REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
CLINICAL
INFORMATION
Cerebral
venous
thrombosis
after
spinal
anesthesia:
case
report
夽
Flora
Margarida
Barra
Bisinotto
a,b,∗,
Roberto
Alexandre
Dezena
c,
Tania
Mara
Vilela
Abud
d,
Laura
Bisinotto
Martins
eaUniversidadeFederaldoTriânguloMineiro,DisciplinadeAnestesiologia,Uberaba,MG,Brazil bUniversidadeFederaldoTriânguloMineiro,HospitaldeClínicas,Uberaba,MG,Brazil cUniversidadeFederaldoTriânguloMineiro,DisciplinadeNeurocirurgia,Uberaba,MG,Brazil dUniversidadeFederaldoTriânguloMineiro,Uberaba,MG,Brazil
eUniversidadedeRibeirãoPreto,RibeirãoPreto,SP,Brazil
Received3September2014;accepted10September2014
Availableonline27March2017
KEYWORDS
Spinalanesthesia; Complications post-duralpuncture headache;
Cerebralvenous thrombosis
Abstract
Introduction:Cerebralvenousthrombosis(CVT)isararebutseriouscomplicationafterspinal anesthesia.Itisoftenrelatedtothepresenceofpredisposingfactors,suchaspregnancy, puer-perium,oralcontraceptiveuse,andmalignancies.Headacheisthemostcommonsymptom.We describeacaseofapatientwhounderwentspinalanesthesiaandhadpostoperativeheadache complicatedwithCVT.
Casereport: Malepatient,30yearsold,ASA1,whounderwentuneventfularthroscopicknee surgeryunder spinalanesthesia.Forty-eight hoursafter theprocedure,thepatient showed frontal,orthostaticheadachethatimprovedwhenpositionedsupine.Diagnosisofsinusitiswas made inthe generalemergency room,and hereceived symptomatic medication.In subse-quent days, theheadache worsened with holocranial locationand with little improvement inthesupineposition.Thepatient presentedwithleft hemiplegiafollowed bytonic---clonic seizures.Heunderwentmagneticresonancevenography;diagnosedwithCVT.Analysisof pro-coagulantfactorsidentifiedthepresenceoflupusanticoagulantantibody.Thepatientreceived anticonvulsantsandanticoagulantsandwasdischargedontheeighthdaywithoutsequelae.
夽 CETdoHospitaldeClínicasdaUniversidadeFederaldoTriânguloMineiro,Uberaba,MG,Brazil.
∗Correspondingauthor.
E-mail:[email protected](F.M.Bisinotto). http://dx.doi.org/10.1016/j.bjane.2014.09.015
©2015SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Raquianestesia; Complicac¸ões cefaleiapós-punc¸ão dadura-máter; Trombosevenosa cerebral
Trombosevenosacerebralapósraquianestesia:relatodecaso
Resumo
Introduc¸ão:A trombose venosa cerebral (TVC) é uma complicac¸ão rara, mas grave, após raquianestesia.Estáfrequentementerelacionadacomapresenc¸adefatorespredisponentes, como gestac¸ão,puerpério, usodecontraceptivosoraise doenc¸as malignas.Osintomamais frequenteéacefaleia.Descrevemosumcasodeumpacientesubmetidoàraquianestesiaque apresentoucefaleianoperíodopós-operatóriocomplicadacomTVC.
Relatodecaso:Pacientede30anos,ASA1,submetidoàcirurgiadeartroscopiadejoelhosob raquianestesia,semintercorrências.Quarentaeoitohorasapósoprocedimentoapresentou cefaleiafrontal,ortostática,quemelhoravacomodecúbito.Foifeitodiagnósticodesinusite emprontosocorrogeralerecebeumedicac¸ãosintomática.Nosdiassubsequentestevepioria dacefaleia,quepassouaterlocalizac¸ãoholocranianaemaisintensaecompequenamelhora comodecúbitodorsal.Evoluiucomhemiplegiaesquerdaseguidadeconvulsõestônico-clônicas generalizadas.Foi submetidoàressonânciamagnética comvenografiaquefezodiagnóstico deTVC.Apesquisaparafatorespró-coagulantesidentificouapresenc¸adeanticorpolúpico. Recebeucomomedicamentosanticonvulsivanteseanticoagulantesetevealtahospitalarem oitodias,semsequelas.
Discussão: Qualquerpacientequeapresentecefaleiaposturalapósumaraquianestesia,eque intensificaapósumplatô,percasuacaracterísticaortostáticaousetornemuitoprolongada, devesersubmetidoaexamesdeimagemparaexcluircomplicac¸õesmaissériascomoaTVC.A perdadelíquidocefalorraquidianolevaàdilatac¸ãoeàestasevenosa,que,associadasàtrac¸ão provocadapelaposic¸ãoereta,podem,emalgunspacientescomestadosprotrombóticos,levar àTVC.
©2015SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Since the first case reported by August Bier in 1898,1
post-puncture headache has been a problem for patients undergoingduralpuncture.Intheclassicaldescription,the post-duralpunctureheadache(PDPH)hasfrontalor occipi-tallocation,getsworsewithuprightpositionandessentially improvesordisappearswiththesupineposition.Theonset anddurationofPDPHsymptomsmaybeextremelyvariable, butinmostcasestheyoccurwithinthefirst48hafterthe punctureandhave aself-limitingcharacter,lastingonlya fewdays.Insomecases,itmaybeassociatedwithnausea andvomiting.1Variouscauseshavebeenassociatedwiththe
onsetofPDPH,particularlytheneedlegaugeandtipdesign. Butevenwithsmallgaugeneedlesandinexperiencedhands, PDPHstillhasanincidenceof0.16---1.3%.2
Although the classic description of PDPH has a benign course, it does not always have this favorable outcome, as it may be a symptom associated with more severe complications,although rare.Among thesecomplications, cerebral venous thrombosis(CVT) is amajor concernand
canbeadiagnosticchallengewhenassociatedwithlumbar puncture.
The objective of this paper is to report the case of a patientwhopresentedwithaclinicalpictureofCVTafter spinalanesthesiafororthopedicsurgery.
Case
report
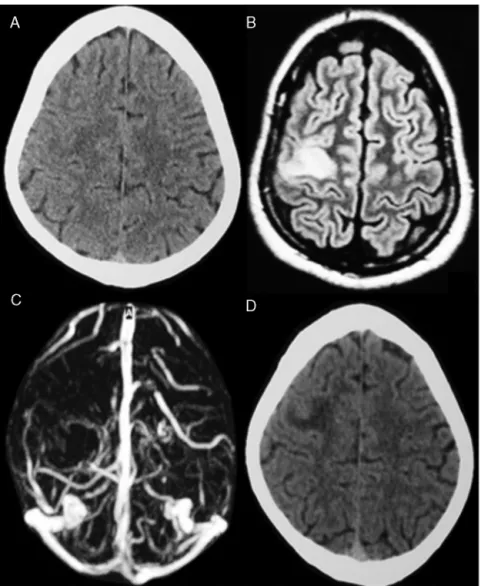
Figure1 Imagingstudyofthecase.A,B,CaretestsperformedonthefirstdayofsymptomsandDisthecontrolexamination
performedafter10 days.A, cranialCTwithoutcontrasttodiscretehypodenseinrightfrontallobe;B,brainMRIFlairshowing
vasogenicedemainthetopographyofthepre-centralgyruslaw;C,MRIangiographydemonstratingacutethrombosisofsuperficial
corticalveinsintherightfrontalconvexity;D,headCTwithoutcontrastwithhypodenseinrightfrontallobe,featuringbetter
definitionofthelesionrelativetotheinitialcranialCT.
(5mg),cefazolin(1g),ondansetron (4mg),dipyrone(2g), andcetroprofeno(100mg).Aftersurgery, thepatientwas takentothepost-anesthesiarecoveryunitandthentothe wardandwasdischargedthesameday.
Forty-eighthoursaftertheprocedure,thepatient devel-opedsevereright frontalheadache,orthostaticinnature, whichimprovedwithrest.Inaperiodof12h,theheadache evolvedtoaholocranialheadache,severityof10onascale of0---10(0=nopainand10=unbearablepain),particularly intheupright position.Inthesupineposition,thepatient stillcomplainedofpain,severityoffiveonthescale men-tionedabove.Inadditiontotheheadache,thepatientalso reportedaclogged earsensation.He sought medicalcare in the emergency department, where he was diagnosed with sinusitis. The patient was treated with antibiotics, anti-inflammatoryandantiallergicdrugs.Onthefourth post-operativeday,thepatienthadparesthesiaintheleftarm, whichevolvedintogradeIIIhemiparesisaroundtheleftside ofthebody.Thenextday(fifthpostoperativeday),hehad
anepisodeofgeneralizedtonic---clonicseizure,received ini-tialcarebytheemergencymedicalsystem(Samu)andwas takentothehospitalwhere,onarrival,hepresentednew generalized convulsive episode, with myoclonus. He was admittedtotheintensivecareunit,wherehewastreated withanticonvulsantsand subjected toimagingtest. Com-putedtomography(CT)oftheheadrevealed asmallright frontalhypodensityandmagnetic resonanceimaging(MRI) withcontrastvenographyshowedvasogenicedema associ-atedwithacutethrombosisofthesuperficialcorticalveinsin therightfrontalconvexity(Fig.1A---C).Withthisdiagnosis, specifictreatmentwasstartedwithfullanticoagulation.
Afterdiagnosisandtreatment,adetailedfamilyhistory revealed thrombotic events. The patient’s father had an episodeofcerebralischemiaandtwouncleshaddeepvein thrombosis.Laboratory testsshowedhyperlipidemia(total cholesterolof331mgdL−1andtriglyceridesof414mgdL−1)
agulantdrugs. After 10days of theictal event, acontrol headCTwasperformed,whichshowedarightfrontal hypo-dense area, better defining the subacute ischemic lesion withregressionoftheedema(Fig.1D).
Three months after the event, the patient reported cyclothymic behavioral changes, with episodes of eupho-riaalternatingwithperiodsofdepression.Nomotordeficit remained.
Discussion
Thenumberofpublishedreviewsreportingthesimultaneous occurrence of PDPH and CVT is limited, which prevents theknowledgeof thetrue incidenceofthis complication. Furthermore, there is the fact that many cases are not reportedorevendiagnosed.GreaterawarenessofCVTfrom casereportslikethiscanhelpincreasetheidentificationof patientsathighriskandearliertreatment.
This paperdescribes acase of CVTafter lumbar punc-turefor spinal anesthesiain apreviously healthy patient. Thedevelopmentofsignsandsymptomsinthesecond post-operativeday,characterizedbyorthostaticheadache,leads tothediagnosisofPDPH.However,twofeaturesdraw atten-tioninthispatient:theheadacheseverityandthelocation changefromfrontaltoholocranial.Theprevioushistoryof sinusitismaskedclinicalsuspicionofothercomplicationand onlytheappearanceofwarningsigns,suchasmotordeficits andseizures,ledtothesuspicionofamoreserious involve-ment.
Our patient had no predisposing conditions that could helpinthediagnosisofCVT.Thisisarareconditionwith mul-tiplecausesorriskfactors,suchasuseoforalcontraceptives andotherdrugs,infections,malignantandinflammatory dis-eases,postpartumperiod,andcongenitalthrombophilia.3,4
Few cases of CVT have been described after post-dural puncture for spinal or epiduralanesthesia,5 myelography,
intrathecaladministrationofdrugsorrelatedtodiagnosis.6
CasesofCVTafterregionalanesthesiareportedinthe liter-aturearerareandusuallyassociatedwiththepostpartum period.6
Of course, there is a dilemma for the physician who attendsapatientwithaheadacheaftera spinal anesthe-sia,asundoubtedlythefirstdiagnosiswillbePDPH.Inthis case,wecanmentionasacomplicatingfactorthe overlap-pingofanotherdiagnosis,ofsinusitis,asthecausalfactor oftheheadache,althoughacutesinusitisisan uncommon causeofheadachewiththemanifestedcharacteristics.7
CVT has a wide and remarkable semiological variety. Continuousheadacherelatedtothestandingposition, dizzi-ness,nausea,vomiting,blurredvision,motorsigns,seizures, reduced mental awareness, and coma may be present. Headacheisthemostcommonsymptom8,9andcansimulate
the PDPH itself,10 cerebral hemorrhage, or migraine-type
headache.11,12 The specific presentation depends on the
location and extent of thrombosis, degree of collateral venouscirculationaroundthrombosis,andpresenceof corti-callesionsassociated.13Thrombosisofasinglecorticalvein
coma. Furthermore,signsandsymptomsmaybe intermit-tentwhenthrombosisandfibrinolysisoccursimultaneously, leadingtofluctuationsinthecirculationaroundthe throm-bosedvesselsandintracranialpressure.14
Inepidemiologicalterms,CVTismorecommoninwomen, agedbetween20and35 years,andit seemsthatthereis noethnicpredominance.Itiswidelyacceptedthatthe fre-quencyofCVTismuchhigherinpregnantwomen,compared tothegeneralpopulation,andaccountsfor34%ofreported casesintheliterature.14Usually,ithasanacuteonset
dur-ingpregnancyandinmostcasesitoccursinthepostpartum period.When relatedto thepostpartum period,CVTmay havean acuteor longeronset.Thevenous congestionand damage to the vascular endothelium, which may be sec-ondary tolabor and expulsion period,combinedwith the typical state of postpartum hypercoagulability could con-tributetotheincreasedriskafterbirth.15---17
Althoughithasprevalenceinpregnantwomen,CVTcan alsoaffect otherpatients.In areviewby Maheshetal.,18
52casesofCVTthatoccurredafterlumbarpuncturewere analyzed.Thecaseswereallocatedintoagroupofobstetric patients(34.06%ofcases),asecondgroupofpatientswho underwent diagnosticlumbar puncture, anda third group ofpatients whounderwentthepuncturefor anesthesiaor injectionofdrugs.Intheobstetricpatients,72.2%had pos-tural headache as the first symptom and changes in the headachepatternwereseeninabout50%ofpatients.Most of themhad prothromboticpredispositionorprevious his-toryoforalcontraceptiveuse.Patientsinbothnon-obstetric groupshadposturalheadacheinalmost100%ofcases,with standard changein77%ofthegroupthatunderwent diag-nosticlumbarpunctureandin40%ofthosewhounderwent thepunctureforanesthesiaorinjectionofdrugs. Demyeli-natingdiseaseswereseenin82%ofthegroupwithdiagnostic lumbarpunctureandprothromboticstatusin66%ofpatients undergoinganesthesia.
Since the first description of the association between lumbar puncture andCVT bySchou and Scherb19 in 1986,
there has been a constant debate of the causal relation-shipbetweenlumbarpunctureandCVT:whetherthereisan associationoramerecoincidencebetweenthetwoevents. However,overthepasttwodecades,thereisgoodevidence to suggest causality, according to which lumbar puncture alone can trigger CVT.20 Nevertheless, in most reported
cases,thereareotherriskfactorsforCVTthatputsindoubt the trueuniqueroleof lumbarpuncture inthe genesis of CVT.
in the venous compartment, at the expenseof stasis and dilationoftheduralvenoussinusesandcorticalveins.This changeoccurssharplyintoughfibrousmeninx(duramater), andasithasnoblood-brainbarrier,suchfactwouldexplain the contrast agent extravasation on a diagnostic imaging test.19WiththereducedCSFvolume,therewillbearelative
declineandtractionofthebrainasawhole,togetherwith the distortion and elongation of dural and cortical veins. Thesechangeswilleventuallydamagethevascularwall.All thesechangesareaggravatedbythestandingpositiondue toacutedilationof theveins,aswellasthestretchingof itswalls.19ThedescribedphenomenonmeetstheVirchow’s
theory,accordingtowhichthethreemaincausesfor throm-bosis occurrencewould beblood stasisand thechange in thevesselwallandbloodcomposition.19,20
Suchpathophysiologicalphenomenadescribedaboveend up creating a vicious cycle because thrombosis of corti-cal veins or superior sagittal sinus leads to a decrease in venous drainage, which reduces the absorption of CSF byarachnoidvilli,furtherincreasingtheintracranial pres-sure. Simultaneously, venous stasis leads to blood stasis andfocalcerebralinfarction.Thistriggerssignsand symp-toms suchassevereheadache,nausea,focal neurological signs,seizures,andalteredconsciousness.The occurrence of subdural hematoma and intracranial hemorrhage after lumbarpunctureisrelatedtothesamepathophysiological mechanism.2,21
TheCSFvolumeescapingthroughtheholemadebythe punctureneedleis responsibleforsecondaryvenodilation. However,thisdilationisnotdirectlycorrelatedwiththe vol-ume lost. In this context, Grant et al.,22 in a study with
magneticresonance,showedthatevensmallvolumesofCSF (about1.8mL)thatarelostafteralumbarpunctureare suf-ficienttoleadtoPDPH.Moreover,Ghalebetal.23 reported
thatalossof10%oftheCSFvolumecantriggerheadache. Toreinforcethehypothesisoftherelationshipbetween lumbar puncture and the occurrence of cerebral throm-bosis, Canhão etal.20 used thetranscranialDoppler in 13
patientsandrecordedthemeanbloodflowvelocityinthe straightsinusbefore,during,andafteralumbarpuncture. Thestudydemonstratedareductioninbloodflowvelocity of approximately 50% in the straight sinus after the lum-barpuncture. This reductionin blood flow velocitywould besecondary to reducedintracranial pressureinduced by decreasedCSF.20
It is well accepted that multiple risk factors are often seen in the same patient with CVT. Indeed, it has been demonstrated in the literature the association with malignancy,thrombophilia, postpartum status,use oforal contraceptives,andintrathecalinjectionofsteroidsor cyto-statics.Insuchpatients,lumbarpuncturehasbeen oneof theprecipitatingfactorsofCVTbythemechanismdescribed byCanhãoetal.24 Consequently,facedwithacaseofCVT
afterlumbarpuncture,otherriskfactorsforvenous throm-bosis should be investigated,as diagnosed in the patient describedherein,aprothromboticstatusbythelupus anti-bodypresence.
Neuroimagingstudiesareneededtoconfirmthediagnosis ofCVT. Computedtomography closesthediagnosisinonly 30%ofcases.11Magneticresonanceimagingassociatedwith
venographyisthegoldstandardmethodforfinaldiagnosis, withsensitivitycloseto100%.24
CVT treatment is primarily non-invasive, although endovascularthrombolysis andsurgical thrombectomy are consideredinseverecases.25,26Anticoagulationisthe
treat-ment of choice, but the indications for its use remain somewhatcontroversial,asapproximately50%ofcasesare associatedwithhemorrhagiccerebralinfarction.27
Asfortheprognosis,theclinicalcourseofCVTis unpre-dictable and often there is worseningof symptoms after thediagnosis.Changesinconsciousness,coma,and intracra-nialhemorrhageareimportantpredictorsofadverseclinical course.28
Thus, we concluded that major complications after regionalanesthesiaarerare,butcanbedevastatingtothe anesthesiologist, and especially to the patient. Although mostcases of PDPHevolve satisfactorily, itshould notbe neglected,asinthecaseofCVT,suchsemiologicalfindingis presentinabout90%ofcasesandmaybetheonly manifesta-tionin10%.Atsuchtimes,thereisaconsiderablepotential formorbidityandevendeath.Therefore,attentionmustbe paidwhentheheadachechangesitsposturalcharacteristic andwhenthepatienthasriskfactorsforvenousthrombosis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Davignon KR, Dennehy KC. Update on postdural puncture headache.IntAnesthesiolClin.2002;40:89---102.
2.Turnbull DK, Shepherd DB. Post-dural puncture headache: pathogenesis, prevention, and treatment. Br J Anaesth. 2003;91:718---29.
3.KarciaA,BoyaciF,YakaE,etal.Cerebralvenousthrombosis initiallyconsideredasacomplicationofspinal-epidural anaes-thesia.JIntMedRes.2005;33:711---4.
4.BarrettJ,AlvesE.Postpartumcerebralvenoussinusthrombosis afterduralpunctureandepiduralbloodpatch.JEmergMed. 2005;28:341---2.
5.KayimYO,BalabanH,CilG,etal.Isolatedcorticalvein throm-bosis after epidural anesthesia:report of threecases. IntJ Neurosci.2010;120:447---50.
6.Ferrante E, Spreafico C, Regna-Gladin C, et al. Cerebral venousthrombosis complicatinglumbarpuncture.Headache. 2009;49:276---7.
7.MarmuraMJ,Silberstein SD. Headachescaused bynasal and paranasalsinusdisease.NeurolClin.2012;32:507---23. 8.StamJ.Thrombosisofthecerebralveinsandsinuses.NEnglJ
Med.2005;352:1791---8.
9.TimóteoA,InácioN,MachadoS,etal.Headacheasthesole pre-sentationofcerebralvenousthrombosis:aprospectivestudy.J HeadachePain.2012;13:487---90.
10.CanOS,YilmazAA,GurcanE,etal.Ispost-partumheadache afterepiduralanaesthesiaalwaysinnocent?EurJAnaesthesiol. 2008;25:697---700.
11.BousserMG.Cerebralvenousthrombosis:diagnosis and man-agement.JNeurol.2000;247:252---8.
12.TodorovL,LauritoCE,SchwartzDE.Posturalheadacheinthe presence ofcerebralvenoussinus thrombosis.AnesthAnalg. 2005;101:1499---500.
venousthrombosis.AustNZJMed.1984;14:643---8.
17.LamyC,SharsharT,MasJL.Cerebrovasculardiseasesin puer-perium.RevNeurol.1996;152:422---40.
18.MaheshPK,ThomasB,SylajaPN.Cerebralvenousthrombosis inpost-lumbarpunctureintracranialhypotension:casereport andreviewofliterature.F1000Res.2014;3:41---6.
19.SchouJ,ScherbM.Postoperativesagittalsinusthrombosisafter spinalanesthesia.AnesthAnalg.1986;65:541---2.
20.CanhaoP,BatistaP,FalcaoF.Lumbarpunctureandduralsinus thrombosis---acausal orcasualassociation?CerebrovascDis. 2005;19:53---6.
21.Zeidan A, Farhat O, Maaliki H, et al. Does postdural punc-ture headache left untreated lead to subdural hematoma? Casereportandreviewoftheliterature.IntJObstetAnesth. 2006;15:50---8.
headache.IntJGenMed.2012;5:45---51.
24.ConnorSEJ,JaroszJM.Magneticresonanceimagingofcerebral venoussinusthrombosis.ClinRadiol.2002;57:449---61. 25.PhilipsMF,BagleyLJ,SinsonGP,etal.Endovascular
thrombo-lysisforsymptomaticcerebralvenousthrombosis.JNeurosurg. 1999;90:65---71.
26.WeatherbySJ,EdwardsNC,WestR,etal.Goodoutcomeinearly pregnancy following direct thrombolysis for cerebral venous sinusthrombosis.JNeurol.2003;250:1372---3.
27.BruijnSF,StamJ.Randomized,placebo-controlledtrialof anti-coagulant treatment with low-molecular-weight heparin for cerebralsinusthrombosis.Stroke.1999;30:484---8.