www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
The
place
of
hyperbaric
oxygen
therapy
and
ozone
therapy
in
sudden
hearing
loss
夽
Gülin
Ergun
Tas
¸döven
a,∗,
Alper
Tunga
Derin
b,
Neslihan
Yaprak
b,
Hasan
Ümit
Özc
¸a˘
glar
baVanTrainingAndResearchHospital,DepartmentofOtorhinolaryngology,Van,Turkey bAkdenizUniversity,SchoolofMedicine,DepartmentofOtorhinolaryngology,Antalya,Turkey
Received15February2016;accepted2June2016 Availableonline6July2016
KEYWORDS
Hyperbaricoxygen therapy;
Idiopathicsudden sensorineuralhearing loss;
Oralsteroid; Ozonetherapy
Abstract
Introduction:Itisdifficulttoevaluatetheeffectofdrugsclinicallyusedforidiopathicsudden sensorineuralhearingloss,mainlybecauseitsunderlyingmechanismremainsunknown.
Objective: Thisstudyassessedtheefficacyofhyperbaricoxygentherapyorozonetherapyin thetreatmentofidiopathicsuddensensorineuralhearingloss,wheneithertherapywasincluded withsteroidtreatment.
Methods:Aretrospectiveanalysisexamined106patientswithidiopathicsuddensensorineural hearinglossseenbetweenJanuary2010andJune2012.Thosewithanidentifiedetiologywere excluded.The patientsweredividedinto threetreatment groups:oralsteroidonly(n=65), oral steroid+hyperbaricoxygen(n=26),andoral steroid+ozone(n=17).Treatmentsuccess wasassessedusingSiegelcriteriaandmeangainsusingpre-andpost-treatmentaudiograms.
Results:Thehighestresponseratetotreatmentwasobservedintheoralsteroid+ozonetherapy group(82.4%),followedbytheoralsteroid+hyperbaricoxygen(61.5%),andoralsteroidgroups (50.8%).Therewerenosignificantdifferencesintheresponsetotreatmentbetweentheoral steroidandoralsteroid+hyperbaricoxygengroups(p<0.355).Theoralsteroid+ozonegroup showedasignificantlyhigherresponseratetotreatmentthantheoralsteroidgroup(p=0.019). There werenosignificantdifferencesbetween theoralsteroid+hyperbaricoxygenandoral steroid+ozonegroups(p=0.146).
Conclusion: Theefficiencyofsteroidtreatmentinpatientswithseverehearinglosswaslow.It wasstatisticallyascertainedthataddinghyperbaricoxygenorozonetherapytothetreatment contributedsignificantlytotreatmentsuccess.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:ErgunTas¸dövenG,DerinAT,YaprakN,Özc¸a˘glarHÜ.Theplaceofhyperbaricoxygentherapyandozonetherapy
insuddenhearingloss.BrazJOtorhinolaryngol.2017;83:457---63. ∗Correspondingauthor.
E-mail:[email protected](G.ErgunTas¸döven).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCervico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.06.002
1808-8694/©2016Associac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.PublishedbyElsevierEditoraLtda.Thisisanopen
PALAVRASCHAVE
Oxigenoterapia hiperbárica; Surdezsúbita; Esteroideoral; Ozonioterapia
Opapeldaoxigenoterapiahiperbáricaedaozonioterapianasurdezsúbita
Resumo
Introduc¸ão:É difícilavaliar oefeito dos fármacos clinicamenteutilizadosna surdez súbita idiopática,principalmenteporqueoseumecanismosubjacentesemantémdesconhecido.
Objetivo:Avaliaraeficáciadaoxigenoterapiahiperbáricaouozonioterapianotratamentode surdezsúbita,quandoumaououtraterapiaéincluídanotratamentocomesteroides.
Método: Umaanáliseretrospectivaexaminou106pacientescomsurdezsúbitaatendidosentre janeirode 2010ejunho de 2012. Aquelescom umaetiologiaidentificada foramexcluídos. Ospacientesforamdivididos em três gruposde tratamento:apenas esteroide oral (n=65), esteroide porviaoral+oxigenoterapia hiperbárica(n=26) eesteroidespor viaoral+ozônio (n=17).OsucessodotratamentofoiavaliadocomcritériosdeSiegeleosganhosmédioscom audiogramaspréepós-tratamento.
Resultados: A taxa de resposta mais elevada para o tratamento foi observada no grupo de esteroide+ozonioterapia (82,4%), seguida por grupos de esteroide oral+oxigenoterapia hiperbárica(61,5%)eesteroideoral (50,8%).Nãohouvediferenc¸assignificantesnaresposta ao tratamento entre os grupos de esteroide oral e esteroides+oxigenoterapia hiperbárica (p<0,355).O grupo de esteroide oral+ozônio apresentou uma taxa de resposta significan-temente mais elevada ao tratamento do que o grupo de esteroide oral (p=0,019). Não houvediferenc¸assignificantesentreosgruposdeesteroideoral+oxigenoterapiahiperbárica eesteroideoral+ozônio(p=0,146).
Conclusão:Aeficiênciadotratamentocomesteroidesempacientescomperdaauditivagrave foi baixa.Verificou-se estatisticamentequeaadic¸ão deoxigenoterapiahiperbáricaou ozo-nioterapiaaotratamentocontribuiusignificantementeparaosucessodotratamento. © 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Idiopathicsuddensensorineuralhearingloss(ISSNHL)isan otologicdiseaserequiringurgent diagnosisandtreatment. ISSNHLis commonly definedas hearingloss of more than 30dB,affectingthreeormorefrequencies,arisingoverless than3days,withoutanidentifiableetiology.1Thehearing
lossdevelops withina few seconds,minutes, or hours.In severalepidemiologicalstudiesconductedontheincidence ofISSNHL,thespontaneousrecoveryrateofISSNHLishigh; theactualincidenceisestimatedtobefarabovethisvalue. Although several factors account for its etiology,most casesareidiopathic.Althoughtherearemorethan100 con-sidered etiologic causes, the widely accepted etiological theoriesareviralinfections,vascularcauses,cochlear mem-branedisorders,andautoimmunity.Inmanycases,however, noapparentcausecanbeindicated.2---4Theetiologycanbe
clarifiedin10---15% ofcases,withISSNHLdiagnosedinthe remainder.2,4,5
Although ISSNHL recurs spontaneously in 32---65% of cases,6 the reported rate ranged between 49% and 89%
whensteroidswereusedduringtreatment.7Steroidsremain
themostcommonly usedmedicationfor thetreatment of ISSNHL.
The idea that ISSNHL could occur due to hypoxia in the cochlear apparatus makes hyperbaric oxygen therapy (HBOT) a reasonable choice. Generally, HBOT is recom-mended for the treatment of ISSNHL as a supplementary therapytothefirst-linemedicaltreatment.
Recently,ozonetherapyhasbeenusedasa supplemen-tary treatmentfor diseaseswhere inflammatoryprocesses arepreponderantandanischemicetiologyisfound.Ozone therapy is considered a treatment for ISSNHL becauseits effects,suchasenhancingoxygen,glucose,andadenosine triphosphate(ATP)deliverytoischemictissues,inturn pro-ducingreactiveoxygenderivatives,resultinvasodilationby increasingtheamountofnitricoxide,stimulating angiogen-esisandprovidingimmunomodulation.
Ourstudyincluded 106patients withISSNHLwhowere treatedatourclinicbetween2010and2012.We retrospec-tivelyinvestigatedtheefficacyof thetreatmentprotocols applied to patients with ISSNHL, and studied the role of HBOT or ozonetherapy for the treatment of ISSNHLwith either therapy administered as a supplement to systemic steroidtreatment.
Methods
Patients
frequencies developing within 3 days. Pediatric patients, patientswithpreexistingMeniere’sdisease,tumors, acous-tic trauma, barotrauma, retrocochlear disease, bilateral hearing loss, those witha history of chronic otitis in the sameear,andthosewitha historyofsurgeryofthe same earwerenotincludedinthestudy.Thosepatientswithan identifiedcause wereexcluded, andonly idiopathic cases wereinvestigated.Bilateral caseswerealsonotincluded. Inall,62(58.5%)ofthestudyparticipantsweremaleand44 (41.5%)werefemale.Themeanagewas50±13years;the oldestperson was81 years,whereas theyoungest person was17years.Allofthepatientshadrepeatedaudiological testsonthe first,third, fifth,seventh,and fifteenthdays oftreatment.InaccordancewiththeAmericanSpeechand Hearing Association guidelines, hearingloss was classified asmild(26---40dB),moderate(41---55dB),moderate-severe (56---70dB),severe(71---90dB),andprofoundortotal(91dB and above) loss according to the average pure tone thresholds at 500, 1000, 2000, and 4000Hz. Temporal magnetic resonance imaging was requested for all of the patients to evaluate the acoustic channel and brain stem.
Treatmentgroups
Thepatientsweredividedintothreegroupsaccordingtothe treatment protocol received: oral steroid (Group A), oral steroid+HBOT (Group B), and oral steroid+ozone(Group C).Theoral steroidgroupcomprised63patients,theoral steroid+HBOT group comprised 26 patients, and the oral steroid+ozone groupcomprised 17 patients.According to our clinic’sprotocols for ISSNHLwith oral steroids, all of thepatientsweregiven1mg/kg/dayoralprednisolonefor 5days,themaximumdosegiventopatientswas60mg/day, whichwassubsequentlytaperedby10mgevery2days;at the sametime, 30mg/day gastroprotective oral lansopra-zole anda salt-free diet combination were administered. Theoralsteroidtreatmentisdoneforallthepatients rou-tinely.Duringthepast6years,hyperbaricoxygentherapy and ozone therapy has been applied asadjunctive treat-ment in our clinic for ISSNHL.Since then, we have given informationandrecommendabout theozonetherapy and hyperbaricoxygentreatment.Andifthepatientwantone of these treatments; this treatment add to the steroid treatment.Sincethehyperbaricoxygentherapyandozone therapywhicharesupplementarytreatmentmethodstothe routinetreatments,arenotpaidforbytheinsurance com-paniesin our country, none of our patients couldreceive thesetreatments.
Thesocio-economicandtransportationstatuswas influ-ential in choosing the treatment method. The reason for thenumberofthepatientswhoreceivedhyperbaricoxygen therapyandozonetherapy beingfewstemsfromthe fact thatnotallpatientsacceptthistreatmentbecauseithasa feetobepaid.
Thepatientsintheoralsteroid+HBOTgroup,inaddition to receiving oral steroids according tothe ISSNHL proto-col,receivedHBOTappliedas100%oxygeninhalationat2.5 ATApressurefor90min,whichwasadministeredonceaday withina10dayperiod(HiperbotModel101;HiperbotLtd, ˙Istanbul).
Thepatientsintheoralsteroid+ozonegroup,inaddition toreceivingoralsteroidsaccordingtotheISSNHLprotocol, received medical ozonetherapy using the major autohe-motherapymethod.Inthismethod,ananti-ozonantinfusion set(Ozonosan;Mikro-Perl-System;Dr.J.Hänsler,Iffezheim, Germany)and100mLblood drawn fromthepatientwere mixed, under sterile conditions, with 99.5% oxygen and 0.5%ofanozonemixture(theozoneconcentrationwithin themixture=20g/mL)obtainedfromanozonegenerator
(MedozonCompact;HerrmannApparatebau,Kleinwallstadt, Germany);thisbloodmixturewasagainadministeredtothe patientintravenously,atleastfora5-minperiod.Duringthe courseoftheprocess,sodiumcitratewasusedasan antico-agulant.Thistherapy wasperformedinfivesessionstwice a week. The ozonetherapy protocol that used by Ragab andhisfriendsontheir searchabout thistopic; alsoused assource (Ragab A, Shreef E, Behiry E, Zalat S, Noaman M.Randomised,doubleblinded,placebo-controlled,clinical trialofozonetherapyastreatmentofsuddensensorineural hearingloss.JLaryngolOtol.2009;123:54---60).
Audiometricinvestigation
To determine the change in post-treatment hearing, pre-treatment audiological examination and post-treatment audiologicalexamination wereperformedonthefifteenth day(thethresholdaveragesat500,1000,2000,and4000Hz werecompared)(ClinicalAudiometersAC-40Interacoustics, Assens,Denmark).
TheresultswereevaluatedconsideringchangesinSpeech DiscriminationScores(SDSs)andPureToneAverages(PTAs) at500,1000,2000,and4000Hz.
The response to therapy was categorizedaccording to Siegel’scriteria8asfollows:
1. Healing:finalthresholdmorethan25dB.
2. Partialimprovement:gainofmorethan15dB,final hear-ingthreshold25---45dB.
3. Slightimprovement:gainofmorethan15dB,final hear-ingthresholdmorethan45dB.
4. No response: gain of less than 15dB and final hearing thresholdmorethan75dB.
APTAgreater than15dB wasconsidereda responseto treatment,whereasa PTAlessthan 15dBwasdeemed no responsetotreatment.Iftheincreaseinthepre-vs. post-treatmentSDSofthepatientswasmorethan20%,thevalue wasconsidered a response to treatment; however, if the increase wasless than 20%, the value wasconsidered no responsetotreatment.
Table1 Theclassificationoftheinitialhearinglossdegreesofthegroups.
Group Mild Moderate Moderate-severe Severe Profoundortotal
A 3(4.8%) 10(15.9%) 15(23.8%) 14(22.2%) 21(33.3%)
B 1(3.8%) 4(15.4%) 2(7.7%) 4(15.4%) 15(57.7%)
C 0 3(17.6%) 2(11.8%) 2(11.8%) 10(58.8%)
A,oralsteroidgroup;B,oralsteroid+hyperbaricoxygengroup;C,oralsteroid+ozonegroup.
Statisticalanalysis
AllstatisticalanalyseswereperformedusingtheStatistical PackagefortheSocialSciences(SPSS)forWindows7.0PASW Statistics18(SPSS,Chicago,IL,USA).Atwo-tailedt-testwas used for descriptive statistical analysis (mean±standard deviation)ofquantitativedata.Ap-valueof<0.05was con-sideredtoindicatestatisticalsignificance.
The university ethics council approved this study
(05/02/2013.Decisionn◦ 43).Ourstudywasperformed as
retrospectively. We have started todo hyperbaric oxygen therapyandozonetherapyonourclinicsince2010forthe patientswhohadsuddensensorineuralhearingloss.We con-ductedthestudyin2013retrospectivelyandthosepatients whomwefollowed-upandtreatedfrom2010to2012were included in the study. Because of this our ethics board approvalwasdated2013.
Results
Groups
In total, 106 patients who complied with the participa-tioncriteriaofthe study wereselected.The cases inthe presentstudyweredividedintothreegroupsasfollows:63 patientswithoralsteroidtreatment(GroupA),26patients withoralsteroid+HBOT(GroupB),and17patientswithoral steroid+ozonetherapy(GroupC).Nostatisticallysignificant differencewasfoundamongthegroupsregardingageand sex.
PTA
Whentheinitialpre-treatmentPTAs(PTPTAs)ofthepatients were analyzed, the average of all study participants was 85.8dB. By group, the values were 80.7dB in Group A, 92.02dB in Group B,and 94.9dB in Group C. No statisti-callysignificantdifferencewasobservedamongthegroups (p=0.084)inKruskal---Wallistests(Table1).
Responsetotreatment
When the groups were analyzed using Siegel’s criteria accordingtotheirrecoverylevels,GroupAshowedcomplete recoveryin14(22.2%)cases,partialrecoveryin10(15.9%) cases, weakrecovery in 8 (12.7%)cases, andno recovery in31(49.2%)cases.GroupBdemonstratedcomplete recov-eryin3(11.5%)cases,partialrecoveryin4(15.4%)cases, weak recovery in 9 (34.6%) cases, and no recovery in 10 (38.5%)cases.InGroupC,completerecoverywasobserved in3(17.6%)cases,partialrecoveryin4(23.5%)cases,weak recovery in 7 (41.2%)cases, andnorecovery in 3 (17.6%) cases(Table2).
APTAgreaterthan 15dBwasconsidered aresponseto treatment, whereasaPTAless than15dBwasdeemedno responsetotreatment.Thehighestresponseratewasfound intheoralsteroid+ozonegroup(GroupC)(82.3%),followed bytheoralsteroid+HBOTgroup(GroupB)(61.5%)andthe oralsteroidgroup(GroupA)(50.8%).
Pearson’schi-squaredtestsindicated nosignificant dif-ferencesintheresponsetotreatmentbetweenGroupsAand B(p<0.355).GroupCshowedasignificantlyhigherresponse ratetotreatmentthanGroupA(p=0.019).Therewereno significant differencesbetween groups BandC (p=0.146) (Table3).
Regarding SDSs, a statistically significant increase was found following treatment in each of the three groups (p=0.002),withnostatisticallysignificantdifferenceinthe degreeofincreaseamongthegroups.
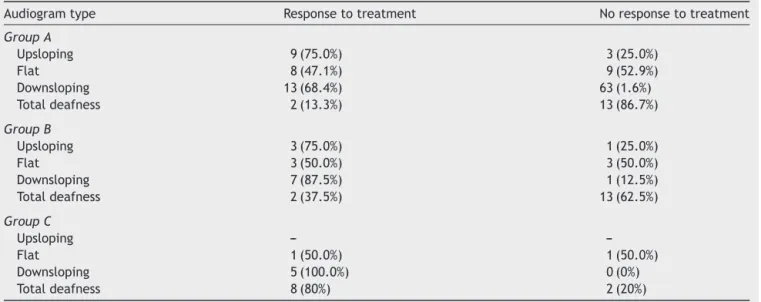
Theaudiogramcurvewasupslopingin16(15%)patients, downslopingin32(30.1%),flatin25(23.5%),andindicated totaldeafnessin33(31.1%)patients.Thegroups participat-inginthestudy wereevaluatedasshowinga‘responseto treatment’or‘noresponsetotreatment’ accordingtothe typesofaudiograms(Table4).
Theefficiencyofsteroidtreatmentinpatientswith pro-foundhearingloss(91dBandabove)waslow;addingHBOT orozonetherapytothetreatmentsignificantlycontributed totreatmentsuccess.
Consideringpatientswithprofound hearingloss only, a statisticallysignificantdifferenceinresponsetotreatment wasfoundbetweenGroupsAandB(p=0.012)andespecially
Table2 Thegroups’responseratestotreatmentaccordingtosiegel’scriteria.
Group Completerecovery Partialrecovery Weakrecovery Norecovery Total
A 14(22.2%) 10(15.9%) 8(12.7%) 31(49.2%) 63
B 3(11.5%) 4(15.4%) 9(34.6%) 10(38.0%) 26
C 3(17.6%) 4(23.5%) 7(41.2%) 3(17.6%) 17
Table3 Thegroups’responsetothetreatment.
Groups Responsetotreatment Noresponsetotreatment Total
A 32(50.8%) 31(49.2%) 63
B 16(61.5%) 10(38.5%) 26
C 14(82.4%) 3(17.6%) 17
A,oralsteroidgroup;B,oralsteroid+hyperbaricoxygengroup;C,oralsteroid+ozonegroup. Thereisresponsetotreatment:gainingPTAabove15dB.
Thereisnoresponsetotreatment:gainingPTAlessthan15dB.
Table4 Thegroups’responsetotreatmentaccordingtoaudiogramshape.
Audiogramtype Responsetotreatment Noresponsetotreatment
GroupA
Upsloping 9(75.0%) 3(25.0%)
Flat 8(47.1%) 9(52.9%)
Downsloping 13(68.4%) 63(1.6%)
Totaldeafness 2(13.3%) 13(86.7%)
GroupB
Upsloping 3(75.0%) 1(25.0%)
Flat 3(50.0%) 3(50.0%)
Downsloping 7(87.5%) 1(12.5%)
Totaldeafness 2(37.5%) 13(62.5%)
GroupC
Upsloping ---
---Flat 1(50.0%) 1(50.0%)
Downsloping 5(100.0%) 0(0%)
Totaldeafness 8(80%) 2(20%)
A,oralsteroidgroup;B,oralsteroid+hyperbaricoxygengroup;C,oralsteroid+ozonegroup. Thereisresponsetotreatment:gainingPTAabove15dB.
Thereisnoresponsetotreatment:gainingPTAlessthan15dB.
Table5 Responsetothetreatmentinpatientswithprofoundhearingloss.
Patientswithprofoundhearingloss Responsetotreatment Noresponsetotreatment Total
GroupA 4(19%) 17(81%) 21
GroupB 9(60%) 6(40%) 15
GroupC 8(80%) 2(20%) 10
A,oralsteroidgroup;B,oralsteroid+hyperbaricoxygengroup;C,oralsteroid+ozonegroup.
betweenGroupsAandC(p=0.002).Nostatistically signifi-cantdifferencewasfoundbetweengroupsBandC(Fisher’s exacttest)(Table5).
Discussion
The factors affecting prognosis in ISSNHL include the patient’sage, existenceof vertigo,degree ofinitial hear-ingloss,shapeoftheaudiogram, andperiodbetween the onset of hearing loss and start of treatment. The degree ofhearingloss isan importantfactorthat determinesthe responsetotreatment.Profoundhearinglossof90dBand aboveindicatesapoorprognosis.
Byletal.4reportedan83%rateofrecoveryinpatients
withmildhearinglossand22%recoveryinthosewithsevere hearingloss.Intheirplacebo-controlledstudythatincluded
steroidtreatment,Wilsonetal.9observedcomplete
recov-ery in all of the patients with a hearing loss of 40dB or less and in patients with a U-shaped hearing loss up to 85dB.However,only 24%of thosewithaflat hearingloss of90dBandaboveappearedtorecover;inaddition,none showedtotalrecovery.Steroidtreatment wasmost effec-tivein patients witha hearing lossof between 40dB and 90dB;only38%ofthesepatientsrecoveredintheplacebo group,whereasapproximately78%recoveredinthesteroid group.
oralsteroid+ozonegroups(p=0.002;Pearson’sChi-squared test).
However, the efficiency of the oral steroid treatment was low in patients with profound hearing loss. In the present study, the response to treatment witha total or close-to-totaltypeofaudiogram configurationwaslow,in concordancewiththeliterature.
RecoveryinISSNHLmostlyoccurswithinthefirst2weeks. Thelongertherecoverytime,theworsetheprognosis. Com-pleteor partialrecoverywithouttreatment isobservedin manypatients(32---65%).9,10
Presently,morethan60treatment protocolshavebeen defined,butnopreciseconsensusexistsregardingwhichis best.Onewidelyacceptedtreatmentissteroidtreatment.
Steroids have several effects on the inner ear. They suppress the immune system and increase the microcir-cular current. They have mineralocorticoid effects, and arethoughttoinfluenceISSNHLby reducingthe endolym-phaticpressure.However,thepreciseunderlyingmechanism remainsunknown.11,12
Therearetwotypesof corticoid receptors,type1and type2,incochlearandvestibularcells.13,14When
glucocor-ticoid receptors are activated,a specific gene expression program is launched; thus, the synthesis of inflammatory mediators and cytokines is inhibited, resulting in anti-inflammatoryeffects.
In thefirstrandomized, controlledstudy ontheuse of steroids in ISSNHL,the authors compareda steroid anda placebo.Intheactivemedicationgroup,theyadministered prednisoloneorallyingraduallyreducedamountsfor10---12 days.All ofthepatients (n=14)withmoderate-frequency hearing losses recovered regardless of the type of treat-ment. In patients whose loss wasworse than 90dB at all frequencies,nodifferencecouldbefoundintermsof recov-erybetweenthesteroidandplacebotreatment groups.In theremainingpatientpopulation(with non-severehearing lossandhearingat4kHzbetterthanat 8kHz),significant recoverywasmonitoredinthegroupthatwasadministered steroids.Whilecomplete recovery wasachievedin 78%of thoseadministeredsteroids,thoseadministeredtheplacebo achieved38% partial recovery.9 In a previous prospective
randomized study, 89% of a group administered corticos-teroidtreatmentrecovered,whereasonly44%ofthecontrol groupadministeredplaceborecovered.7
HBOT has been usedto treat inner-eardisorders since the early 1970s.15 In the late 1970s, several researchers
suggestedthatcirculatorydisorderswerethemain reason for ISSNHL.Consequently, HBOT becamea comprehensive treatmentoptionforISSNHL.16
The purposeof HBOT in the treatment of ISSNHL is to increase the partial pressure of oxygen in the blood and then,viadiffusion,toincreasethepartialpressureofoxygen intheinnerearfluidsthatnourishthesensoryandneural elementsofthecochlea.17
Fujimura et al.18 claimed that HBOT had a significant
additionaleffectwhenusedin combination withsystemic steroid therapy in 43 patients, when compared with 51 patientswhoweretreatedwithsteroidsalone.Inpatients withinitialhearinglevelsof≥80dB,thehearing improve-ment rate was significantly higher in the HBOT group than in the steroid group, whereas in patients with ini-tial hearing levels of <80dB, the hearing improvement
rate was not statistically different between the two groups.
Alimogluetal.,19whoconsidered217patients,
adminis-teredanoralsteroidto58patients,oralsteroid+HBOTto 61patients,intratympanicsteroidto43patients,andonly HBOTto57patients.Thetreatmentsuccessratewas high-estinthesteroid+HBOTgroup(86.88%;53/61),followedby the oral steroidgroup (63.79%;37/58), the intratympanic steroid group (46.51%; 20/43), and the only HBOT group (43.85%;25/57).
Topuzetal.20showedthatHBOThadagreatereffecton
hearingatlowfrequenciesthanathigherfrequencies, par-ticularly inyoung patients.In particular,patients younger than50intheHBOTgrouphadbetterhearingoutcomes.
AlthoughtheetiologyandpathogenesisofISSNHLarenot completelyunderstood,vascularcausesareamongthe pri-maryunderlyingetiologies.Exceptforthosewithadefinite contraindication,addingHBOTtothetreatment ofISSNHL isacommonstrategy.
Inourstudy,thegroup administeredsteroidtreatment experienced a 50.8% treatment response, whereas the steroid+HBOTgrouphadabetterresponse,at61.5%.
Although the patients who received steroid treatment and those who received HBOT in addition to steroid treatment showed similar responses to treatment, the HBOTsupplementpositivelycontributedtotherecoveryof patientswithsevereorprofoundhearingloss.
OzonetherapyisatreatmentstrategyforISSNHLbecause itenhancesoxygen,glucose,andATPdeliverytoischemic tissues, and leads to vasodilation, increasing the amount of nitric oxide, stimulating angiogenesis, and providing immunomodulation. Hydrogen peroxide, a derivative of reactive oxygen metabolites that generates ozone in the body,isnowwidelyrecognizedasanintracellularsignaling moleculethatactivatesatyrosinekinase,which phosphory-latesatranscriptionfactor(NuclearFactorkappaB;NF-B),
whichallowsthesynthesisofseveraldifferentproteins.21---23
Recently,anewhypothesisofpathologicalactivationof thecellularstresspathwaysinvolvingNF-Binthecochlea
wassuggested.PathologicalactivationofNF-Bcanresultin
theproductionofinflammatorycytokinesandother stress-relatedproteins thatcandisrupt thehomeostaticbalance of acell or tissue.24 Afterozonation, H
2O2 freely diffuses into thecytoplasm and activatesspecific protein kinases, which---byphosphorylatingI[kappa]BboundtoNF-b---
reg-ulate its action and allow migration of the transcription heterodimer p50---p65 into cell nuclei, where it activates gene expression.25 Ozone also induces up-regulation of
antioxidant enzymes in several cell types, which effec-tivelyre-equilibratestheoxidant---antioxidantimbalance.25
Therefore, ozone therapy can bean effective method of treatment according to the cellular stress hypothesis in ISSNHL.
InastudybyRagabetal.26 comprising45patientswith
the recovery of hearing in the placebo group was40%, a significantdifference.Ozonetherapy,byproducingreactive oxygenderivatives,causesthehemoglobin-oxygen dissoci-ationcurve toslide/sliptothe right, therebycausing the oxygen to be more easily delivered into tissues; further-more,thistherapyenhancesnitricoxideoscillation/release, which is a powerful vasodilator of endothelial cells, and fixesischemiainthecochlea.Inadditiontothesefeatures, ozonetherapyincreasesantioxidantefficiencyandbecomes effectiveforthetreatmentofISSNHLbyimpactingcellular stress.26
Inanotherstudy,27patientswithtinnituswere admin-istered ozone therapy, 26 were administered betahistine treatment,and15comprisedacontrolgroup;asignificant decline was observed in average tinnitus disability ques-tionnairescoresandsubjectivetinnitusscoresintheozone groupaftertreatment(p<0.001).A22.2%recoveryratewas achievedaccordingtotheseverityoftinnitusinpatients,a 44.4% recovery rate was achievedaccording tothe tinni-tusdisabilityquestionnaires,anda40.7%recoveryratewas determinedaccordingtothesubjectivetinnitusscores.27
Inthisstudy,inthesteroidtreatment group(GroupA), there wascomplete recovery in 14 (22.2%) cases, partial recovery in 10 (15.9%), weak recovery in 8 (12.7%), and norecoveryin31(49.2%).Inthegroupadministeredozone therapyinadditiontosteroidtreatment(GroupC),3cases (17.6%) had total recovery, 4 cases had partial recovery (23.5%),and7caseshadweakrecovery (41.2%);however, norecoverywasobserved in3(17.6%)ofthecasesin this group.The highest responseratetotreatment wasin the steroid+ozonetherapygroup(GroupC)(82.4%),followedby thesteroid+HBOTgroup(GroupB)(61.5%),andoralsteroid group(GroupA)(50.8%).
Conclusion
The results of our study demonstrate that ozone ther-apy significantly contributes to the recovery process in treatment of ISSNHL; however, we believe that further placebo-controlled studies should be performed with a greater number ofpatients receiving ozonetherapy for a longerperiodandwithahigherozonedose.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.NationalInstituteofHealth.Suddendeafness.Bethesda,MD: NationalInstitutesofHealth;2000.NIHpublication00-4757.
2.BylFMJr.Suddenhearingloss:8years’experienceand sug-gestedprognostictable.Laryngoscope.1984;94:647---61.
3.Arts HA. Differentialdiagnosis of sensorineural hearing loss. CummingsCWotolaryngologyhead&necksurgery,vol.4,3rd ed.Philadelphia:Mosby-YearBook,Inc.;1998.p.2923---8.
4.BylF.76cases ofpresumedsuddenhearinglossoccurringin 1973:prognosisandincidence.Laryngoscope.1977;87:817---25.
5.Hughes GB, Freedman MA, Haberkamp TJ, Guay ME. Sud-den sensorineural hearing loss. Otolaryngol Clin North Am. 1996;29:393---405.
6.FettermanBL,SaundersJE,LuxfordWM.Prognosisand treat-ment of sudden sensorineural hearing loss. Am J Otol. 1996;17:529---36.
7.MoskowitzD,LeeKJ,SmithHW.Steroiduseinidiopathicsudden sensorineuralhearingloss.Laryngoscope.1984;94:664---6.
8.SiegelLG.The treatmentof idiopathic suddensensorineural hearingloss.OtolaryngolClinNorthAm.1975;8:467---73.
9.WilsonWR,BylFM,LairdLN.Theefficacyofsteroidsinthe treat-mentofidiopathicsuddenhearingloss.Adouble-blindclinical study.ArchOtolaryngol.1980;106:772---6.
10.MattoxDE,SimmonsFB.Naturalhistoryofsuddensensorineural hearingloss.AnnOtolRhinolLaryngol.1977;86:463---80.
11.GarcíaBerrocalJR,Ramírez-CamachoR.Immuneresponseand immunopathologyoftheinnerear:anupdate.JLaryngolOtol. 2000;114:101---7.
12.Mort DJ, Bronstein AM. Sudden deafness. Curr OpinNeurol. 2006;19:1---3.
13.Erichsen S, Bagger-Sjöback D, Curtis L, Zuo J, Rarey KE, Hultcrantz M.Appearence of glicocorticoidreceptors in the innerearofthemouseduringdevelopment.ActaOtolaryngol. 1996;16:721---4.
14.FurutaH,MoriN,SatoC.MineralocorticoidtypeIreceptorinthe ratcochlea:mRNAidentificationbypolymerasechainreaction andinsituhybridization.HearRes.1994;78:175---80.
15.Lamm H, Klimpel L. Hyperbaric oxygen therapy in inter-nal ear and vestibular disorders. Preliminary report. HNO. 1971;19:363---9.
16.HauptH,ScheibeF,LudwigC.Changesincochlearoxygenation, microcirculationandauditoryfunctionduringprolongedgeneral hypoxia.EurArchOtorhinolaryngol.1993;250:396---400.
17.LammK,LammH,ArnoldW.Effectofhyperbaricoxygen ther-apyin comparisonto conventionalor placebotherapy orno treatmentinidiopathicsuddenhearingloss,acoustictrauma, noise-inducedhearinglossandtinnitus.Aliteraturesurvey.Adv Otorhinolaryngol.1998;54:86---99.
18.FujimuraT,SuzukiH,ShiomoriT,UdakaT,MoriT.Hyperbaric oxygenandsteroidtherapyforidiopathicsuddensensorineural hearingloss.EurArchOtorhinolaryngol.2007;264:861---6.
19.Alimoglu Y, Inci E, Edizer DT, Ozdilek A, Aslan M. Efficacy comparisonoforalsteroid,intratympanicsteroid,hyperbaric oxygen and oral steroid+hyperbaric oxygen treatments in idiopathic sudden sensorineural hearing losscases. EurArch Otorhinolaryngol.2011;268:1735---41.
20.TopuzE,Yi˘gitO,CinarU,SevenH.Shouldhyperbaricoxygenbe addedtotreatmentinidiopathicsuddensensorineuralhearing loss?EurArchOtorhinolaryngol.2004;261:393---6.
21.BocciV.OZONE.Anewmedicaldrug.2nded.Dordrecht,The Netherlands:Springer;2011.p.23---4.
22.BaeuerlePA,HenkelT.FunctionandactivationofNF-Binthe immunesystem.AnnuRevImmunol.1994;12:141---79.
23.BarnesPJ,KarinM.Nuclearfactor-kappaB:apivotal transcrip-tion factor in chronic inflammatory diseases. NEngl JMed. 1977;336:1066---71.
24.Merchant SN, Adams JC, Nadol JB Jr. Pathology and patho-physiologyofidiopathicsuddensensorineuralhearingloss.Otol Neurotol.2005;26:151---60.
25.Di Paolo N, Gaggiotti E, Galli F. Extracorporeal blood oxy-genationandozonation:clinicalandbiologicalimplicationsof ozonetherapy.RedoxRep.2005;10:121---30.
26.RagabA,ShreefE,BehiryE,ZalatS,NoamanM.Randomised, doubleblinded,placebo-controlled,clinicaltrialofozone ther-apy as treatment of sudden sensorineural hearing loss. J LaryngolOtol.2009;123:54---60.