www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Effectiveness
of
acupuncture
therapy
as
treatment
for
tinnitus:
a
randomized
controlled
trial
夽
Marcelo
Yugi
Doi
a,b,∗,
Simone
Sayomi
Tano
a,b,
Adriane
Rocha
Schultz
a,b,
Ricardo
Borges
c,d,
Luciana
Lozza
de
Moraes
Marchiori
a,baRehabilitationScienceProgramAssociate,UniversidadeEstadualdeLondrina(UEL),Londrina,PR,Brazil bUniversidadeNortedoParana(UNOPAR),Londrina,PR,Brazil
cFaculdadedeMedicina,UniversidadeEstadualdeLondrina(UEL),Londrina,PR,Brazil
dMedicalResidencyProgramSupervisorinOtolaryngology,HospitalUniversitáriodeLondrina(UEL),Londrina,PR,Brazil
Received31March2016;accepted13April2016 Availableonline30April2016
KEYWORDS
Acupuncturetherapy; Tinnitus;
Qualityoflife; Randomized controlledtrial; Rehabilitation
Abstract
Introduction:Tinnitusisasubjectivesensationofhearingasoundintheabsenceofanexternal stimulus,whichsignificantlyworsensthequalityoflifein15---25%ofaffectedindividuals.
Objective:Toassesstheeffectivenessofacupuncturetherapyfortinnitus.
Methods:Randomizedclinicaltrial(REBEC:2T9T7Q)with50participantswithtinnitus,divided intotwogroups:25participantsintheacupuncturegroupand25participantsinthecontrol group.Theacupuncturegroupreceivedacupuncturetreatmentandthecontrolgroupreceived notreatment.Afteraperiodof5weeks,theywerecalledtoperformthefinalevaluationand thecontrolgroupreceivedacupuncturetreatmentforethicalreasons.
Results:Astatisticallysignificantresultwasfoundfortheprimaryoutcome,reducingthe inten-sityoftinnitus,withp=0.0001andthesecondaryendpoint,showingimprovementinqualityof life,withp=0.0001.
Conclusion:Chinesescalpacupunctureassociated withbilateralelectroacupuncture demon-strated, in theshort term, astatistically significant improvementby reducingthe levelof tinnitusintensity,aswellasimprovingthequalityoflifeofindividualswithtinnitus.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽
Pleasecitethisarticleas:DoiMY,TanoSS,SchultzAR,BorgesR,MarchioriLLM.Effectivenessofacupuncturetherapyastreatmentfor tinnitus:arandomizedcontrolledtrial.BrazJOtorhinolaryngol.2016;82:458---65.
∗Correspondingauthor.
E-mail:[email protected](M.Y.Doi).
http://dx.doi.org/10.1016/j.bjorl.2016.04.002
PALAVRAS-CHAVE
Terapiapor acupuntura; Zumbido;
Qualidadedevida; Ensaioclínico controladoaleatório; Reabilitac¸ão
Efetividadedaterapiaporacupunturacomotratamentoparaozumbido:ensaio clínicoaleatorizado
Resumo
Introduc¸ão: Ozumbidoéasensac¸ãosubjetivadeouvirum somnaausênciadeum estímulo externoepiorasignificativamenteaqualidadedevidade15%---25%daspessoasafetadas.
Objetivo: Verificaraefetividadedaterapiaporacupunturaemindivíduoscomzumbido.
Método: Ensaioclínicoaleatorizadocom50participantescomzumbido,divididosemdois gru-pos:25participantesnoGrupodaAcupuntura(GA)e25participantesdoGrupodeControle (GC).OGArecebeutratamentocomacraniopunturachinêseoGCnãorecebeunenhum trata-mento.Apósoperíodode5semanas,elesforamchamadospararealizaraavaliac¸ãofinaleo GCrecebeutratamentodeacupunturaporquestõeséticasdepesquisa.
Resultados: Foiencontradoresultadoestatisticamentesignificativoparaodesfechoprimário, reduzindo aintensidadedozumbido,comp=0,0001eodesfechosecundário,apresentando melhoranaqualidadedevida,comp=0,0001.
Conclusão:A craniopuntura chinesaassociada à eletroacupuntura bilateral nos mostrou no curtoprazo,umamelhoraestatisticamentesignificativa,reduzindooníveldeintensidadedo zumbido,bemcomomelhorandoaqualidadedevidadosindivíduoscomzumbido.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Tinnitusis a symptom definedasthe perception of sound withoutthepresenceofanexternalsoundsource.1
Itisestimatedthatapproximately5---15%ofthe popula-tionhasofsometypeoftinnitusand,althoughitcanoccur atanyage,itismoreprevalentamongtheelderly(mainlyin thoseagedbetween60and69years)thaninyoungadults.2 Inastudyontheincidenceoftinnitus,Nondahletal.3 fol-loweda groupof 2922adult andelderlyindividuals, aged 48---92years,for10years.Duringthefirst5yearsof follow-upinthissamegroup,theyobservedthattheincidenceof tinnitusintheassessedpopulationwas5.7%.4After10years, theauthorsfoundthattheincidencehadmorethandoubled, reaching12.7%.3
In Brazil, it is estimated that 17% of the population is affectedbytinnitus,i.e.,morethan28millionBrazilians.5 Santosetal.6 evaluated406patients ina 6month period andfoundthat58%hadatinnituscomplaint;ofthese,68% werefemalesand32%males.Inastudycarriedoutby Gib-rinetal.7in2012,theauthorsevaluated519individualsof both genders witha median age of 69 years andfound a prevalenceof42.77%fortinnituscomplaints.
Itiscurrentlybelievedthattinnitusoccursasaresultof thedynamic interactionof severalcentersof thenervous andthelimbicsystem,andthatcochlearalterationsand/or lesions arethe precursorsof this process, causing imbal-anceinthelowerauditorypathways,resultinginabnormal neuronalactivity,furtherenhancedbythecentralnervous system,andfinallyperceivedastinnitus.8
Several etiologies have been proposed, including oto-logic, dental, neurological, psychiatric diseases, cervical spineandmetabolicdisorders,aswellasothersrelatedto theintakeofdrugs,caffeine,alcohol,andtobacco.9
However, the physiopathological mechanisms of tinn-itus are not well-defined, and therefore the treatment remains amajor challengetodate. Symptom subjectivity and the wide etiological variety, often seen in the same patient,makeitdifficulttoobtaingoodresults.9Moreover, currently, noone specific treatment, includingdrug ther-apy, is considered effective in treating the symptoms of tinnitus.10
Complementaryandalternativemedicinehasoftenbeen usedtotreattinnitus,andacupunctureis oneofthemost often-usedoptions.10 Acupunctureisatherapeuticmethod thatinvolvestheinsertionandmanipulationofneedlesinto the body. The treatment of tinnitus by acupuncture has beenwidelydescribedinbooks11,12;however,thescientific literaturestilllacksstudiessupportingitstherapeutic effec-tiveness. Studies have shown that stimulation performed withneedlespromotesintroductionofanelectricalcharge that triggers action potentials in order to rebalance the system.13,14
Chinesescalpacupuncture isa contemporary acupunc-turetechniquethathasonly40yearsofhistory.Itintegrates traditionalChineseinsertion methods withWestern medi-calknowledgeofthecerebralcortex,andhasbeenproven tobeaveryeffectivetechniquefor thetreatment of sev-eraldiseasesofthecentralnervoussystem,15aswellasfor alleviatingthesymptomsoftinnitus.9
Losses (n=3)
∗ 1 due to lack of
availability to come for the sessions; and
∗ 2 due to fear and
hyper sensitivity to acupuncture needles.
Assessed regarding eligibility
criteria (n=76)
Excluded (n=26)
∗ 20 were excluded due to light and/or mild degrees according to the THI questionnaire
∗ 3 reported transportation difficulties; and
Randomized (n=50)
Acupuncture group (n=25)
Assessed at the end of the treatment
(n=22)
Assessed after 5 weeks without treatment
(n=24) Control group
(n=25)
∗ 3 did not come on the day scheduled for assessment
Losses (n=1)
∗ 1 did not come at the reassessment date
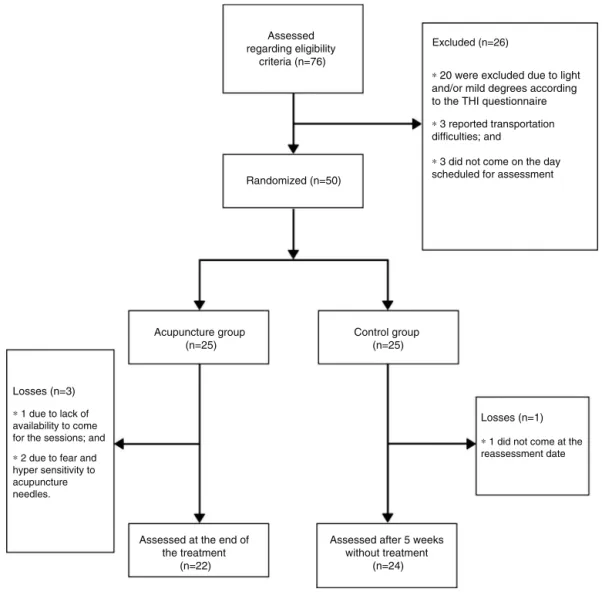
Figure1 Flowchart.
Hence,thisstudyaimedtodeterminetheeffectiveness ofan acupuncture program asatherapeutic procedure in patientswithtinnitus.
Methods
Thiswasarandomizedclinicaltrial(RCT)thatincluded indi-vidualsofbothgenders,agedbetween50and85years,with moderatecontinuoustinnitusfor at least1 year,in whom tinnitusinterferedwiththequalityoflifemeasuredbythe TinnitusHandicapInventory(THI)questionnaire.17
Exclusion criteriawere: individuals withactive cardio-vasculardisease,thoseusingpacemakersormetalimplants, andthosewhohadascoreattheTHIquestionnaireshowing onlyslightor milddegreesof interferencewithqualityof life.Inaddition,subjects whowere participatingin other treatmentprogramsfortinnituswereexcluded.
Allparticipants signed an informedconsent.The study wasapproved bythe EthicsCommitteeinResearch (num-ber95,055)andwasregisteredintheBrazilianclinicaltrial register(REBEC:2T9T7Q).
Thestudyparticipantswererecruitedthroughinterviews on the local television programs of three local stations,
whichintroducedtheresearchproject,informedthe popu-lationaboutthetinnitus,andprovidedrecommendationsto thoseinterestedinparticipatinginthestudy.Throughthese talk shows,76 phonecallswere receivedfromindividuals thatmetthestudycriteriaandwerecalledforevaluation.
Of these 76 assessed patients, 20 were excluded due to light and/or mild degrees according to the THI ques-tionnaire; 3reportedtransportation difficulties,and3did not appear for the evaluation appointment. Therefore, a total of 50 individuals of both genders, aged between 50 and85years,whowerenotundergoinganothertreatment fortinnitusandwhohadmoderatetoseverescoresatthe THIquestionnaire,asshownintheflowchart(Fig.1),were includedinthestudy.
The 50 participants were randomly divided into two groups.Randomizationwascarriedoutwiththeaidof com-puterizedtableofrandomnumberscreatedbyaMicrosoft Excelspreadsheet.
Mild
Moderate
Severe
Visual analog scale – VAS
Figure2 Visualanalogscale.
whoreceivednotreatment.Fig.1shows theflowchartof participants’enrollmentandrandomization.Afterthestart oftheinterventions, threeparticipantsfromtheAG with-drewfromthestudy,oneduetolackofavailabilitytoattend thesessionsandtwoduetofearandhypersensitivitytothe acupunctureneedles,thustotaling22individualsintheAG. OneparticipantfromtheCGalsowithdrewfromthestudy, afterfailingtoattendarevaluationconsultation.
Evaluations of AG participants were performed before andafter5weeksofintervention,by apreviouslytrained researcherwhowasblindedtotreatmentor controlgroup allocation.EvaluationsintheCGwereperformedat enroll-mentandaftera5weekintervalwithoutanytreatment,bya previouslytrainedresearcherwhowasblindedtotreatment orcontrolgroupallocation.
Acase historyformwascompletedtocharacterize the sample.Itcontainedinformationongender,age,presence or absenceof tinnitus,unilateral orbilateral tinnitus,the durationoftinnitusmanifestation,typeoftinnitus (contin-uousorintermittent),presenceorabsenceofdizziness,ear surgery,historyofexposuretooccupationalnoise,diabetes orhigh bloodpressure,pacemakeruse,metallicimplants, medicationsused,andwhetherthepatientwasundergoing orhadundergoneanykind oftreatment fortinnitusandif so,forhowlong,basedontheKatzprotocolforanamnesis.18 Hearing assessment was performed with an otoscopic evaluation of the external ear canal and tympanic mem-brane,andwithpuretoneaudiometry,consideredthegold standard to assess auditory threshold in adults.19 Hearing losswasclassifiedaccordingtoSilmanandSilverman20 and theclassificationofLloydandKaplanwasusedtogradethe degreeofhearingloss.21
Visualanalogscale(VAS)
Toassessthelevelofintensityofthetinnitus,avisualanalog scale(VAS)wasused(Fig.2),consistingofavisualgraphic tooltodeterminethevolumelevelorintensityordiscomfort caused bythetinnitus,ona scaleof 0---10.The patientis askedtogiveascorefrom0to10totheintensitygenerated bythetinnitus,where0representstotalabsenceoftinnitus symptomand10indicatesamaximumintensityoftinnitus symptom,requiringgoingtoahospitaltoreceivecare.14,22 TheVASwasappliedattheinitialandfinalassessments,both intheAGandtheCG.
THIquestionnaire
TheTHIisaquestionnairedevelopedbyNewmanetal.17in 1996,andconsistsof25questionswithascorerangingfrom0 to100,wherethehigherthescore,thegreatertheimpactof
tinnitusonpatientqualityoflife.Itisarapidmeasurement, easytoapplyandinterpret.Ithasbeenbroadlyusedinthe clinicalsettingtoassesspatientswithtinnitus.
The three main items assessed by the THI are: func-tionalreactionstotinnitus,suchasdifficultyconcentrating andantisocialtendencies;emotional reactionstotinnitus, suchasanger,frustration,irritability,depression;and cata-strophicreactionstotinnitus,suchasdespair,hopelessness, fearof severe disease, loss of control, and incapacity to cooperate.
THI iscurrently oneofthe mostaccepted methods for tinnitusassessment,havingbeenvalidatedinmany consen-suses.Itwastranslatedandculturally adaptedtobeused intheBrazilianpopulation in200523 anditsvalidationand reproducibilitywerecarriedoutin2006.24
Intervention
Theinterventionlasted5weeks,withatwice-a-week fre-quency, totaling ten sessions, with each session lasting approximately40min.The acupuncture programwas con-ducted by a specialist and supervised by the researcher. Participants were instructed to report any complaint, whetheror not associatedto the treatment. Both groups were instructed not to participate in any other tinnitus treatmentprogramthroughoutthestudyperiod.
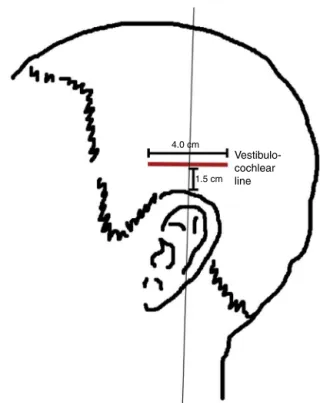
IntheAG,theparticipantsreceivedtreatmentthat fol-lowed an acupuncture program using the Chinese scalp acupuncturetechniqueassociatedwithelectrostimulation, bilaterallyin the vestibulocochlearline (Fig.3). This line is located 1.5cm abovethe ear apex in a horizontal line segmentcorrespondingto4cm.12
Inthecontrolgroup(CG),theparticipantsdidnotreceive acupuncturetreatment.Theseparticipantswereevaluated andthen waited 5weeks, afterbeing toldnot toreceive or undergo any treatment for tinnitus during this period, includingdrugtreatment,andtocontinuewiththeirnormal dailyactivities.Afterthe5weekperiod,theywerecalled intoundergothefinalevaluation.Itwasonlyafterthefinal assessment that these participants received acupuncture treatment,forethicalreasons.Theacupuncturetreatment programwasthesametowhichtheAGwassubmitted.
Statisticalanalysis
4.0 cm
1.5 cm
Vestibulo-cochlear line
Figure3 Vestibulocochlear lineaccording to Chinesescalp acupuncture.
TheMann---WhitneyUtestwasusedtocomparebetween thegroups,andtheWilcoxontestwasusedtoassesswithin eachgroup.
Allanalyseswereperformed byintentiontotreat using theSPSSv.15.0softwareandstatisticalsignificancewasset at5%(p≤0.05).
Results
Seventy-sixsubjectswereevaluatedregardingthestudy eli-gibilitycriteria.Ofthese,26(34.2%)wereexcludedand50 (65.8%)participatedinthestudy.Only46participants(92%) completedthetreatment.Descriptivecharacteristicsofthe sampleareshowninTable1.
Ofthe46participants,22wereallocatedtotheAGand ofthese,8weremalesand14females,withamedianage of62 years;17 hadbilateral sensorineuralhearing loss,3 hadunilateralsensorineuralhearingloss,and2didnothave hearingloss.Twenty-fourparticipantswereallocatedtothe CG,ofwhich10weremalesand13females,withamedian geof60years;18hadbilateralsensorineuralhearingloss,2 hadunilateralsensorineuralhearingloss,and4didnothave hearingloss.
Of the 90 ears assessed, the vast majority, 74 (82.2%) showedsensorineuralhearingloss;ofthese,31(34.4%)had normal degree, with a decrease in acute frequencies, 23 (25.5%)weremild,16(17.7%)weremoderate,4(4.4%)were severe,andnonewereprofound.
Concerningtheprimaryoutcome,intensitylevelof tinni-tusmeasuredbytheVAS,therewasastatisticallysignificant difference,p=0.0001 (Table2),whencomparingbetween the AG assessment at baseline and after treatment. The data showeda reductionof almost 50% in tinnitus
inten-sitywhencomparingAGandCGfrombaselinetotreatment withacupuncture.
There was no statistically significant difference when comparingtheresultsfromthedataevaluatedatbaseline andafter5weeksintheCG,withp=0.168(Table2).
Toassesstheresultsofthesecondaryoutcome (improve-mentinqualityoflifeasmeasuredbytheTHIquestionnaire) theTHI scores atbaseline,were comparedwithTHI after treatment in the AG,and astatistically significant differ-encewasobserved (p=0.0001; Table2), withthe median datarevealingadecreasefromgrade4(severeinterference inthequalityoflife)tograde2(mildinterferencein qual-ityoflife)oftinnitusinfluenceonqualityoflife,whereas intheCG,therewasnostatisticallysignificantdifference, withp=0.943(Table2).
When comparing the AG and CG regarding the values of the initial VAS scores and the initial THI question-naire, obtainedin the assessment beforethe start of the treatment,theresultsshowednostatisticallysignificant dif-ference,withp=0.580andp=0.331,respectively.However, whencomparingtheAGandCGregardingthevaluesoffinal THIandfinalVASobtainedafterthetreatment,theresults showed to be statistically significant, with p=0.0001 and
p=0.0001,respectively(Table2).
Discussion
ThetreatmentoftinnituswithAChasbeenwidelydescribed inTCM.The scientificliterature,however,lacksstudiesto demonstrateitseffectivenessasatreatmentoption.ACisa holisticformoftreatmenttailoredtoeachindividual.Thus, protocols withadequate standardized methods that meet the principles of TCM and modern Western medicine are difficulttocreate.9
This study aimed to compare the effectiveness of an acupuncture program for the treatment of patients with tinnitus.Theresultsindicatethattreatmentwith acupunc-ture improves the perception of tinnitus, decreases the intensity level, and improves the quality of life of indi-viduals with tinnitus. That differs from most literature results,25,26inwhichthestudiesreportednosignificant dif-ferencebetweentreatmentwithacupunctureandplacebo. Only a few studies reported a significant effect of acupuncturefor thetreatmentoftinnitus;however,these effectsweresignificantonlyforimmediaterelief.9
Onefactor thatcanexplainthisdifferenceisthe num-beroftreatmentsessionsperformedinthesestudies.Most of them had a treatment program with fewer than tem acupuncturesessions,andtwoofthesestudiesuseda sin-glesession, whichmaybeinsufficienttoobtain apositive clinicaloutcome.9,25---27
Another bias inherent to these studies was evaluated basedonthedescription oftheparticipantrandomization methods. Mostof the included studies had a high risk of bias.Low-qualitytrialsaremorelikelytooverestimatethe effect size. Moreover, none of the studies used a statis-tical calculation indicating the power of study sizes, and samples were obtained by convenience, and thus were nonrepresentative.28,29
Table1 Characteristicsoftheparticipantsassessedbeforetreatment.
Groups
AG(n=22) p CG(n=23) p
Gender,n(%)
Male 8(36.3) 10(43.4)
Female 14(63.7) 13(56.6)
Age(years) 62[57---67.5] 60[54.5---62]
Hearing(n;%)
Bilateralloss 17(77.3) 18(78.3)
Unilateralloss 3(13.7) 2(4.3)
Noloss 2(9) 4(17.4)
HLGrade(n) RE/LE RE/LE
NLwithdecrease 7/6 9/9
Mild 7/6 4/5
Moderate 2/5 5/4
Severe 1/2 1/1
InitialVAS 8[7---9] 0.331 8[7.5---9.5] 0.331
InicialTHI 56[44---65.5] 0.176 58[48---76] 0.176
M,male;F,female;HL, hearingloss;NL, normal;RE,rightear;LE,left ear;valuesshownasmedian [1stquartile;3rdquartile]; Mann---WhitneyUtestconsideringp>0.05;AG,acupuncturegroup;CG,controlgroup;InitialVAS,initialvisualanalogscale;InitialTHI, initialTinnitusHandicapInventoryquestionnaire.
symptomsbetween the placebo andcontrol groups. How-ever, they observed that the study participants showed improvementinsleepquality,bloodcirculation,andmuscle relaxation.
Inthepresentstudy,theseaspectsalsoshowed improve-ment,andthefinalresultoftheTHIquestionnaireindicates that the participants in the control group had a severe degree of interference with quality of life, which often shows sleeppatternalterations andinterference withthe activities ofdaily life.The participantsof theAG showed improvementinthedegree ofinterferencewithqualityof lifetomildaftertreatmentwithacupuncture,easilymasked bytheenvironmentandalsoeasilyforgotteninthepresence ofusualnoisesduringactivitiesofdailyliving.
In anotherstudy byJeon etal.,30 thelong-term effect of an acupuncture program for the treatment of tinnitus wasassessed.Thirty-threesubjectsweredividedintotwo groups: one group treated withacupuncture and another groupwithshamacupuncture.Theacupuncturetreatment programconsistedoftensessions, twiceaweek,lasting5 weeks.Theparticipantswereevaluatedpriortotreatment,
attheendoftreatment,andat3monthsoffollow-up.The assessmenttoolsusedweretheVASandTHIquestionnaire.In thisstudy,therewasnostatisticaldifferenceinanyoutcome betweentherealacupunctureandshamacupuncture.
However,theTHIquestionnairescoresshoweda signifi-cantimprovementattheendoftreatmentwhencompared tobaseline,andthiseffectwasmaintainedthroughoutthe follow-upperiod(after3months);however,thisresultwas notobservedintheshamacupuncturegroup.
WhencomparedthroughVAS,boththeacupunctureand thesham acupuncturegroups showedsignificant improve-ment from baseline to 3 months of follow-up. However, therewasnostatisticaldifferenceinanyoutcomebetween thetreatmentgroupandtheshamgroup.Theacupuncture groupshowedstatisticalsignificanceonlyforthemean per-centagevariationin VAS,comparedtoshamacupuncture, fromthe start of treatment until 3 months of follow-up, withp=0.019.
AsinthestudybyJeonetal.,30thepresentstudyshows anacupuncturetherapyprogramconsistingoftensessions, twiceaweek,withatotaldurationof5weeks.Thisstudy
Table2 Primaryandsecondaryendpoint,andcomparisonbetweengroups. Acupuncturegroup
(n=22)
Controlgroup(n=24) p
InitialVAS 8[7---9] 8[7.5---9.5] 0.580
FinalVAS 4[3---6] 8[8---10] 0.0001
p 0.0001 0.168
InitialTHI 56[44---65.5] 58[48---76] 0.331
FinalTHI 28[8---55.5] 68[46---76] 0.0001
p 0.0001 0.943
alsousedtheVAStooltoassesstinnitusintensity.Thistool iswidelyusedtomeasurethevolumereportedbytinnitus patients,25,31,32 mainly due to the fact that it is fast and easytoapplyand,therefore,itis easytocompareresults betweengroups.
Astatisticallysignificantdifferencewasfoundinthe vari-ationoftheVASscoresbetweentheAGandCG,andbetween theinitialandfinalevaluations,withp=0.0001.
Similarly tothe VAStool,the THI questionnaire is also oneofthemostoftenusedtoolsininternationalliteratureto assesstheinterferenceoftinnitusonqualityoflife.TheTHI questionnaireiscurrentlyoneofthemostaccepted meth-odsfor assessingtinnitus,havingbeen validatedinseveral consensuses.32ThisstudyalsousedtheTHIquestionnaireto assessthequalityoflifeofpatientswithtinnitus,asithas beenusedinseveralotherstudies.32,33
Thepresent studydemonstratedstatisticallysignificant differencesintheTHIquestionnairescoresbetweentheAG andCG,betweentheinitialandfinalevaluation.
Thisstudyshowedthatthereiseffectsoftinnitus symp-tomreliefasaresultofChinesescalpacupuncture.Other non-specificfactorsunrelatedtothevestibulocochlearline ofChinesescalpacupuncturemayberelatedtothiseffect, such as induction by the patient’s subjectivity and the increasedattentiongivenbydoctorstothestudypatients.9 Thesignificantlevelsofimprovementoftheeffect jus-tify the use of this technique. This study shows that the techniqueis safe anddoes not cause anyside effects for patients.However,more studies arerequired toestablish otherpossibleeffectsofChinesescalpacupunctureonthe auditorysystem.
Studylimitations
Amongthelimitationsofthisstudyisthelackoffollow-up. Thus,itwasnotpossibletoassesswhethertheacupuncture programhadamedium-orlong-termeffectonperceptionof tinnitus,decreaseinintensity,andimprovedqualityoflife ofindividualswithtinnitus,andwhethertheeffectiveness obtainedwaspalliativeortherapeutic.
Another limitation was the possibility of the placebo effectof the acupuncture intervention, sincethe control groupdidnotundergoanyinterventiontoobviatethis pos-sibility;thustheeffectofplacebotreatmentcannotberuled outincasesoftinnitus.
Furthermore, although this study followed the sample sizecalculation,itwouldbeprudenttoperformastudywith alargernumberofparticipants,i.e.,toensureasafety mar-ginconsideringpossiblelossesthatoccurredthroughoutthe study.
Implicationsforfuturestudies
Morestudieswithhighmethodologicalqualityandlowriskof biasarerequiredtoassesstheeffectofacupunctureonthe treatmentof tinnitus.The rules oftheConsort statement must be followed and described in detail, aswell asthe sample size calculation, sothat a systematic review with meta-analysiscanbeperformed.
Conclusion
The patients showed a significantly improved tinnitus perception. The technique of Chinese scalp acupuncture associated with bilateral electroacupuncture showed a statistically significant improvement in reducing tinnitus intensity level, aswell as improving the qualityof life in patientswithtinnitusintheshortterm.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.PintoPCL,SanchezTG,TomitaS.Avaliac¸ãodarelac¸ãoentre sev-eridadedozumbidoeperdaauditiva,sexoeidadedopaciente. BrazJOtorhinolaryngol.2010;76:18---24.
2.NorenaAJ.Anintegrativemodeloftinnitusbasedona cen-tralgaincontrollingneuralsensitivity.NeurosciBiobehavRev. 2011;35:1089---109.
3.NondahlDM,CruickshanksKJ,WileyTL,KleinBE,KleinR, Chap-pellR,etal.Theten-yearincidence oftinnitusamongolder adults.IntJAudiol.2010;49:580---5.
4.Nondahl DM, Cruickshanks KJ, Wiley TL, Klein R, Klein BE, TweedTS.Prevalenceand5-yearincidenceoftinnitusamong olderadults:theepidemiologyofhearinglossstudy.JAmAcad Audiol.2002;13:323---31.
5.Possani LNA. Estudo daprevalência e dascaracterísticas do zumbidoemtrabalhadoresexpostosaoruídoocupacional.Porto Alegre:UniversidadeFederaldoRioGrandedoSul;2006.
6.Studyoftheoccurrenceandthecharacteristicsoftinnitusina Brazilianaudiologicalclinic.SantosTMM,BrancoFCA,Rodrigues PF,BohsenYA,SantosNI,editors.ProceedingsoftheVI inter-nationaltinnitusseminar.1999.
7.GibrinPCD, MeloJJ, Marchiori LLdM.Prevalênciade queixa dezumbidoeprováveisassociac¸õescomperdaauditiva, dia-betesmellitusehipertensãoarterialempessoasidosas.CoDAS. 2013;25:176---80.
8.MoreiraMD,MarchioriLLdM,CostaVdSP,DamascenoEC,Gibrin PCD.Zumbido:possívelassociac¸ãocomalterac¸õescervicaisem idosos.ArqIntOtorrinolaringol.2011;15:333---7.
9.OkadaDM,OnishiET,ChamiFI,BorinA,CassolaN,Guerreiro VM.Acupuncturefortinnitusimmediaterelief.BrazJ Otorhi-nolaryngol.2006;72:182---6.
10.KimJI,ChoiJY,LeeDH,ChoiTY,LeeMS,ErnstE.Acupuncture forthetreatmentoftinnitus:asystematicreviewof random-izedclinicaltrials.BMCComplementAlternMed.2012;12:97.
11.MaciociaG. Osfundamentos da medicinachinesa: um texto abrangenteparaacupunturistasefitoterapeutas.2nded.São Paulo:Roca;2007.
12.YamamuraY.Acupunturatradicional:aartedeinserir.2nded. SãoPaulo:Roca;2004.
13.PomeranzB,ChiuD.Naloxoneblockadeofacupuncture analge-sia:endorphinimplicated.LifeSci.1976;19:1757---62.
14.AzevedoRFd,ChiariBM,OkadaDM,OnishiET.Efeitoda acupun-turasobreasemissõesotoacústicasdepacientescomzumbido. BrazJOtorhinolaryngol.2007;73:599---607.
15.HaoJJ,ChengW,LiuM,LiH,LuX,SunZ.Treatmentofmultiple sclerosiswithChinesescalpacupuncture.GlobAdvHealthMed. 2013;2:8---13.
17.Newman CW, Jacobson GP, Spitzer JB. Development of the TinnitusHandicapInventory.ArchOtolaryngolHeadNeckSurg. 1996;122:143---8.
18.KatzJ.Tratadodeaudiologiaclínica.SãoPaulo:EditoraManole; 1989.
19.Gorga MP, NeelyST, Dorn PA.Distortion productotoacoustic emissiontestperformancefor aprioricriteriaand for multi-frequencyaudiometricstandards.EarHear.1999;20:345---62.
20.SilmanS,SilvermanCA.Basicaudiologictesting.Auditory diag-nosis:principlesandapplications.SanDiego:SingularPublishing Group;1997.p.44---52.
21.LloydLL, Kaplan H.Audiometricinterpretation: amanual of basicaudiometry.Baltimore:UniversityParkPress;1978.
22.Azevedo AAd, Oliveira PMd, Siqueira AGd, Figueiredo RR. Análisecríticadosmétodosdemensurac¸ãodozumbido.Braz JOtorhinolaryngol.2007;73:418---23.
23.FerreiraPÉA,CunhaF,OnishiET,Branco-BarreiroFCA,Gananc¸a FF.TinnitusHandicapInventory:adaptac¸ãoculturalparao Por-tuguêsbrasileiro.Pró-FonoRAtualCient.2005;17:303---10.
24.SchmidtLP, TeixeiraVN, Dalligna C,Dallagnol D,Smith MM. Adaptac¸ão para língua portuguesa do questionário Tinnitus HandicapInventory:validadeereprodutibilidade.BrazJ Otorhi-nolaryngol.2006;72:808---10.
25.MarksNJ,EmeryP,OnisiphorouC.Acontrolledtrialof acupunc-tureintinnitus.JLaryngolOtol.1984;98:1103---9.
26.Axelsson A, Andersson S, Gu LD. Acupuncture in the man-agement of tinnitus: a placebo-controlled study. Audiology. 1994;33:351---60.
27.TanKQ,ZhangC,LiuMX,QiuL.Comparativestudyon therapeu-ticeffectsofacupuncture,ChineseherbsandWesternmedicine onnervoustinnitus.ZhongguoZhenJiu.2007;27:249---51.
28.Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evi-denceofbias.Dimensionsofmethodologicalqualityassociated withestimatesoftreatmenteffectsincontrolledtrials.JAMA. 1995;273:408---12.
29.DaySJ,AltmanDG.Statisticsnotes:blindinginclinicaltrials andotherstudies.BMJ.2000;321:504.
30.Jeon SW, Kim KS, Nam HJ. Long-term effect of acupunc-ture for treatment of tinnitus: a randomized, patient- and assessor-blind, sham-acupuncture-controlled, pilot trial. J AlternComplementMed.2012;18:693---9.
31.FurugardS,HedinPJ,EggertzA,LaurentC.Acupunctureworth tryinginseveretinnitus.Lakartidningen.1998;95:1922---8.
32.Figueiredo RR, Azevedo AAD, Oliveira PDM. Análise da correlac¸ãoentre a escala visual-análoga eo Tinnitus Handi-capInventorynaavaliac¸ãodepacientescomzumbido.BrazJ Otorhinolaryngol.2009;75:76---9.

![Table 1 Characteristics of the participants assessed before treatment. Groups AG (n = 22) p CG (n = 23) p Gender, n (%) Male 8 (36.3) 10 (43.4) Female 14 (63.7) 13 (56.6) Age (years) 62 [57---67.5] 60 [54.5---62] Hearing (n; %) Bilateral loss 17 (77.3) 18](https://thumb-eu.123doks.com/thumbv2/123dok_br/15416891.588562/6.918.73.833.112.427/characteristics-participants-assessed-treatment-groups-gender-hearing-bilateral.webp)
