REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Epidemiological
profile
of
patients
seen
in
the
pre-anesthetic
assessment
clinic
of
a
university
hospital
Monica
Loureiro
Santos
a,b,∗,
Cristiane
de
Oliveira
Novaes
c,
Antonio
Carlos
Iglesias
d,eaUniversidadeFederaldoEstadodoRiodeJaneiro(Unirio),SaúdeeTecnologianoEspac¸oHospitalar,RiodeJaneiro,RJ,Brazil bUniversidadeFederaldoEstadodoRiodeJaneiro(Unirio),HospitalUniversitárioGaffréeeGuinle,Servic¸odeAnestesiologia,
RiodeJaneiro,RJ,Brazil
cUniversidadeFederaldoEstadodoRiodeJaneiro(Unirio),InstitutodeSaúdeColetiva,RiodeJaneiro,RJ,Brazil
dUniversidadeFederaldoEstadodoRiodeJaneiro(Unirio),EscoladeMedicinaeCirurgia,DepartamentodeCirurgiaGerale
Especializada,RiodeJaneiro,RJ,Brazil
eUniversidadeFederaldoEstadodoRiodeJaneiro(Unirio),HospitalUniversitárioGaffréeeGuinle,Servic¸odeCirurgiaGerale
CirurgiadoAparelhoDigestivo,RiodeJaneiro,RJ,Brazil
Received7November2015;accepted27June2016 Availableonline26April2017
KEYWORDS
Preanesthetic evaluation; Surgery;
Preoperativecare
Abstract
Objective: Assessthedemographicandclinicalcharacteristicsofsurgicalpatientsseeninthe
Pre-anestheticAssessmentClinicoftheHospitalUniversitárioGaffréeeGuinle(APA/HUGG),in ordertoassistinthepursuitforquality,effectiveness,andresourcerationalizationofhospital management.
Method: Cross-sectional descriptive study with 491 patients undergoing elective surgery,
treated at APA/HUGG Clinic from March to December 2014. The following variables were assessed:sex,age,BMI,smokingstatus,associateddiseases,classificationofMET’sandASA, presenceofdecompensateddisease,medicalassociatedappointmentsinterconsultation, spe-cialtyandsurgicalrisk,historyofprioranesthetic-surgicalprocedure,andcomplications.
Results:Therewasapredominanceoffemale(64.8%)andoverweightpatients(55.9%),aged
18---59years.Theprevalenceofassociateddiseaseswashigh(71.3%),withhypertensionpressure prevailing(50.1%).Mostpatientshadclinicallycompensatedmorbidity(96.3%)andlong-term useofmedication(77.4%).Regardingthesurgicalcharacteristics,themostfrequentspecialty wasgeneralandmediumrisksurgeries.Theanalysisofthecharacteristicsbyageshowedthat the elderlyhavemore associated diseases andlong-termuse ofmedication, inaddition to predominanceofASAII---III.
∗Correspondingauthor.
E-mail:[email protected](M.L.Santos). http://dx.doi.org/10.1016/j.bjane.2017.04.006
Conclusion:TheepidemiologicalprofileofsurgicalpatientsseenattheAPA/HUGGwasfemale, age18---59years,overweight,withassociateddiseases,long-termuseofmedication,without clinical decompensation, ASA II andMET’s ≥4. Knowledge of theclinical characteristicsof surgicalpatientsiscriticaltoscheduletheperioperativecare,allowingtheimprovementof qualityandsafetyinanesthesiaandsurgery.
©2016SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Avaliac¸ão pré-anestésica; Cirurgia; Cuidados pré-operatórios
Perfilepidemiológicodepacientesatendidosnoambulatóriodeavaliac¸ão pré-anestésicadeumhospitaluniversitário
Resumo
Objetivo:Verificar ascaracterísticas demográficase clínicas dos pacientes cirúrgicos
aten-didosnoAmbulatóriodeAvaliac¸ãoPré-AnestésicadoHospitalUniversitárioGaffréeeGuinle (APA/HUGG),comoobjetivodeauxiliarnabuscadequalidade,efetividadeeracionalizac¸ão derecursosdagestãohospitalar.
Método: Estudodescritivotransversal,feitocom491pacientesdeoperac¸ãoeletiva,atendidos
noAmbulatóriodeAPA/HUGGdemarc¸oadezembro de2014. Foramestudadasasvariáveis: sexo,faixaetária,índicedemassacorporal(IMC),tabagismo,doenc¸asassociadas,classificac¸ão dacapacidadefuncional(METs),(ASA),doenc¸adescompensada,interconsultas,especialidadee portecirúrgicos,históriadeprocedimentoanestésico-cirúrgicoprévioepossíveiscomplicac¸ões.
Resultados: Predominarampacientesdosexofeminino(64,8%),nafaixade18a59anos(55,9%)
ecom sobrepeso(38,3%). A prevalênciade doenc¸as associadas foielevada (71,3%)sendoa hipertensãoarterialaprincipal(50,1%).Amaiorparceladospacientesapresentavamorbidade clinicamentecompensada(96,3%)eusocontínuodemedicamento(77,4%).Emrelac¸ãoàs car-acterísticascirúrgicas,aespecialidademaisfrequentefoiacirurgiageraleoportemédio.A análisedascaracterísticasporfaixaetáriamostrouqueosidososapresentarammaisdoenc¸as associadaseusocontínuodemedicac¸ãoalémdepredomíniodeASAIIeIII.
Conclusão:OperfilepidemiológicodospacientescirúrgicosatendidosnaAPA/HUGGfoi:sexo
feminino,faixaetáriade18a59anos,sobrepeso,comdoenc¸asassociadas,emusodemedicac¸ão contínua,semdescompensac¸ãoclínica,ASAIIeMETs≥ 4.Oconhecimentodascaracterísticas clínicasdospacientescirúrgicoséfundamentalpara oplanejamentodoscuidados perioper-atóriosepermiteavanc¸arnaqualidadeeseguranc¸aemanestesiaecirurgia.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Since the last decades of the twentieth century, the qualityofservices andhealth systemshas becomea cen-tral and common theme throughout world. Quality and safety form a binomial that should guide improvements in structures, outcomes, and processes.1 Pre-anesthetic
evaluation(PAE)isinsertedinthiscontextasa fundamen-tal aspect to increase the anesthetic-surgical safety and qualityofcare.Inadequateand/orinsufficientPAEis asso-ciated with increased surgical morbidity and mortality.2
However, when performed on an outpatient basis, it has manyadvantages,suchasimprovementofpatient’sclinical status, reduced anxiety, and faster postoperative recov-ery in addition to increased contact of the patient with the anesthesiologist.3---5 The Brazilian Federal Council of
Medicine (Conselho Federal de Medicina --- CFM) through the Resolution 1.802/06.1 declared the pre-anesthetic
evaluation asessential, and recommended itscompletion beforehospitaladmission.6
PAE is defined as a set of measures that precede the anestheticcare requiredfor theoperation andconsistsof collecting and recording information through interviews, medicalhistory,physicalexamination,laboratorytests,and evaluations by medical specialists. Its objectives are to identifyassociateddiseases,evaluatedrugtherapy, deter-mine the need for perioperative interventions, formulate the anesthesia plan (choice of drugs, intraoperative or postoperativemonitoring),andestablishmeasurestoguide intraoperative decisions.7,8 Moreover, it is the time to
obtainconsentandprovideinformationandguidancetothe patient.9,10
preoperativecareexpandedoutoftheoperatingroomand thus expandedtheroleoftheanesthesiologist asan eval-uator of these procedures. The outpatient preoperative clinicalvisitmadebytheanesthesiologistisarelativelynew model,sothattheconceptofapre-anestheticassessment clinicwasinitiallyintroducedjustover 50years11 andhas
beengraduallyimplementedinBrazil.
Knowledge of the demographic and clinical character-isticsof thepopulation candidatefor surgical procedures of a hospital is critical to business planning and physical dimensionoftheoperatingtheaterandcaresystems,such as admission/discharge and day hospital. It also helps in multidisciplinary effort, education and training of human resources, and in the operation of support sectors, such as laboratory,transfusional agency, and pharmacy. It is a veryusefultoolinthesearchforsafety,quality, effective-ness,andstreamliningofhospitalmanagementresources. Theaimofthisstudywastodeterminethedemographicand clinicalcharacteristicsofsurgicalpatientsseenatthe Pre-anesthetic Assessment Clinic of the Hospital Universitário GaffréeeGuinle(HUGG).
Methods
Descriptive,cross-sectionalstudyperformedfromMarchto December 2014. It was approved by the Research Ethics Committee,No27505514.4.0000.5258,andallpatientswho agreedtoparticipategaveWrittenInformedConsent(WIC). Thestudypopulationconsistedofpatientswithsurgical diseases of elective treatment, referred for preopera-tive evaluation by the following clinics: general surgery, digestive tract surgery, and colon surgery and proctol-ogy (specialties that in this study comprised the general surgerygroup),urology,gynecology,thoracicsurgery, vascu-larsurgery,otorhinolaryngology,orthopedics,neurosurgery, plasticsurgery,andophthalmology.Exclusioncriteriawere patients aged under 18 years and absence or failure to complete the evaluation form. Pre-anesthetic consulta-tionfollowedtheguidelinesforambulatoryanesthesiaand surgeryapprovedbytheAmericanSocietyof Anesthesiolo-gists(ASA).12Datawerecollectedbytheresearcher,through
a data collection form, who collected information from interview and physical examination registered in individ-ualpre-anestheticevaluationforms(aformdevelopedand usedbytheDepartmentof Anesthesiology[SANE/HUGG]). PAEconsultationsweremadebythreeSANE-HUGG anesthe-siologists.
Thefollowinggroupsofvariableswereconsidered:
1. Demographic and anthropometric variables: Sex; age stratified in two groups (18---59 years and ≥60 years); weight and height used to calculate body mass index (BMI).13
2. Clinical variables: Presence of one or more associ-ated diseases identified by history and/or physical examination and identified by history and/or physical examinationandtheirquantitative;historyofsmoking; use of medications; functional classification according to metabolic equivalents --- MET (Duke Activity Sta-tusIndex),DukeActivityStatusIndex,14physical status
ASA,15needforreferraltospecialistaccordingtoclinical
criteria,andtheoccurrenceofclinicallydecompensated associateddisease.
3. Surgicalprocedurevariables:Surgicalspecialty,surgery classificationproposedbyEagle,16andprevioushistoryof
surgeryand/oranesthesiaandpossiblecomplications.
For sample size calculation, we obtained the histori-calaverage numberofpatientsseen inthePre-anesthetic Assessment Clinic of HUGG. We use the calculation for finite population samples and sampling procedures with-out replacement and obtained a sample of 329, which ensuresa95%confidenceintervalandasignificancelevelof
p≤0.05.TheSPSSsoftwareversion17.0forWindows (Statis-ticPackageforSocialSciences,Chicago,IL,USA)wasused fordata processingthroughdescriptivestatistics; qualita-tivevariablesaredescribedaspercentagesandcontinuous variablesasmeanandstandarddeviation.Tocheckthe dis-tributionofcharacteristicsbyagegroupandsexweusedthe chi-squaretest (95%confidence intervalanda p≤0.05 as significant).
Results
Weanalyzed491patients intotal.Ofthe500consecutive patientsinitially recruited, sixrefused to participateand threedidnotmeetthestudycriteria.
Therewasapredominance of female(64.8%);meanof 56.12±15.3 years (18---90 years); 55.9% of patients were assignedtothe group of upto59 years. Ofthe patients, 67.2%wereoverweight,with38.3%intheoverweightgroup and28.9%intheobesegroup(gradeI,II,andIII),shownin
Table1.
Associated diseases were identified in most patients (71.3%),and theassociation of twoor more diseases was identifiedin32% ofthe sample. Themost prevalent asso-ciated disease was systemic arterial hypertension (SAH), whichaffectedhalfofthepatients(50.1%),followedby dia-betesmellitus(11.4%),lungdisease(9.5%),anddyslipidemia (7,9%).Regardinglifehabits,11%ofpatientsweresmokers. Thecontinueduseofmedicationwasseenin77.4%.Among the most commonly used drugs, angiotensin-converting enzyme(ACE)inhibitorsandangiotensinIIreceptor block-ers(ARBs)wereusedby36.9% ofpatients,whereas25.5% useddiuretics and11.2% other antihypertensivedrugs ( -blockers,Ca+channelblockers,etc.).Thesegroupsofdrugs
werefollowedbyoralorinjectableantidiabeticagentsused by14.9%,corticosteroids by5.3%,immunosuppressantand chemotherapyagentsby 1.6%,andanticoagulantsby1.4% ofthesample(Table1).
Accordingtothefunctionalclassificationused,65.6%of thesamplewereclassifiedwithmoderatefunctional capac-ity(MET≥4);22.4%withexcellentcapacity(MET≥10),and 12%withlowcapacity(MET<4).Regardingthephysical sta-tusclassificationproposedbyASA,64.4% ofpatientswere classifiedasASA II.Referral tospecialistswasrequired in 6.7%ofpatients,withpredominanceofcardiology.Only3.7% ofpatients hadaclinically decompensateddiseaseduring
PAE(Table1).
Table 1 Demographic, anthropometric, and clinical variables.
Variable n %
Sex
Female 316 64.4
Male 175 35.6
Age
18---59years 275 56
≥60years 216 44
Bodymassindex
Underweight 11 2.2
Eutrophic 150 30.5
Overweight 188 38.3
ObesitygradeI,IIandIII 142 28.9
Associateddiseases
Yes 350 71.3
No 141 28.7
Twoormoreassociated 157 32
SAH 246 50.1
DM 56 11.4
Smoker
Yes 54 11
No 437 89
Useofdrugs
Yes 380 77.4
No 111 22.6
Functionalclassification(MET)
<4METs 59 12
≥4METs 322 65.6
≥10METs 110 22.4
Physicalstatus(ASA)
ASAI 131 26.7
ASAII 316 64.4
ASAIII 44 9
Needforreferral
Yes 33 6.7
No 458 98.3
Decompensateddisease
Yes 18 3.7
No 473 96.3
Total 491 100
SAH,SystemicArterialHypertension;DM,diabetesmellitus.
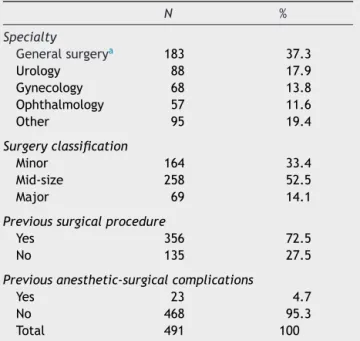
(13.8%); about half of operations were medium-sized (52.5%).Mostpatients(72.7%)hadaprevioushistoryof sur-gicalinterventionsandonly 4.7%reportedtheoccurrence ofcomplicationsinanesthetic-surgicalprocedures.
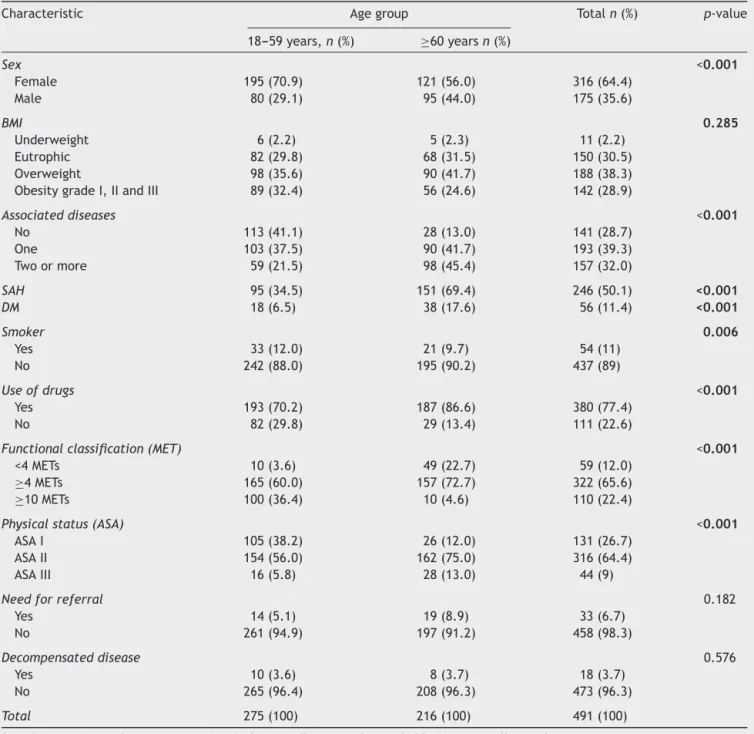
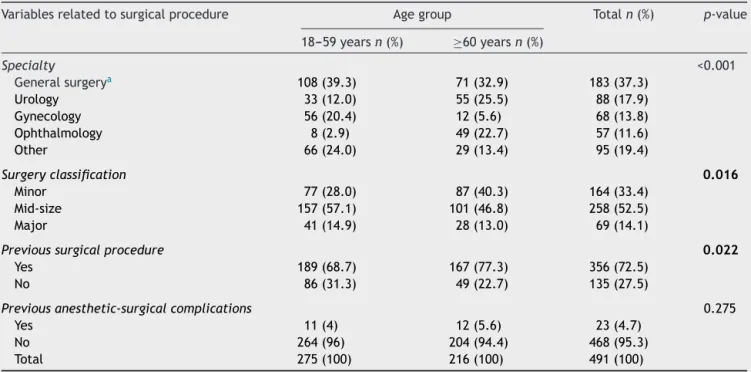
Tables 3 and 4 showthe distribution of characteristics
byagegroup,whoseanalysiswasperformedusingthe chi-squaretest andadoptingasignificance levelof p ≤0.05. Therewere significant differences for sex, withthe high-estconcentrationofwomenintheoldergroup(p<0.001); therewaspredominanceofassociateddiseasesintheolder group (p<0.001), as well as smokers (p=0.006), use of medication (p<0.001), MET (p<0.001), ASA (p<0.001),
Table2 Variablesrelatedtosurgicalprocedure.
N %
Specialty
Generalsurgerya 183 37.3
Urology 88 17.9
Gynecology 68 13.8
Ophthalmology 57 11.6
Other 95 19.4
Surgeryclassification
Minor 164 33.4
Mid-size 258 52.5
Major 69 14.1
Previoussurgicalprocedure
Yes 356 72.5
No 135 27.5
Previousanesthetic-surgicalcomplications
Yes 23 4.7
No 468 95.3
Total 491 100
a General surgery comprises surgical procedures general
surgery,abdominalsurgery,andcoloproctology.
surgicalspecialty(p<0.001),sizeofsurgery(p=0.016),and previoussurgicalprocedure(p=0.022).Tables5and6show thedistributionofcharacteristicsbysex.Therewasa pre-dominance of women in theobesity group (p=0.007) and in continuoususeof medication (p=0.013);menwas pre-dominant in the smoker group (p<0.001) and also in the functional classification MET ≥10 (p<0.001). There were alsosignificantdifferencesbetweensexesindistributionby surgicalspecialty(p<0.001),withpredominanceoffemale ingynecologyandophthalmologyspecialtiesandmale pre-dominanceinurology,inadditiontofemalepredominance in previous history of surgical procedures (p=0.039) and anesthetic-surgicalcomplications(p=0.045).
Discussion
Theprimaryobjectivesofthepre-anestheticevaluationare topromotesafetyinsurgeryandanesthesiabyreducing sur-gical morbidity and mortality, in addition to improve the qualityofcareandreduceperioperativecarecosts.Studies performedinAustralia2,17 reportedthat14%of
anesthetic-surgical complications and 39% of deaths attributed to anesthesiawereunequivocallyassociatedwithinsufficient and/orinadequatepreoperativeevaluation.
In our country there is a strong trend toward PAE expansioninoutpatientsettings,althoughtherearestill dif-ficultiesintheimplementationoftheseservicesevenwith evidenceofimprovedqualityofcare,reducedmorbidityand mortality,andimprovementinperformanceindicators.18---20
Table3 Distributionofanthropometricandclinicalcharacteristicsbyagegroup.
Characteristic Agegroup Totaln(%) p-value
18---59years,n(%) ≥60yearsn(%)
Sex <0.001
Female 195(70.9) 121(56.0) 316(64.4)
Male 80(29.1) 95(44.0) 175(35.6)
BMI 0.285
Underweight 6(2.2) 5(2.3) 11(2.2)
Eutrophic 82(29.8) 68(31.5) 150(30.5)
Overweight 98(35.6) 90(41.7) 188(38.3)
ObesitygradeI,IIandIII 89(32.4) 56(24.6) 142(28.9)
Associateddiseases <0.001
No 113(41.1) 28(13.0) 141(28.7)
One 103(37.5) 90(41.7) 193(39.3)
Twoormore 59(21.5) 98(45.4) 157(32.0)
SAH 95(34.5) 151(69.4) 246(50.1) <0.001
DM 18(6.5) 38(17.6) 56(11.4) <0.001
Smoker 0.006
Yes 33(12.0) 21(9.7) 54(11)
No 242(88.0) 195(90.2) 437(89)
Useofdrugs <0.001
Yes 193(70.2) 187(86.6) 380(77.4)
No 82(29.8) 29(13.4) 111(22.6)
Functionalclassification(MET) <0.001
<4METs 10(3.6) 49(22.7) 59(12.0)
≥4METs 165(60.0) 157(72.7) 322(65.6)
≥10METs 100(36.4) 10(4.6) 110(22.4)
Physicalstatus(ASA) <0.001
ASAI 105(38.2) 26(12.0) 131(26.7)
ASAII 154(56.0) 162(75.0) 316(64.4)
ASAIII 16(5.8) 28(13.0) 44(9)
Needforreferral 0.182
Yes 14(5.1) 19(8.9) 33(6.7)
No 261(94.9) 197(91.2) 458(98.3)
Decompensateddisease 0.576
Yes 10(3.6) 8(3.7) 18(3.7)
No 265(96.4) 208(96.3) 473(96.3)
Total 275(100) 216(100) 491(100)
SAH,SystemicArterialHypertension;DM,DiabetesMellitus.Numbersinboldarestatisticallysignificant.
Thepredominanceofwomen(65%)inthissampleis sim-ilartothat seenin thecountryaccording totheBrazilian InstituteofGeographyandStatistics(IBGE)censusof2010.21
The explanationliesinthe largestBrazilian women popu-lation,quantitatively, in additiontothe predominance of womenintheolderagegroup.Thisfeaturerepresentsthe so called feminization of aging process,22 a configuration
explained by the fact that male mortality is higher than female,aswellasbytheincreaseddemandanduseofhealth servicesbywomen.23
Althoughmost patientswereintheagegroupof18---59 years(55.9%),similartothatfoundinthestudybyGusman18
conductedina universityhospitalofBotucatu(SãoPaulo,
Brazil),itshouldbenotedthatolderpatientshaveachieved asignificant rate inthe sample studied (44.1%).This fact expresseswhathasbeenobservedinrecentdecadesinthe country; that is, the progressive reduction of population growth and changes in the age group structure demon-strated, among other facts, due to the increased elderly population.Thispopulationagingprocessidentifiedbya nar-rowbaseandabroadtopoftheagepyramidisconfirmedby thelastpopulationcensusof2010.21 Thisimpliestheneed
fortrainedhealthprofessionalsandinstitutionstocarefor thisgrowinggroupofpatients.
Table4 Variablesrelatedtosurgicalprocedureclassifiedaccordingtoagegroups.
Variablesrelatedtosurgicalprocedure Agegroup Totaln(%) p-value
18---59yearsn(%) ≥60yearsn(%)
Specialty <0.001
Generalsurgerya 108(39.3) 71(32.9) 183(37.3)
Urology 33(12.0) 55(25.5) 88(17.9)
Gynecology 56(20.4) 12(5.6) 68(13.8)
Ophthalmology 8(2.9) 49(22.7) 57(11.6)
Other 66(24.0) 29(13.4) 95(19.4)
Surgeryclassification 0.016
Minor 77(28.0) 87(40.3) 164(33.4)
Mid-size 157(57.1) 101(46.8) 258(52.5)
Major 41(14.9) 28(13.0) 69(14.1)
Previoussurgicalprocedure 0.022
Yes 189(68.7) 167(77.3) 356(72.5)
No 86(31.3) 49(22.7) 135(27.5)
Previousanesthetic-surgicalcomplications 0.275
Yes 11(4) 12(5.6) 23(4.7)
No 264(96) 204(94.4) 468(95.3)
Total 275(100) 216(100) 491(100)
aGeneralsurgerycomprisessurgicalproceduresgeneralsurgery,abdominalsurgery,andcoloproctology.
Numbersinboldarestatisticallysignificant.
tochronicnon-communicablediseasesinsteadofinfectious andparasiticdiseases.Theincreasingprevalenceofchronic diseasebrings withitthe need for continuoustreatments andincreasedoccurrenceofvaryingdegreesofdysfunction andaddiction,whichhasdirectimplicationsforthesurgical patientmanagement.Thisfactisofsignificantrelevanceto thesocialdemandsandpublicspendingonhealth,with sig-nificantrelevancetotrendsincountriesinmoreadvanced stagesofthedemographictransition.Therefore,aresearch agendainhospitalcare,qualityofcare,andhealthexpenses should seek appropriate hospital infrastructure to absorb thispopulation change, considering the need for physical facilitiesandthetrainingandallocationofhumanresources basedonthecomplexityoftheproblemsandagegroupthat tendstoprevailinthecomingdecades.
TheBMIassessmentallowedtheidentification ofa pre-dominant group classified asoverweight (35%) and obese (28.9%), with predominance of women in these groups, whichissimilarinparttothatreportedintheassessmentby theIBGE,24 inwhichoverweight(BMI≥25kgm−2)was
diag-nosedin 50% of menand 48%of women and obesity(BMI
≥30kgm−2)in12.5%ofmenand16.9%ofwomen.The
fre-quencyofbothoverweightandobesityincreasedintheage groupof45---54yearsformenand55---64yearsforwomen, decliningfromthere,different fromthatobserved inthis studyinwhichtherewasnostatisticaldifferenceregarding BMIassessmentbyagegroup.Similarfindingswerereported by VigitelBrazil in 2013 (Vigilânciade fatores derisco e protec¸ãoparadoenc¸ascrônicasporinquéritotelefônico25);
soin that the comparisonof the lastIBGE24 surveys, the
frequencyofoverweightindividualsincreasedbymorethan
onepercentagepointperyear,whichpointstowardthe pos-sibilitythatinabout10yearstheexcessweightmayreach twothirdsoftheadultpopulationinBrazil.
Obesity is a major public health problem worldwide, withan increasingtrendinrecentyears.This condition is associatedwithincreasedmortalityandoneofthe compli-catingfactorsinthecontrolofchronic,non-communicable diseases (NCDs), particularly cardiovascular and diabetes, veryprevalentconditionsinsurgicalpatients.Moreover,it isknownthatobesityisamajorriskfactorforpostoperative complications,particularlyrespiratoryandinfectious.26This
findingimpliestheneedforamultidisciplinaryapproachfor disorder identification andmonitoring before,during,and aftersurgery,inordertominimizetheadverseconsequences thatmayoccurtothisspecificgroupofpatients.
Inthisstudy,71.3%ofthepatientshadanassociated dis-ease,and32%ofthetotalsamplehadtwoormore.Among themoreprevalentonesthereishypertension,inhalfofthe cases,anddiabetesmellituswithonlythesetwoconditions accountingfor61.5%oftheassociatedchronicdiseases.The prevalenceof associateddiseaseswashigherinolder sub-jects,asdiscussedabove,butwithnostatisticaldifference bysex. NCDsarecurrentlyoneofthemajorpublichealth problems,andestimatesfromtheWorldHealthOrganization (WHO)indicatethatNCDs accountedfor 63%of36million deaths worldwide in 2008.29 Historical series of mortality
statistics available for the capitalsof the Brazilian states indicatethattheproportionofdeathsfromNCDsincreased bymorethanthree-foldsbetween1930and2006.24
The 2013 National HealthSurvey27 indicates thatNCDs
Table5 Distributionofanthropometricandclinicalcharacteristicsbysex.
Characteristics Sex Totaln(%) p-value
Femalen(%) Malen(%)
Agegroup <0.001
18---59years 195(70.9) 80(29.1) 275(56)
≥60years 121(56.0) 95(44) 216(44)
BNI 0.007
Underweight 8(2.5) 3(1.7) 11(2.2)
Eutrophic 82(25.9) 68(38.9) 150(30.5)
Overweight 118(37.3) 70(40.0) 188(38.3)
ObesitygradeI,IIandIII 108(34.2) 34(19.5) 142(28.9)
Associateddiseases 0.692
No 87(27.5) 54(30.9) 141(28.7)
One 123(38.9) 70(40) 193(39.3)
Twoormore 106(33.6) 51(29.2) 157(32)
SAH 162(51.3) 834(47.4) 246(50.1) 0.236
DM 34(10.8) 22(12.6) 56(11.4) 0.321
Smoker <0.001
Yes 29(9.2) 25(14.3) 54(11.0)
No 287(90.8) 150(85.7) 437(89.0)
Useofdrugs 0.013
Yes 255(80.7) 125(71.4) 380(77.4)
No 61(19.3) 50(28.6) 111(22.6)
Functionalclassification(MET) <0.001
<4METs 31(9.8) 28(16) 59(12)
≥4METs 231(73.1) 91(52) 322(65.6)
≥10METs 54(17) 56(32) 110(22.4)
Physicalstatus---ASA 0.151
ASAI 82(25.9) 49(28) 131(26.7)
ASAII 211(66.8) 105(60) 316(64.4)
ASAIII 23(7.3) 21(12.0) 44(9)
Needforreferral 0.633
Yes 20(6.3) 13(7.4) 33(6.7)
No 296(94.9) 153(91.2) 458(98.3)
Decompensateddisease 0.474
Yes 11(3.5) 7(4.2) 18(3.7)
No 305(96.5) 168(95.8) 473(96.3)
Total 316(100) 175(100) 491(100)
SAH,SystemicArterialHypertension;DM,DiabetesMellitus.Numbersinboldarestatisticallysignificant.
theyaccountforover70%ofthecausesofdeathsinBrazil. Cardiovasculardiseases, cancer,diabetes, chronic respira-torydiseases,andneuropsychiatricdisorders,whicharethe main NCDs, have accounted for a high number of deaths beforeage70andlossofqualityoflife,causingdisabilities andahigh degree oflimitationof illpeopleintheirwork andleisureactivities.
Alsoaccordingtothe2013NationalHealthSurvey(NHS), theproportionofindividualsaged18andolderwhoreported diagnosisofhypertensioninBrazilwas21.4%,corresponding to31.3millionpeople,withahigherproportionofwomen (24.2%)comparedtomen (18.3%).27 Inthis survey,among
the total number of people between 60 and 64 years of age44.4%reporteda diagnosisof hypertension,a propor-tionthatwas52.7%amongpeopleaged65---74yearsand55% amongpeopleaged75yearsor more,dataverysimilarto thosefoundbyVigitelin2013.25Inthepresentstudy,itwas
found that50.1% of patients had systemicarterial hyper-tension(SAH) withnostatisticaldifferenceintheanalysis bysex.Probablyreflectingthenumberofelderlyinthe pop-ulationstudied,inwhichtherateofNCDsand,amongthem SAH,ishigherthanthatofthegeneralpopulation.
Table6 Variablesrelatedtosurgicalprocedureclassifiedaccordingtosex.
Variablesrelatedtosurgicalprocedure Sex Totaln(%) p-value
Femalen(%) Malen(%)
Specialty <0.001
Generalsurgerya 115(36.4) 68(38.8) 183(37.3)
Urology 26(8.2) 62(35.4) 88(17.9)
Gynecology 68(21.5) 0(0) 68(13.8)
Ophthalmology 44(13.9) 13(7.4) 57(11.6)
Other 63(25.4) 32(13.3) 95(19.4)
Surgeryclassification 0.101
Minor 112(35.4) 52(29.7) 164(33.4)
Mid-size 167(52.8) 91(52) 258(52.5)
Major 37(11.7) 32(18.3) 69(14.1)
Previoussurgicalprocedure 0.039
Yes 189(68.7) 167(77.3) 356(72.5)
No 78(24.7) 57(32.6) 135(27.5)
Previoussurgicalanestheticcomplications 0.045
Yes 19(6) 4(3.3) 23(4.7)
No 297(94) 171(97.7) 468(95.3)
aGeneralsurgerycomprisessurgicalproceduresgeneralsurgery,abdominalsurgery,andcoloproctology.
Numbersinboldarestatisticallysignificant.
operationduetosevereuncontrolledhypertensionisrelated to a classic study showing that hypertension is associ-atedwithperioperative cardiovascularcomplications.30 In
asystematicreviewandmeta-analysisof30observational studies,31 it was identified that there is little evidence
that systolic blood pressure under 180mmHg and dia-stolicblood pressureunder110mmHgareassociatedwith perioperative complications. Therefore, it is a consensus amongmostauthorsthatmoderatedegreeofhypertension (180×110mmHg)withouttarget-organdamageshouldnot beareasontopostponeorsuspendoperations.Forsevere hypertension,thebenefitsofdelayingasurgicalprocedure tocontrolbloodpressureshouldbeweighedagainsttherisks of postponing the curative operation. One should always keep in mind that the blood pressure improvement time shouldberespected,suddencorrectionsshouldbeavoided anda postoperativeclinical follow-up ensured.32 Another
challengeposedbythismorbidityisthecorrect identifica-tionandassessmentofpossiblelesionsintargetorgansand associatedmorbidities,suchasunderlyingcoronarydisease, congestiveheartfailure,hypertrophyand/orleft ventricu-laroverload, cerebral atherosclerosis, andimpaired renal function.While uncontrolled isolated SAH is considered a minorrisk factor16 andwhenaccompanied byhypertrophy
orleftventricularoverloadisknowntobeanindependent cardiovascularriskfactor.33
Inthissample,theoccurrence ofpatientswith decom-pensatedhypertension(>180×110mmHg)wasverylow,but accordingtotheabove,it isbelievedthat itisduringthe outpatientpreoperative assessment thatthe hypertensive patientshould be identified and treated through internal medicineand/orcardiologyappointmentsandproper guid-ancetostrictadherencetodrugprescription.Moreover,itis
duringthistimethatacarefulevaluationofpossiblelesions intargetorgansallowsacorrectstratificationof cardiovas-cularriskandplanningtheperioperativesurgicalanesthetic management.
AccordingtoSartorelli,34 theprevalence oftype2
dia-betesmellitus hasexponentiallyincreased,particularly in developing countries. Whereas in developed nations, the increaseoccursmainlyintheolderagepopulation,sothatin thoseaged45---64yearstheprevalenceisexpectedtotriple, whileinthoseaged20---44yearsand65yearsormoreitis expected todouble.According toVigitel Brazil,25 in 2013
the frequencyof previous diagnosis ofdiabetes was6.9%, with6.5% for menand 7.2%for women. According tothe 2013NHS,276.2%oftheBrazilianpopulationaged18orolder
reportedhavingbeendiagnosedwithdiabetes,reaching20% of the age group of 65---74 years.The results obtained in ourpopulationshowaprevalenceof11.5%,alsowithhigher percentagesintheelderlygroup(17.6%)withoutstatistical differencebetweensexes.BecauseDMisanimportant pre-dictor of postoperative death and ischemic heart disease is the most common cause of postoperative morbidity in thesepatients,35strictpreoperativeassessmentisrequired,
involvingareferraltoaspecialistwheneverneeded. Theresultsobtainedin thisstudycomparedwiththose foundbythe2013NHSregardinghypercholesterolemia(8.1% vs.12.5%),occurrenceofasthma(5.1%vs.4.4%),andheart diseases(5,2%vs.5.0%)weresimilar.
of medication use, age and weight of the patient, and concurrencewithenzymeinduction,amongothers.36
During PAE, after identifying the continueduse of any drug, the decision to maintain, discontinue or change the drug should be based on the evaluation of each case, which sometimes requires interaction with other medical specialty. It is worth noting that in this study, because SAH was the most frequent associated disease, soitwastheuseofantihypertensivedrugs.Among these, the angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptorblocker (ARB) werethe most used (36.8%),followedbydiuretics(25.5%).Suchmedicationsare thesubjectofrecentcontroversiesregardingits periopera-tivemaintenance.37Thisisduetothefactthatthereisstill
insufficientevidencefor definingwhichgroups ofpatients orwhichoperationswouldbenefitornotfromdiscontinuing theperioperativeuseofACEinhibitorsandARBblockers.
Among the study patients, 11% reported the use of tobacco,menwithahigherpercentagethanwomen(14.3% vs.9.2%).According tothe2013NHS,27 theprevalenceof
currentusersoftobaccoproducts,smokedornon-smoked, dailyoroccasionally,was15%,alsowithahigherpercentage ofusersamongmen(19.2%)thanamongwomen (11.25%), afindingclosetothatreportedinthisstudy.Otherstudies withsimilarresultsarethe studyby Vigitel2013,27 which
in all the27 cities surveyed found an 11.3%frequency of adult smokers,andthe studyconducted at theUniversity HospitaloftheFederalUniversityofSantaCatarina,which found aprevalence of18.7% ofsmokersin thepopulation studied.28 Becausesmokingisan important riskfactor for
theonsetofvariouschronicdiseases,thishabitremainsasa globalleaderamongthepreventablecausesofdeath.29Itis
undeniablethatthecircumstancesdescribedaboveismost relevantamongpatientscandidateforsurgicaltreatment.
TheuseoftheDukeActivityStatusIndex14revealedthat
aminorityofpatients(12.6%)hadpoorfunctionalcapacity (MET <4).Particularlyin thisgroup,the increasedcardiac risk wasreported.32 In astudy of600 patientsundergoing
non-cardiacsurgery,perioperativemyocardialischemiaand other cardiovascularcomplications were morecommonin patientswithfunctional capacitybelow4MET, evenafter adjustingfor other risk factors.32 The functional capacity
categorizationperformed for all patientsduring PAE aims toguidethechoiceofsurgical procedure,choiceof surgi-caltechniqueandanestheticagents,typeofintraoperative monitoring,andpostoperativesurveillancelevel.
Inthisstudy,themostfrequentphysicalstatuswasASA II,whichmeansthatmostpatientshadmoderatesystemic disease without functional limitation. The prevalence of patients withASA II was alsofound in other preoperative evaluationstudies.18---20Whenanalyzingthisvariablebyage,
itisseenapredominanceofolderpeoplebothinASAIIand ASAIII.Thisconfirmsthatthisisthemostprevalentgroup inthediagnosisofmoderatetosevereassociateddiseases, compensatedornot.
Our result withonly 6.7% of the patients whoneeded referraltomedicalspecialtiesdiffersfromtheresultsofa study conducted by Bisinotto,20 which showedthat 11.9%
of thestudy population had clinical decompensation and, therefore, needed referral, particularly tocardiology. We believe that this difference is due to the low frequency (3.7%)ofpatientswiththisconditioninoursample.
IntheUnitedStates,theelderlypopulationaccountsfor 20---40% of surgical procedures, 50% of emergency opera-tions,and75%ofsurgicalmortality.38Theelderlymorbidity
inelectivesurgeryrangesfrom10%to58%;thisvariationis duetolackofuniformdefinitionsfortheconceptof compli-cation, variability of the surgical procedures performed, andnon-proportionaldivisionofindividualspergroupabove 60yearsold.38 Mortalityandmorbidityin electivesurgery
hasdeclinedinrecentdecadesduetoimprovementsin secu-rity,anestheticandsurgicaltechniquesandassessment,and preoperativecare.38Thereisaconsensusthatmortalityand
surgicalmorbidityinthispopulationarenotrelatedtoage buttophysiologicalaspectsofaginganditsresponseto sur-gicalaggression.Thepresenceofpreexistingdiseaseandthe severityofthebasicsurgicalconditionmakeevaluationand preoperative care the key to success in the management of surgical elderly, prevention and treatment of possible complications.
In the study population, the predominant group was the general surgery group, followed by urology, gynecol-ogy,andophthalmologygroups.Whenanalyzingthesurgical variables by age and sex, it was found a predominance ofolder peoplein minoroperationsandinophthalmology andurology, of women in gynecologyand ophthalmology, andof men inurology. These findingsare consistent with findingsin the literature, withthemost common surgical diseases in the elderly are the ophthalmological, urolog-ical, orthopedic, and surgical diseases of the digestive tract.38 Regardingprevious surgicalprocedure,theelderly
and women represented the largest group, which con-firmsthisgroupgrowingincreaseinallsurgicalprocedures worldwide.38
Consideringit isnot mandatorytorefer elective surgi-calpatients to a pre-anesthetic evaluation in HUGG,and since the PAE clinic service capacity is lower than the demand for surgery in this hospital we believe that the mainlimitationofthisstudyis thefactthattheremaybe atendencyofsurgeonstoreferolderpatientswithchronic diseasesandcandidatesformajorsurgerytothePAEclinic, ratherthanyoungerpatients candidatesforminorsurgery andwithouthistoryofassociateddiseases.Inthissense,it isworththinkingaboutthefuturepossibilityof standardiz-ingthePAEprocedurealsointhisrespect,withallsurgical patientsbeingevaluatedinloco.
Conclusion
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.DonabedianA. The quality ofcare:how canit be assessed? JAMA.1988;260:1743---8.
2.Kluger MT, Tham EJ, Coleman NA, et al. Inadequate pre-operativeevaluationandpreparation:areviewof197reports from the Australian incident monitoring study. Anaesthesia. 2000;55:1173---8.
3.Klopfenstein CE,Forster A, Van Gessel E.Anesthetic assess-mentinanoutpatientconsultationclinicreducespreoperative anxiety.CanJAnaesth.2000;47:511---5.
4.SchiffJH,FrankenhauserS,PritschM,etal.TheAnesthesia Pre-operativeEvaluationClinic(APEC): aprospectiverandomized controlledtrialassessingimpactonconsultationtime,direct costs,patienteducation,andsatisfactionwithanesthesiacare. MinervaAnestesiol.2010;76:491---9.
5.Halaszynski TM, Juda R, Silverman DG. Optimizing postop-erativeoutcomes withefficientpreoperativeassessmentand management.CritCareMed.2004;324Suppl:S76---86. 6.Resoluc¸ão CFM n◦ 1802/2006, de 20 de dezembro de
2006; sec¸ão I: 160. Sociedade Brasileira de Anestesi-ologia [Internet]. Available from: http://www.sba.com.br/ normaseorientacoes/res18022006.asp[accessed18.7.15]. 7.Bader AM, Hepner DL. Update on preprocedure testing. In:
FleisherLA,editor.Evidence-basedpracticeofanesthesiology. 3rded.Saunders/ElsevierInc.;2013.p.8---13.
8.IglesiasAC.Cuidadospré-operatórioseriscocirúrgico.Atheneu. 2010:63---92.
9.Preoperative tests | Guidance and guidelines | NICE [Inter-net]. Available from: https://www.nice.org.uk/guidance/cg3 [accessed18.7.15].
10.ApfelbaumJL,ConnisRT,NickinovichDG.Practiceadvisoryfor preanesthesiaevaluation:anupdatedreportbytheAmerican SocietyofAnesthesiologistsTaskForceonPreanesthesia Evalu-ation.Anesthesiology.2012;116:522---38.
11.Lee JA. The anaesthetic out-patient clinic. Anaesthesia. 1949;4:169---74.
12.Guidelines for AmbulatoryAnesthesia and Surgery.Aprovado por ASA House of Delegates em 15 de outubro de 2003, alterado em 22 de outubro de 2008. Available from: http://www.asahq.org10
13.Ministério da Saúde. Secretariade Atenc¸ãoà Saúde. Depar-tamento de Atenc¸ão Básica. Brasília: Ministério da Saúde. [Internet]2006;108p.il.CadernosdeAtenc¸ãoBásica,n.12. SérieA.NormaseManuaisTécnicos.Obesidade.Programase políticasdenutric¸ãoealimentac¸ão. Availablefrom:https:// pt.scribd.com/doc/11555582/ministerio-da-saude-cadernos-de-atencao-basica-n12-obesidade[accessed20.7.14]. 14.HlatkyMA,BoineauRE,HigginbothamMB,etal.Abrief
self-administered questionnaireto determine functional capacity (The Duke Activity Status Index). Am J Cardiol. 1989;64: 651---4.
15.Fitz-HenryJ.TheASAclassificationandperi-operativerisk.Ann RCollSurgEngl.2011;93:185---7.
16.Eagle KA, Berger PB, Calkins H, et al. ACC/AHA guide-line update for perioperative cardiovascular evaluation for noncardiac surgery --- executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1996 Guidelines on Perioperative Cardiovascular Evalu-ation for Noncardiac Surgery). J Am Coll Cardiol. 2002;39: 542---53.
17.DavisNJ.AnaesthesiarelatedmortalityinAustralia1994---1996: reportoftheCommitteeConvenedUndertheAuspicesofthe AustralianandNewZealandCollegeofAnaesthetists.Australian andNewZealandCollegeofAnaesthetists;1999.
18.Gusman PB, do Nascimento Júnior P, Castiglia YMM, et al. Avaliac¸äo pré-anestésica ambulatorial. Rev Bras Anestesiol. 1997;47:522---7.
19.MendesFF, Mathias LAST, Duval Neto GF, et al. Impacto da implantac¸ãode clínica de avaliac¸ãopré-operatória em indi-cadoresdedesempenho.RevBrasAnestesiol.2005;55:175---87. 20.BisinottoFMB,PedriniM Jr,AlvesAAR,etal.Implantac¸ãodo servic¸odeavaliac¸ãopré-anestésicaemhospitaluniversitário. Dificuldadeseresultados.RevBrasAnestesiol.2007;57:167---76. 21.Instituto Brasileiro de Geografia e Estatística [homepage na internet] Censo demográfico 2010. Available from: http://www.ibge.gov.br[accessed15.5.15].
22.Organizac¸ãoPan-Americanade Saúde.Envelhecimento ativo: umapolíticadesaúde.Brasília;2005,60p.
23.Pesquisa Nacional por Amostra de Domicílios 2008. Um PanoramadaSaúdenoBrasil---Acessoeutilizac¸ãodosservic¸os, condic¸õesdesaúdeefatoresderiscoeprotec¸ãoàsaúde2008. Available from: http://www.ibge.gov.br/home/estatistica/ populacao/panoramasaudebrasil20032008/comentarios.pdf [accessed15.5.15].
24.Pesquisa de orc¸amentos familiares 2008/2009. Available from: http://www.ibge.gov.br/home/estatistica/./pof/./pof 20082009 encaa.pdf[accessed15/05/2015].
25.Vigitel Brasil.Vigilânciade fatoresde risco eprotec¸ãopara doenc¸ascrônicasporinquéritotelefônico.Secretariade Vigilân-ciaemSaúdeSecretariadeGestãoEstratégicaeParticipativa BrasíliaDF:MinistériodaSaúde;2013.
26.Guaragna LP, Dall’Alba DP, Goulart P, et al. O impacto da obesidade na morbimortalidade de pacientes submetidos à cirurgiaderevascularizac¸ãomiocárdica.SciMed.2008;18Suppl 2:75---80.
27.PesquisaNacional de Saúde. Percepc¸ãodo estado de saúde, estilosde vida edoenc¸ascrônicas: Brasil, grandesregiões e unidadesdafederac¸ão;2013.Availablefrom:http://www.ibge. gov.br/home/estatistica/populacao/pns/2013/ [accessed 15.5.15].
28.BarretoRB,PincelliMP,SteinwandterR,etal.Tabagismoentre pacientes internadosem um hospital universitáriono sul do Brasil: prevalência, grau de dependência e estágio motiva-cional.BrasPneumol.2012;38:72---80.
29.World Health Statistics 2011. Available from: http://www.who.int/whosis/whostat/2011/en/ [accessed 15.5.15].
30.Prys-RobertsC,MelocheR, Foex P.Studies ofanaesthesiain relationtohypertensionI:cardiovascularresponsesoftreated anduntreatedpatients.BrJAnaesth.1971;43:122---37. 31.KhuriSF,DaleyJ,HendersonW, etal.TheNationalVeterans
AdministrationSurgicalRiskStudy:riskadjustmentforthe com-parativeassessmentofthequalityofsurgicalcare.JAmColl Surg.1995;180:519---31.
32.Fleisher LA, Fleischmann KE, Auerbach AD, et al. 2014 ACC/AHAguidelineonperioperativecardiovascularevaluation and management ofpatients undergoing noncardiacsurgery. Executivesummary:areportoftheAmericanCollegeof Car-diology/American Heart Association Task Force on Practice Guidelines.JAmCollCardiol.2014;64:2373---405.
33.FleisherLA.Preoperativeevaluationofthepatientwith hyper-tension.JAMA.2002;287:2043---6.
34.Sartorelli DS,Franco LJ.Tendênciasdo diabetesmellitus no Brasil: o papel datransic¸ãonutricional. Cad SaúdePública. 2003;19:29---36.
36.Tumber PS, Cullen DF. Drug interactions for the anesthe-siologist. ASA Refresher Courses in Anesthesiology. 2000;28: 215---28.
37.Rosenman DJ, McDonald FS, Ebbert JO, et al. Clini-cal consequences of withholding versus administering
renin-angiotensin-aldosterone system antagonists in the preoperativeperiod.JHospMed.2008;3:319---25.