IV,Worsened.GroupIandIIwereclassifiedinthesamegroup as‘‘favorable’’ outcome. Preoperative and postoperative first year pure tone air and bone conduction thresholds, Air-Bone Gaprates wereassessed according tothe Amer-ican Academy of Otolaryngology Head and Neck Surgery Guidelines.14Air-BoneGapwascalculatedwithsubtraction of the bone conduction threshold levelsfrom air conduc-tionthresholdlevels.Successofthesurgerywasdefinedas postoperativefirstyearpuretoneABG<10dBwithout sen-sorineuralhearingloss(postoperative>10dBdeterioration
ofboneconductionlevelscomparedtopreoperativelevels forfrequencies1.2and4kHz).8
Statisticalanalysis
Descriptivestatisticswerepresentedasproportionsor medi-ans(25---75%percentiles)asappropriate.
All continuous measurements were tested for normal-ity using the Kolmogorov---Smirnov and Shapiro---Wilktest.
p<0.05 wasaccepted assignificant.As measurementsdid not displaya normal distribution,non-parametric method Mann---Whitney U-test was used for independent groups’ comparison.Thecomparisonresultsweredisplayedwiththe box-plotgraph.
Categorical data were compared using pearson Chi-SquarewithYates’s correction,likelihoodratioor Fisher’s exacttest.TwoproportionZtestwasusedtocomparethe two groups whether any differences between them were significant.
Results
Fifty-six (81.1%) of 69 patients had preoperative tinni-tus complaint. The overall success rate was 79.7% (55 of 69 patients). There was no worsened tinnitus among patientswithpreoperativetinnitus.Howeverinonepatient withoutpreoperativetinnitus,moderate(60dB) sensorineu-ral hearingloss occurred. He reported tinnitus complaint postoperatively.Preoperativetinnitusfrequencies wereas follows:20 patients withlow pitchtinnitus,four patients withmiddlepitchand32patientswithhighpitchtinnitus.
Thirty-fourof 56(60.7%) patients hada favorable out-come with Group I (28 patients---50%) or Group II (6 patients---10.7%) tinnitus status. Twenty-two of 56 (39.3%) patientshadunchanged(GroupIII)tinnitusstatus.
PostoperativeABGwassmallerthan10dBin44(78.6%) of56patientswithpreoperativetinnitus.ABGwasbetween 10and20dBin9(16%)andgreater than21dBin 3(5.4%) patients. None of these patients had postoperative sen-sorineural hearing loss. Preoperative and postoperative frequency specific ABG values were given in Table 1. Relationship between postoperative tinnitus status and postoperative average pure tone threshold ABG levels wereshowninFig.1.Therewasnostatisticallysignificant
Table1 Meanfrequencyspecificpreoperativeand
postop-erativeAir-BoneGap(ABG)values.
Frequency(kHz) MeanABG SD p-Values 0.5Preop 46.73 10.79 <0.001
0.5Postop 8.84 7.31
1Preop 41.92 10.48 <0.001
1Postop 9.03 7.98
2Preop 35.96 9.7 <0.001
2Postop 7.4 6.52
3Preop 35.57 9.73 <0.001
3Postop 8.17 6.26
30
25
20
15
10
5
0
Completely recovered or improved
Unchanged
Post operative tinnitus status
P
o
st oper
ativ
e ABG
Figure 1 Comparison of postoperative tinnitus status and
postoperativeaveragepuretonethresholdABGlevelshasbeen demonstrated(ABG,Air-BoneGap).
difference between postoperative average pure tone
thresholdsABGlevelsandtinnitusstatus(p=0.213). Preoperativetinnitusfrequency andpostoperative tinn-itus status was demonstrated in Table 2. There was a statistically significant relationship between preoperative tinnitusfrequencyandpostoperativetinnitusimprovement (p=0.003), low pitch tinnitus had a more favorable out-comecomparedtohighpitchtinnitus(p=0.002).Therewas nostatisticallysignificantdifferencebetweenlowand mid-dle(p=0.22),orhigh andmiddlepitchtinnitus(p=0.812) regardingpostoperativetinnitusimprovement.
Thirty-two patients with preoperative high frequency tinnituswereevaluatedforABGclosurerateattinnitus fre-quencies postoperatively. Postoperative tinnitus status of thesepatientswasgiveninFig.2.Therewasnostatistically significant difference between postoperative ABG closure attinnitusfrequenciesandimprovementofhighfrequency tinnituscomplaints(p=0.427).
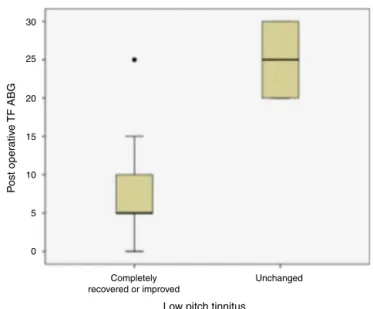
Twentypatientswithpreoperativelow frequency tinni-tuswere assessedregarding theirclosure ofAir-Bone Gap attinnitusfrequencyandpostoperativetinnituscomplaints (Fig. 3). There was a statistically significant difference betweenABGimprovementattinnitusfrequenciesand tinn-itusrecovery(p=0.026).
Table2 Relationshipbetweentinnitusfrequencyand
post-operativetinnitusstatus.
Tinnitus
Subjective tinnitus frequency
Improvedor completely recovered
Unchanged p-Value
Highfrequency 14(43.8%) 18(56.2%) 0.003 Middlefrequency 2(50%) 2(50%)
Lowfrequency 18(90%) 2(10%)
25
20
15
10
5
0
Completely recovered or improved
Unchanged
High pitch tinnitus
P
o
st oper
ativ
e
TF ABG
Figure2 Comparisonofhighpitchtinnitusstatusand
postop-erativeABGvaluesattinnitusfrequencieswasshown(TFABG, TinnitusFrequencyAir-BoneGapvalues).
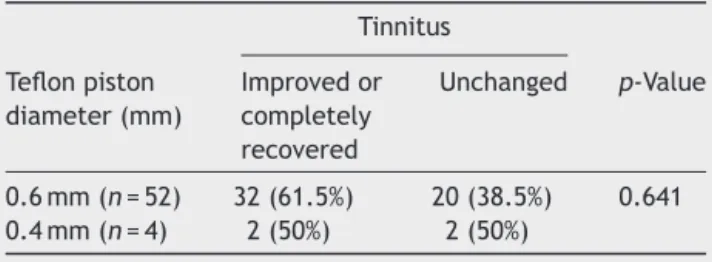
Twosizesofprosthesiswereused:0.4mmshaftdiameter forfourof thepatients and0.6mm for52 ofthem. Com-parisonofTeflonpistondiameterandpostoperativetinnitus statuswas summarized in Table 3. There wasno statisti-cally significant relationship between prosthesis diameter andpostoperativetinnitusstatus(p=0.641).
Discussion
Inthe current study,preoperative tinnitus waspresent in 81.1%of patientswithOS; theoverall success rateofour stapedotomy surgery was 78.6% for these patients. The tinnitusincidencewasreportedas56---84.5%2,4andthe suc-cessrateof thesurgery wasshownas56---92% in previous studies.4,6,8,15
30
25
20
15
10
5
0
Completely recovered or improved
Unchanged
Low pitch tinnitus
P
o
st oper
ativ
e
TF ABG
Table3 RelationshipbetweenTeflonpistondiameterand tinnitusstatus.
Tinnitus
Teflonpiston diameter(mm)
Improvedor completely recovered
Unchanged p-Value
0.6mm(n=52) 32(61.5%) 20(38.5%) 0.641 0.4mm(n=4) 2(50%) 2(50%)
Thirty-four (60.7%) patients with tinnitus completely recovered or improved; however, tinnitus was unchanged in 22 (39.3%) patients in our study. The tinnitus had not worsened in any patients postoperatively. The favor-able (completely recovered or improved) tinnitus rate has been reported as 40---96% postoperatively in previous manuscripts.9,15LimaAdaetal.15andSzyma´nskietal.4also reportedthatnopatientshadworsenedtinnitus postopera-tively.
In our study, improvement of tinnitus was more pro-nounced in preoperative low pitch tinnitus compared to the high pitch ones after stapes surgery (p=0.002). The exact pathophysiology of tinnitus is unknown in patients withOS. The efferentauditory pathwayhasa modulatory effect on the outer hair cells of the Corti organ, which canbufferoramplifythemessagecomingfromthebrain.5 Whentheauditorystimulusdecreases,thecentralnervous system compensates by increasing the sensitivity of the outer hair cells16 and generates a phantom auditory per-ception as tinnitus. Helleret al.17 and DelBo L. et al.18 showedthat healthy adults withnormal hearing reported tinnitus generation after staying in an anechoic chamber foralong time.The decreaseintheinner earfluid vibra-tioninpatientswithconductivehearingloss,suchasthatin OS,diminishestheafferentstimulusofthecentralauditory pathway.Thedecreasedafferentstimulusinturndecreases the suppressive effect of the efferent pathways on the Corti’s organ.Efferent pathway dysfunctionis one of the possiblemechanismsoftinnitusperceptioninpatientswith conductivehearing loss.5,16 Causse etal.5 stated thatthe signal amplification mechanism of outer hair cells causes a low pitch tinnitus rather than a buzzing or engine-like noiseincaseswithconductivehearingloss.Whenthe vibra-tions of the inner ear fluids are re-established surgically and the hearing loss is improved, the low pitch tinnitus mostly recovers. Our findings and those of several previ-ousstudies6,19,20 alsosupportthisidea.However,Gersdorff et al.7 and Ayache et al.8 could not find any correlation between thepostoperative tinnitusstatus and the preop-erativetinnitusfrequency.
Although we had a successful hearing outcome, post-operative tinnitus recovery was not related to the postoperativeABGclosure(p=0.213).Thisfindingwas sup-portedbyRamsayetal.,6LimaAdaetal.,15Szyma´nskietal.4 and Gersdorff et al.7 They found no correlation between surgical success and postoperative tinnitus status, either. Recently,Bast etal.9 claimedthat thesuccess of surgery had an impact on the preoperative compensated tinni-tus,whereasthenon-compensatedtinnitusdidnotresolve
despite a successful surgery. The results of Glasgold and Altmann21andSparanoetal.22didnotsupportourfindings, andapoorerpostoperativehearingstatuswasmorelikely tohaveanunfavorabletinnitusoutcomeintheirstudies.
Tinnitusaccompanies70---85%ofcaseswithhearingloss caused by different pathologies of the auditory system.23 The pitch of tinnitus often correlates the hearing loss frequencies.24Alossoradecreaseincochlearinputscauses are-organizationandover-signalingofthehearingloss fre-quenciesinthecentralpathways.Forthisreason,thepitch of thetinnitusis perceived closetoorwithin thehearing lossfrequencies.25 Fromthispointofview,weassessedthe effectofABGclosureattinnitusfrequenciesonthetinnitus outcome in OSpatients. Wefound that whenthe tinnitus pitchslidtolowerfrequencies,ABGclosureattinnitus fre-quencyincreasedthechanceoftinnitusimprovement.This findingshowsthatthepathogenesisofhighfrequency tinni-tusinOSpatientsisadifferentfactorratherthanthefixed stapesfootplate.
ThesurgicaltechniqueusedduringOSsurgeryismostly acceptedtohaveanimpactonthetinnitusoutcome.Sakai etal.19showedthatamoretraumaticsurgerysuchastotal stapedectomy had an unfavorable tinnitus outcome com-paredtopartialstapedectomyorstapedotomy.Inthestudy ofGersdorffetal.,7theprognosisoftinnituswasbetterafter stapedotomycomparedtopartialstapedectomy,andtheuse ofargonlaserduringsurgerydidnotchange theoutcome. Ayache etal.8 opposedthisfinding; theyfound no differ-encebetweenthesurgicaltechniquesandthepostoperative tinnitusoutcome.Recently,Bagger-Sjöbäcketal.3reported thatOSsurgerycausedhighfrequencyhearinglossbeyond 8kHzandthatthetinnitusoutcomewasdirectlyrelatedto this surgical trauma-induced high frequency hearing loss. However,thefindingsofRamsayetal.6didnotsupportthis report,andforpatientswithhighfrequencyhearinglossin thepostoperativeperiodduetosurgicaltrauma,the tinni-tusoutcomewasnotdifferentcomparedtotherestofthe patients.Accordingtoourresults,asmallerperforationin theovalwindowandthe useofasmaller diameterTeflon pistondidnot changethe tinnitusoutcome,but this find-ingmaybespuriousduetothelownumberofpatientswith prosthesisof0.4mmdiameterinourseries.
Conclusion
Stapessurgerynotonlyre-establishesthehearingofpatients with OS, but also resolvesthe tinnitus complaint in most ofthepatients.Thecomplaintoflowfrequencytinnitusis morelikelytoberesolvedaftersurgery.Highpitchtinnitus maynot resolveevenafter closureof theABGat tinnitus frequencies.Allotosclerosispatientswiththecomplaintof tinnitusmustbeevaluatedfortheirtinnitusfrequencies pre-operatively.Thepatientswithhighfrequencytinnitusmust beinformedthattheirtinnituscomplaint maynotresolve despiteasuccessfulimprovementinhearing.
Conflicts
of
interest
References
1.HouseJW,CunninghamCD.Otosclerosis.In:FlintPW,Haughey BH,LundVJ,NiparkoJK,Richardson MA,RobbinsKT, etal., editors.Cummingsotolaryngologyheadandnecksurgery.5th ed.Philadelphia,PA:Mosby-Elsevier;2010.p.2028---35.
2.GristwoodRE,VenablesWN.Otosclerosisandchronictinnitus. AnnOtolRhinolLaryngol.2003;112:398---403.
3.Bagger-Sjöbäck D, Strömbäck K, Hultcrantz M, Papatziamos G,SmedsH,Danckwardt-LillieströmN,et al.High-frequency hearing,tinnitus,andpatientsatisfactionwithstapedotomy:a randomizedprospectivestudy.SciRep.2015;5:13341.
4.Szyma´nskiM,GołabekW,MillsR. Effectofstapedectomy on subjectivetinnitus.JLaryngolOtol.2003;117:261---4.
5.CausseJB,VincentR.Poorvibrationofinnerearfluidsasacause oflowtonetinnitus.AmJOtol.1995;16:701---2.
6.RamsayH,KärkkäinenJ, PalvaT.Success insurgeryfor oto-sclerosis: hearing improvement and other indications. Am J Otolaryngol.1997;18:23---8.
7.GersdorffM,NouwenJ,GilainC,DecatM,BetschC.Tinnitus andotosclerosis.EurArchOtorhinolaryngol.2000;257:314---6.
8.AyacheD,EarallyF,ElbazP.Characteristicsandpostoperative courseoftinnitusinotosclerosis.OtolNeurotol.2003;24:48---51.
9.BastF,MazurekB, SchromT. Effect ofstapedotomy on pre-operativetinnitusandits psychosomaticburden.AurisNasus Larynx.2013;40:530---3.
10.Fisch U. Stapes surgery. In: Fish U, May J, editors. Tym-panoplasty,mastoidectomyandstapessurgery.NewYork,PA: ThiemeMedicalPublishers;1994.p.211---34.
11.MartinesF,BentivegnaD,MartinesE,SciaccaV,MartinciglioG. Characteristicsoftinnituswithorwithouthearingloss: clini-calobservationinSiciliantinnituspatients.AurisNasusLarynx. 2010;37:685---93.
12.KimTS,YooMH,LeeHS,YangCJ,Ahn JH,ChungJW,etal. Short-term changes in tinnitus pitch related to audiometric shapeinsuddensensorineuralhearingloss.AurisNasusLarynx. 2016;43:281---6.
13.TylerRS,Conrad-ArmesD.Tinnituspitch:acomparisonofthree measurementmethods.BrJAudiol.1983;17:101---7.
14.Committee On Hearing and Equilibrium guidelines for the evaluation of results of treatment of conductive hearing loss. American Academy of Otolaryngology-Head and Neck Surgery Foundation. Otolaryngol Head Neck Surg. 1995;113: 186---7.
15.LimaAdaS,Sanchez TG, MarcondesR, BentoRF.The effect ofstapedotomyontinnitusinpatientswithotospongiosis.Ear NoseThroatJ.2005;84:412---4.
16.LimaAdaS,SanchezTG,BonadiaMoraesMF,BatezatiAlvesSC, BentoRF.Theeffectoftympanoplastyontinnitusinpatients withconductive hearingloss: a six month follow-up. Braz J Otorhinolaryngol.2007;73:384---9.
17.HellerMF,BergmanM.Tinnitusauriuminnormallyhearing per-sons.AnnOtolRhinolLaryngol.1953;62:73---83.
18.DelBoL,FortiS,AmbrosettiU,CostanzoS,MauroD,UgazioG, etal.Tinnitusauriuminpersonswithnormalhearing:55years later.OtolaryngolHeadNeckSurg.2008;139:391---4.
19.SakaiM,SatoM,LidaM,OgataT,IshidaK.Theeffecton tinni-tusofstapessurgeryforotosclerosis.RevLaryngolOtolRhinol (Bord).1995;116:27---30.
20.Causse JB, Vincent R. Surgery and tinnitus for otosclerotic patients.IntTinnitusJ.1996;2:123---7.
21.GlasgoldA,AltmannF.Theeffectofstapessurgeryontinnitus inotosclerosis.Laryngoscope.1966;76:1524---32.
22.SparanoA,LeonettiJP,MarzoS,KimH. Effectsof stapedec-tomyontinnitusinpatientswithotosclerosis.IntTinnitusJ. 2004;10:73---7.
23.Manche SK, Madhavi J, Meganadh KR, Jyothy A.
Associa-tion of tinnitus and hearing loss in otological disorders: a
decade-longepidemiologicalstudyinaSouthIndianpopulation.
Braz J Otorhinolaryngol. 2016, http://dx.doi.org/10.1016/
j.bjorl.2015.11.007.
24.McNeillC,Távora-VieiraD,AlnafjanF,SearchfieldGD,Welch D.Tinnituspitch,maskingandtheeffectivenessofhearingaids fortinnitustherapy.IntJAudiol.2012;51:914---9.