online | memorias.ioc.fiocruz.br Leishmaniases are diseases caused by protozoa of the
genus Leishmania. Human infection occurs through the bite of an infected sandfly and it is estimated that ap-proximately two million new cases of leishmaniasis oc-cur each year; however, only approximately 600,000 are reported (Ashford et al. 1992). In Brazil, cases are report-ed for all regions and leishmaniasis is especially common in the states of Ceará, Maranhão and Bahia (MS 2007).
Leishmaniasis can manifest as a tegumentary form that includes cutaneous and mucocutaneous leishmaniasis or as a visceral form of the disease. The difference in clini-cal manifestation depends on the host immune system and the infecting parasite strain (Yoneyama et al. 2007). The most common clinical form of tegumentary leishmaniasis (TL) is cutaneous leishmaniasis (CL). CL is characterised by a single ulcer, which is also referred to as localised CL (LCL) and this ulcer may spontaneously regress or disseminate into the multiple ulcers and papules, which are characteristic of disseminated leishmaniasis (DL), an emerging form of leishmaniasis (Costa et al. 1986, Turetz et al. 2002). Multiple studies of the morphological
pathol-ogy of leishmaniasis have been performed in attempts to establish a morphological pattern that could be used to differentiate between the lesions (Azulay 1960, Ridley et al. 1980, Magalhães et al. 1986a).
In infected individuals who do not develop lesions or disease, the immune response expresses a T-helper (Th)1 pattern that can be detected in peripheral blood cells (Carvalho et al. 1985). However, the intensity of inflammation can also result in ulcerations in which the healing capacity of these cells is lost, thus favouring the immunopathology of the disease (Gollob et al. 2005).
In LCL, the lesions involve a local inflammatory re-action composed primarily of plasma cells, macrophages and lymphocytes. Experimental studies have evaluated T lymphocytes and their contributions to the lesion reso-lution process and to resistance to infection (Müller et al. 1994, Milon et al. 1995, Scott & Farrell 1998). In hu-mans, several studies have evaluated the frequency and the pattern of T cells in the peripheral blood and tissues from TL (Uyemura et al. 1993, Carvalho et al. 1994, da-Cruz et al. 1994, Diaz et al. 2002, Antonelli et al. 2005, Campanelli et al. 2006).
One study suggested that the humoral response was not essential for the development of protective immunity in human leishmaniasis (McSorley et al. 1996). However, studies in experimental models have shown that B cell depletion leads to disease exacerbation, suggesting that B cells are necessary for the activity of the T cells that mediate lesion healing; thus, humoral responses may in fact play a role in mediating protective immunity against doi: 10.1590/0074-0276130312
Financial support: NIH (AI-30639), INCT, ICIDR + Corresponding author: [email protected] Received 15 March 2013
Accepted 17 December 2013
Comparative analysis of the tissue inflammatory response
in human cutaneous and disseminated leishmaniasis
Marina Loyola Dantas1/+, Juliana Menezes Gomes Cabral de Oliveira1,
Lucas Carvalho2,3, Sara Timóteo Passos2,3, Adriano Queiroz2,3, Luiz Henrique Guimarães2,3, Paulo Machado2,3, Edgar Carvalho2,3, Sérgio Arruda1
1Laboratório Avançado de Saúde Pública, Centro de Pesquisas Gonçalo Moniz-Fiocruz, Salvador, BA, Brasil 2Serviço de Imunologia, Hospital Universitário Professor Edgard Santos, Universidade Federal da Bahia, Salvador, BA, Brasil
3Instituto Nacional de Ciência e Tecnologia de Doenças Tropicais, Salvador, BA, Brasil
Cutaneous leishmaniasis (CL) is the most frequent clinical form of tegumentary leishmaniasis and is charac-terised by a single or a few ulcerated skin lesions that may disseminate into multiple ulcers and papules, which characterise disseminated leishmaniasis (DL). In this study, cells were quantified using immunohistochemistry and
haematoxylin and eosin staining (CD4+, CD68+, CD20+, plasma cells and neutrophils) and histopathology was used
to determine the level of inflammation in biopsies from patients with early CL, late CL and DL (ulcers and papules). The histopathology showed differences in the epidermis between the papules and ulcers from DL. An analysis of the cells present in the tissues showed similarities between the ulcers from localised CL (LCL) and DL. The papules had
fewer CD4+ T cells than the DL ulcers. Although both CD4+ cells and macrophages contribute to inflammation in
early CL, macrophages are the primary cell type associated with inflammation intensity in late ulcers. The higher
frequency of CD20+ cells and plasma cells in lesions demonstrates the importance of B cells in the pathogenesis of
leishmaniasis. The number of neutrophils was the same in all of the analysed groups. A comparison between the ul-cers from LCL and DL and the early ulul-cers and papules shows that few differences between these two clinical forms can be distinguished by observing only the tissue.
leishmaniasis (Scott et al. 1986). Comparisons of the im-mune responses involved in LCL and DL have indicated that the host immunity in LCL is more efficient, with
higher production of interferon (IFN)-γ and tumour ne-crosis factor (Turetz et al. 2002, Guimarães et al. 2005). The differences in the immune responses between the localised and disseminated forms may provide in-formation regarding protection and resistance against leishmaniasis parasites. The present study used histo-pathology and the detection of cells in situ to examine the differences between the two clinical forms of leish-maniasis. Correlations between cell populations and the total extent of inflammation may highlight aspects of the tissue response and elucidate leishmaniasis pathogene-sis. Thus, the present study aimed to compare the histo-pathology and cell infiltrates in biopsies from patients with early and late LCL and from patients with DL who presented both ulcers and papules.
SUBJECTS, MATERIALS AND METHODS
Patients characteristics - We evaluated 30 patients divided into the following four groups: 10 patients with skin lesions diagnosed with recent LCL (LCL-E) (with-in 20 days after the appearance of the first lesion), 10 patients with late LCL (LCL-L) (lesions for more than 30 days) and 10 patients with DL who had both ulcers (DL-U) and papules (DL-P), resulting in two biopsies per patient in this group. Biopsies were performed for diagnosis and selected according to the clinical criteria specified above. The analysed variables were obtained from medical records.
Leishmaniasis was diagnosed in subjects depending on clinical criteria, positivity for Montenegro intrader-mal skin test, parasite culture, polymerase chain reac-tion and histopathology. Grocott staining was used for fungal differential diagnosis and immunohistochemis-try (IHC) using a polyclonal anti-Leishmania antibody was performed for confirmation when necessary.
Biopsy: procedure, processing and analysis - Skin fragments obtained from the borders of ulcers or pap-ules were performed using a 4-mm “punch” while the patient was under local anaesthesia. The fragments were fixed in 10% formalin for 48 h and processed at the his-totechnology laboratory at Oswaldo Cruz Foundation (Fiocruz). After paraffin embedding, the tissues were
cut into 5-μm sections for staining with haematoxylin
and eosin (H&E) and for IHC.
Immunohistochemical staining - The tissue sections obtained from paraffin were deparaffinised and rehy-drated. IHC reactions were performed after blocking peroxidase activity with 3% hydrogen peroxide for 5 min. The slides were incubated at 25ºC with anti-CD4 (M3354, Spring, USA), anti-CD68 (M071801-5, DAKO, USA) or anti-CD20 (Mob 004, DBS) antibodies at dilu-tions of 1:500, 1:50 and 1:50, respectively. A Peroxidase Mouse & Rabbit Kit/HRP (DBS KP500, USA) was used to perform the reaction according to the manufacturer’s recommendations. All of the slides were counter-stained with Harris haematoxylin, dehydrated and mounted with Canadian balsam and glass coverslips.
Cellular composition analysis - A Nikon ACT-1 with v.2.70 software was used to capture 15 random images from 15 different fields of each tissue sample at 400X magnification. The quantification of CD4+, CD20+ and CD68+ cells was performed manually using ImageJ soft-ware (National Institutes of Health). Neutrophils and plasma cells were directly quantified from fragments stained with H&E following the same methodology. The numbers of cells were reported as absolute values (number of cells/15 fields).
Inflammation quantification - Images of tissue frag-ments stained by H&E were captured as described. The analysis was performed on the total area of the tissue
fragment and the extent of inflammation (μm2) was de-termined using ImageJ software. The percentage of in-flammation/fragment total area was determined.
Histopathological analysis - Histopathological anal-ysis was performed by two observers on all of the frag-ments stained with H&E. The morphological character-istics of each biopsy were evaluated for their presence (+) or absence (0) and reported in a worksheet. Changes were observed in the epidermis (fibrin crust, hyperkera-tosis, acanthosis, hydropic degeneration, spongiosis and exocytosis) and in the dermis (oedema, granulation tis-sue, granulomas, giant cells and lytic necrosis).
Ethical considerations - The study was approved by the Human Ethical Committee of the Gonçalo Moniz Research Center under Fiocruz protocol 321-2009.
Statistical analysis - Statistical analyses were per-formed using GraphPad Prism 5.0. Spearman correla-tion analysis, Kruskal-Wallis and Pearson correlacorrela-tions and One-Way ANOVA were performed as non-paramet-ric and parametnon-paramet-ric tests, respectively. The results were considered statistically significant when p < 0.05. A chi-square test was performed to compare the frequencies between variables in independent samples.
RESULTS
Twenty patients with LCL were placed in the follow-ing subgroups accordfollow-ing to the duration of their lesions: LCL-L, for those with lesions with more than 30 days and LCL-E, when diagnosed with an ulcer for less than 20 days. The other 10 patients had DL and all of these patients had simultaneous ulcerated primary lesions (DL-U) plus secondary lesions due to dissemination (DL-P), thereby forming a fourth group composed of the same patients. The clinical characteristics of the patients are described in Table I.
The epidermis and dermis were analysed separately. The analysed histopathological-characteristic frequen-cies and the comparisons between the groups are de-scribed in Table II.
in 20% of the cases. However, unlike early ulcers, late lesions had more spongiosis (80%), granulomas (90%) and lytic necrosis (50%) (Table II).
The histopathological characteristics of the epider-mis were much different between the secondary lesions and ulcers in DL. The ulcers presented higher frequen-cies of hyperkeratosis (90%), hydropic degeneration (70%) and spongiosis (80%) and lacked a fibrin crust. The papules presented a fibrin crust in 40% of the cases and presented acanthosis in 70% of the cases. Exocytosis was equal between the ulcers and papules (50%). These differences were not observed in the dermis (Table II).
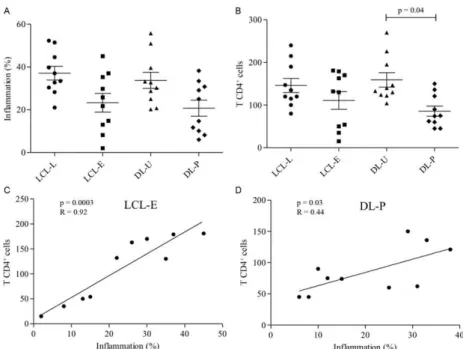
A higher percentage of inflammation was observed in the LCL-L group (37 ± 10) compared with recent lesions (23 ± 13) (Fig. 1A). We evaluated the time and extent of the lesion area and found that the lesions increased with disease progression only in the more advanced ulcers (over 30 days) (data not shown).
The primary and secondary lesions of patients with DL had various degrees of inflammation. The ulcerated lesions (DL-U) had a higher inflammatory infiltrate (35 ± 12) compared with the papular lesions (DL-P) (20 ± 12) (Fig. 1A). Although the ulcerated lesions of this group were present for a similar time as the LCL-L le-sions (over 30 days), there was no correlation with lesion area, as observed in the other group (data not shown). The area of the papules was not measured.
The presence of CD4+ T lymphocytes, although not statistically significant, was higher in the late ulcers than in the recent ulcers (Figs 1B, 2A). A comparison between the number of CD4+ cells and the level of inflammation showed that the amount of CD4+ cells increased with the inflammatory infiltrate in early ulcers (Fig. 1C). In later lesions, no correlation between CD4+ cells and inflamma-tion was observed (data not shown). In DL, CD4+ T lym-phocytes were more prevalent in ulcers than in papules (Fig. 1B). Unlike the ulcers, the papules showed a positive correlation between the number of CD4+ lymphocytes and the extent of the inflammatory infiltrate (Fig. 1D).
Macrophages were the most prevalent cell type and showed similar frequencies between LCL-L and LCL-E (Figs 2B, 3A). Unlike the CD4+ T lymphocytes, the
num-ber of CD68+ macrophages in the inflammatory infiltrate progressively increased as inflammation increased, in both types of lesions (Fig. 3B, C). In DL biopsies, CD68+ cells were slightly higher in the ulcerated lesions than in the papules (Fig. 3A). Unlike what was observed for LCL lesions, the presence of macrophages did correlate with increased inflammatory infiltrate in the DL lesions (data not shown).
CD20+ B cells and plasma cells (Fig. 2C, D) in the LCL-L and LCL-E groups were similar and appeared more frequently in the late lesions (Fig. 4). In DL, the CD20+ B lymphocytes were present in the same amount in the ulcers and papules. Although not significant, plas-ma cells tended to be more frequent in DL ulcers (Fig. 4A, B). The number of CD20+ B and plasma cells did not correlate with inflammatory infiltration in any of the four lesions evaluated (data not shown)
Neutrophils were rarely found in the tissues and ap-peared in equal numbers in all groups (Fig. 5A, B). How-ever, in the early phase of ulcers, neutrophils appeared to be gradually recruited and correlated with increased inflammatory infiltrate; this did not occur in the older ul-cers (Fig. 5C). However, the number of neutrophils did not correlate with lesion duration (data not shown). Neutro-phils were also rare in DL (Fig. 5B). NeutroNeutro-phils appeared to be important during the initial stage of the disease, but their numbers did not correlate with lesion progression or increased infiltration in biopsies (data not shown).
DISCUSSION
The analysis of biopsies showed minimal differences in histology between the clinical forms of CL. Studies that have analysed different clinical forms and biopsies before and after treatment of recurrent CL lesions also did not observe any differences (Esterre et al. 1992, Meh-regan et al. 1999). The frequency of morphological char-acteristics in the early and late LCL lesions is consistent with those described by Magalhães et al. (1982) and by Weigle and Saravia (1996). The differences observed at the epidermis in the biopsies from the DL patients were described in the first study on the histology of DL le-sions (Carvalho et al. 1994). Therefore, it is not possible
TABLE I
Clinical characteristics of patients with cutaneous leishmaniasis (CL)
Characteristics
LCL-L (n = 10)
LCL-E (n = 10)
DL-U (n = 10)
DL-P (n = 10)
Male:female 07:03 07:03 07:03 07:03
Age (mean years ± SD) 25 ± 11 23 ± 9 45 ± 17 45 ± 17
Lesion duration (mean days ± SD) 34 ± 10 17 ± 2 43 ± 20 30 ± 25
Number of lesions (mean days ± SD) 1 1 3 ± 4 29 ± 60
Lesion size (mean mm2 ± SD) 337 ± 240 58 ± 63 185 ± 136 NM
MST (mean mm2 ± SD) 190 ± 125 322 ± 256 164.6 ± 136 164.6 ± 136
to establish an exact time of evolution of a CL lesion using histopathology and we cannot predict whether this lesion may progress or be cured.
The immune response mediated by T cells with a Th1 or Th2 profile in leishmaniasis has been well described based on findings from peripheral blood cells (Reed & Scott 1993, Coutinho et al. 1996, Ribeiro-de-Jesus et al. 1998, Rocha et al. 1999, Campanelli et al. 2006). How-ever, few studies have evaluated the response in situ (Esterre et al. 1992, Palma & Saravia 1997, da-Cruz et al. 2005, Campanelli et al. 2006) compared with the re-sponse in DL (Carvalho et al. 1994, Turetz et al. 2002, Machado et al. 2011). Unlike studies based on periph-eral blood cells (Esterre et al. 1992, da-Cruz et al. 1994, Campanelli et al. 2006), the analysis of cells in situ made it possible to describe a different immune response pat-tern (Uyemura et al. 1993, Campanelli et al. 2006).
By comparing the inflammatory infiltrates, we found that the late ulcers and the DL ulcers had higher inflammation than the early ulcers or papules. Thus, as the disease progresses, there is a continuous influx of inflammatory cells into the tissues and many inflamma-tory cells remain at the site of infection.
The abundance of CD4+ Th1 cells may be responsi-ble for the development of immunity and for the natural healing of lesions (Uyemura et al. 1993). In biopsies of older ulcers from LCL and DL patients, there was a high-er frequency of CD4+ T cells than in the early lesions and papules; these data are consistent with previous studies (Palma & Saravia 1997, da-Cruz et al. 2005). The early lesions and papules, unlike late and disseminated ulcers, demonstrated a positive correlation between the CD4+ cells and the amount of inflammatory cell infiltration, suggesting that during the early development of the dis-ease, the recruitment of CD4+ cells occurs gradually. However, no association with the extent of inflammation and these cells was found in the late lesions. This may indicate a change to a lesion-healing phase.
Similar numbers of macrophages were observed in both stages of LCL and in the two clinical forms, but there was a slight tendency for increased numbers of macrophages in DL lesions; this predominance was also observed by Vieira et al. (2002). Macrophages were the cell type that showed the strongest correlation with in-flammation in LCL.
Little has been reported about B cells and antibodies in CL patients. Like the study by Vieira et al. (2002), our findings revealed that late LCL lesions had a higher frequency of B lymphocytes than early lesions. Higher
production of IFN-γ is associated with increased anti -body secretion by B cells, helping to contain the
para-sites, but IFN-γ is also associated with Leishmania entry into macrophages, a process that results in permanent lesions (Vieira et al. 2002). Increased levels of antibod-ies in the blood have been associated with dissemina-tion to the mucosa in patients with LCL (Carvalho et al. 1994). Similar numbers of B cells in ulcers and papules may be associated with the dissemination of the parasite. Because of the differences in the immune responses of DL patients, B cells may be more closely related to para-site spreading in these cases. However, in LCL, B cells
T A B L E I I F re q u e n cy o f h is to p at h o lo g ic al a sp e ct s ob se rv e d i n t h e 4 0 c u ta n e o u s l ei sh m a n ia si s ( C L ) a n d d is se m in at e d l ei sh m a n ia si s ( D L ) b io p si e s E p id e rm is D e rm is F ib ri n c ru st H y p e rk e ra tos is A ca n th os is H y d ro p ic d eg e n e ra ti on S p o n g ios is E x o cy tos is Oe d e ma G ra n u la ti o n ti ss u e G ra n ul o m a G ia n t ce lls Ly ti c n e c ros is L C L -L 30 80 10 0 80 80 50 90 90 80 20 50 L C L -E 30 90 10 0 80 50 60 10 0 90 30 20 10 D L -U 0 90 10 70 80 50 10 10 20 20 50 D L -P 40 70 70 50 50 50 10 10 30 30 50 p L C L
-L x L
C L -E NS NS NS NS 0 .0 0 01 NS NS NS 0 .0 0 01 NS 0 .0 0 01 L C L
-L x D
L -U 0 .0 0 01 NS NS NS NS NS 0 .0 01 5 0 .0 01 5 0 .0 0 01 NS NS D L
-U x D
may contribute more to persistent lesions. A new class of B cells capable of acting as regulatory cells (Bregs) has been studied in chronic and autoimmune diseases (Yang et al. 2009, Carter et al. 2012, Giannoukakis & Trucco 2012). An evaluation of the number of Breg cells in le-sions from DL may show that Breg cells also enable the spread of Leishmania.
Plasma cells were frequently observed in the infil-trates of tissue lesions in all of the groups and they were more common than B lymphocytes in the LCL and DL late ulcerative lesions; this observation is consistent with previous studies showing that most of these cells are mature at the lesion site and are responsible for im-munoglobulin production in situ (Magalhães et al. 1986, Esterre et al. 1992, Vieira et al. 2002). In contrast to CD4+ T lymphocytes, the recruitment of B lymphocytes and plasma cells did not occur gradually with disease progression in any clinical form. CD4+ T cells may play a role in inflammation, while B and plasma cells are co-ordinated differently.
Neutrophils were rare compared with the other cells analysed in this study and were present at similar num-bers in all types of lesions. Several studies have evalu-ated neutrophils in leishmaniasis, especially in the early phase of the disease. However, some of the reports are controversial. For example, neutrophils may contribute to protection from the disease, but may also be important for the immunopathology (Müller et al. 2001, Aga et al. 2002, Laskay et al. 2003, von Stebut 2007, Afonso et al. 2008, Daboul 2010). Some studies have suggested that Leishmania can use neutrophils to invade macrophages
during the initial attempt of these cells to contain the parasite (Aga et al. 2002, van Zandbergen et al. 2004). However, Daboul (2010) reported that neutrophils are recruited gradually during the initial phase and that their presence at the late stage occurs after the rupture of phagocytes filled with amastigotes, thus restarting an acute reaction in which neutrophils limit the disease pro-gression (Daboul 2010). These data explain the positive correlation between early LCL and inflammatory
infil-Fig. 1A: inflammation percentage in lesions from localised cutaneous leishmaniasis (LCL) and disseminated leishmaniasis (DL). Mean ± standard deviation (SD) are indicated; B: number of CD4+ T lymphocytes in lesions from LCL and DL. Mean ± SD are indicated; C: linear
cor-relations of Spearman (p = 0.003; R = 0.92) between inflammation (%) and CD4+ T lymphocytes in recent (LCL-E) group; D: linear correlations
of Spearman between inflammation (%) and CD4+ T lymphocytes in DL with papule (DL-P) group (p = 0.03; R = 0.44) (10 patients per group).
Significance levels are indicated. DL-U: DL with ulcers; LCL-L: late LCL.
Fig. 2A: immunostained CD4+ T cells (400X) (arrows); B:
immunos-tained CD68+ cells (400X) (arrows); C: immunostained CD20+ cells
trate and the absence of a correlation with late lesions. The tissues of ulcers from both clinical forms are similar and it is not possible to predict disease dissemi-nation. The early ulcers and papules also showed some histopathological similarities. Although these two clini-cal forms are similar, they represent distinct immunolog-ical moments. The analysis of the dynamics of cellular infiltration into CL lesions in its various clinical forms
contributes to the characterisation of the local inflam-matory response and provides a better understanding of the pathogenesis of the disease.
ACKNOWLEDGEMENTS
To Mr Lago, Ms Neuza and Ms Renda, from Corte de Pe-dra Health Service, and to technicians of the histotechnology service of CPqGM-Fiocruz.
Fig. 5A: in haematoxylin and eosin, the presence of neutrophils in the inflammatory infiltrate (arrows) (400X); B: number of neutrophils in lesions from localised cutaneous leishmaniasis (LCL) and disseminated leishmaniasis (DL); C: linear correlations of Pearson between inflam-mation (%) and neutrophils in recent LCL (LCL-E) group (10 patients per group). DL-P: DL with papules; DL-U: DL with ulcers.
Fig. 3A: number of CD68+ macrophages in lesions from localised cutaneous leishmaniasis (LCL) and disseminated leishmaniasis (DL). Mean ±
standard deviation are indicated; B: linear correlations of Spearman between inflammation (%) (p = 0.0005; R = 0.89) and CD68+ macrophages
recent LCL (LCL-E) group; C: linear correlations of Spearman (p = 0.01; R = 0.59) between inflammation (%) and CD68+ macrophages in late
LCL (LCL-L) group (10 patients per group). DL-P: DL with papules; DL-U: DL with ulcers.
Fig. 4A: number of CD20+ B lymphocytes in lesions from localised cutaneous leishmaniasis (LCL) and disseminated leishmaniasis (DL). Mean
REFERENCES
Afonso L, Borges VM, Cruz H, Ribeiro-Gomes FL, dos Reis G, Dutra AN, Clarêncio J, de Oliveira CI, Barral A, Barral-Netto M, Brod-skyn CI 2008. Interactions with apoptotic but not with necrotic neutrophils increase parasite burden in human macrophages in-fected with Leishmania amazonensis. J Leukoc Biol 84: 389-396.
Aga E, Katschinski DM, van Zandbergen G, Laufs H, Hansen B, Mül-ler K, Solbach W, Laskay T 2002. Inhibition of the spontaneous apoptosis of neutrophil granulocytes by the intracellular parasite
Leishmania major. J Immunol 169: 898-905.
Antonelli LRV, Dutra WO, Almeida RP, Bacellar O, Carvalho EM, Gollob KJ 2005. Activated inflammatory T cells correlate with lesion size in human cutaneous leishmaniasis. Immunol Lett 101: 226-230.
Ashford RW, Desjeux P, Deraadt P 1992. Estimation of population at risk of infection and number of cases of leishmaniasis. Parasitol
Today 8: 104-105.
Azulay RD 1960. Histopatologia da leishmaniose tegumentar.
Der-matol Iber Lat Am 2: 7-15.
Campanelli AP, Roselino AM, Cavassani K, Pereira MSF, Mortara R, Brodskyn CI, Goncalves HS, Belkaid Y, Barral-Netto M, Barral A, Silva JS 2006. CD4+CD25+ T cells in skin lesions of patients
with cutaneous leishmaniasis exhibit phenotypic and functional characteristics of natural regulatory T cells. J Infect Dis 193: 1313-1322.
Carter NA, Rosser EC, Mauri C 2012. Interleukin-10 produced by B cells is crucial for the suppression of Th17/Th1 responses, in-duction of T regulatory type 1 cells and rein-duction of collagen-induced arthritis. Arthritis Res Ther 14: R32.
Carvalho EM, Barral A, Costa JM, Bittencourt A, Marsden P 1994. Clinical and immunopathological aspects of disseminated cuta-neous leishmaniasis. Acta Trop 56: 315-325.
Carvalho EM, Johnson WD, Barreto E, Marsden PD, Costa JL, Reed S, Rocha H 1985. Cell mediated immunity in American cutane-ous and mucosal leishmaniasis. J Immunol 135: 4144-4148.
Costa JM, Marsden PD, Llanos-Cuentas EA, Netto EM, Carvalho EM, Barral A, Rosa AC, Cuba CC, Magalhães AV, Barreto AC 1986. Disseminated cutaneous leishmaniasis in a field clinic in Bahia, Brazil: a report of eight cases. J Trop Med Hyg 89: 319-323.
Coutinho SG, Oliveira MP, da-Cruz AM, de Luca PM, Mendonça SC, Bertho AL, Soong L, McMahon-Pratt D 1996. T-cell responsive-ness of American cutaneous leishmaniasis patients to purified
Leishmania pifanoi amastigote antigens and Leishmania brazili-
ensis promastigote antigens: immunologic patterns associated
with cure. Exp Parasitol 84: 144-155.
Daboul MW 2010. Role of neutrophils in cutaneous leishmaniasis.
East Mediterr Health J 16: 1055-1058.
da-Cruz AM, Bertho AL, Oliveira-Neto MP, Coutinho SG 2005. Flow cytometric analysis of cellular infiltrate from American tegumentary leishmaniasis lesions. Br J Dermatol 153: 537-543.
da-Cruz AM, Conceição-Silva F, Bertho AL, Coutinho SG 1994.
Leishmania-reactive CD4+ and CD8+ T cells associated with cure
of human cutaneous leishmaniasis. Infect Immun 62: 2614-2618.
Diaz NL, Zerpa O, Ponce LV, Convit J, Rondon AJ, Tapia FJ 2002. Intermediate or chronic cutaneous leishmaniasis: leukocyte im-munophenotypes and cytokine characterisation of the lesion. Exp
Dermatol 11: 34-41.
Esterre P, Dedet JP, Frenay C, Chevallier M, Grimaud JA 1992. Cell populations in the lesion of human cutaneous leishmaniasis: a
light microscopical, immunohistochemical and ultrastructural study. Virchows Arch A Pathol Anat Histopathol 421: 239-247.
Giannoukakis N, Trucco M 2012. A role for tolerogenic dendritic cell-induced B-regulatory cells in type 1 diabetes mellitus. Curr Opin
Endocrinol Diabetes Obes 19: 279-287.
Gollob KJ, Antonelli LRV, Dutra WO 2005. Insights into CD4+
mem-ory T cells following Leishmania infection. Trends Parasitol 21: 347-350.
Guimarães LH, Machado PRL, Lessa HA, Lessa M, D’Oliveira A, Carvalho EM 2005. Aspectos clínicos da leishmaniose tegumen-tar. Gaz méd Bahia 75: 66-74.
Laskay T, van Zandbergen G, Solbach W 2003. Neutrophil granulo-cytes-Trojan horses for Leishmania major and other intracellular microbes? Trends Microbiol 11: 210-214.
Machado PR, Rosa MEA, Costa D, Mignac M, Silva JS, Schriefer A, Teixeira MM, Bacellar O, Carvalho EM 2011. Reappraisal of the immunopathogenesis of disseminated leishmaniasis: in situ and systemic immune response. Trans R Soc Trop Med Hyg 105: 438-444.
Magalhães AV, Chiarini LH, Raick AN 1982. Histopathology of cuta-neous leishmaniasis. Rev Inst Med Trop Sao Paulo 24: 268-276.
Magalhães AV, Moraes MAP, Raick AN, Cuentas AL, Costa JML, Cuba CC, Marsden PD 1986. Histopathology of tegumentary leish-maniasis caused by Leishmania braziliensis braziliensis. 2. Tissue humoral response. Rev Inst Med Trop Sao Paulo 28: 293-299.
McSorley S, Proudfoot L, O’Donnell CA, Liew FY 1996. Immunol-ogy of murine leishmaniasis. Clin Dermatol 14: 451-464.
Mehregan DR, Mehregan AH, Mehregan DA 1999. Histologic diag-nosis of cutaneous leishmaniasis. Clin Dermatol 17: 297-304.
Milon G, Giudice GD, Louis JA 1995. Immunobiology of experimen-tal cutaneous leishmaniasis. Parasitol Today11: 244-247.
MS - Ministério da Saúde Brasil 2007. Leishmaniose tegumentar americana. Portal da Saúde. Available from: portal.saude.gov.br/ portal/saude/profissional/area.cfm?id_area=1560.
Müller I, Kropf P, Louis JA, Milon G 1994. Expansion of gamma in-terferon-producing CD8+ T cells following secondary infection of
mice immune to Leishmania major. Infect Immun 62: 2575-2581.
Müller K, van Zandbergen G, Hansen B, Laufs H, Jahnke N, Solbach W, Laskay T 2001. Chemokines, natural killer cells and granulo-cytes in the early course of Leishmania major infection in mice.
Med Microbiol Immunol 190: 73-76.
Palma GI, Saravia NG 1997. In situ characterization of the human host response to Leishmania panamensis. Am J Dermatopathol 19: 585-590.
Reed SG, Scott P 1993. T-cell and cytokine responses in leishmania-sis. Curr Opin Immunol 5: 524-531.
Ribeiro-de-Jesus A, Almeida RP, Lessa H, Bacellar O, Carvalho EM 1998. Cytokine profile and pathology in human leishmaniasis.
Braz J Med Biol Res 31: 143-148.
Ridley DS, Marsden PD, Cuba CC, Barreto AC 1980. A histological classification of mucocutaneous leishmaniasis in Brazil and its clinical evaluation. Trans R Soc Trop Med Hyg 74: 508-514.
Rocha PN, Almeida RP, Bacellar O, de Jesus AR, Filho DC, Filho AC, Barral A, Coffman RL, Carvalho EM 1999. Down-regulation of Th1 type of response in early human American cutaneous leish-maniasis. J Infect Dis 180: 1731-1734.
Scott P, Farrell JP 1998. Experimental cutaneous leishmaniasis: in-duction and regulation of T cells following infection of mice with
Scott P, Natovitz P, Sher A 1986. B lymphocytes are required for the generation of T cells that mediate healing of cutaneous leishma-niasis. J Immunol137: 1017-1021.
Turetz ML, Machado PR, Ko AI, Alves F, Bittencourt A, Almeida RP, Mobashery N, Johnson WD, Carvalho EM 2002. Dissemi-nated leishmaniasis: a new and emerging form of leishmaniasis observed in northeastern Brazil. J Infect Dis 186: 1829-1834.
Uyemura K, Pirmez C, Sieling PA, Kiene K, Paes-Oliveira M, Modlin RL 1993. CD4+ type 1 and CD8+ type 2 T cell subsets in human
leishmaniasis have distinct T cell receptor repertoires. J Immunol 151: 7095-7104.
van Zandbergen G, Klinger M, Mueller A, Dannenberg S, Gebert A, Solbach W, Laskay T 2004. Cutting edge: neutrophil granulocyte serves as a vector for Leishmania entry into macrophages. J
Im-munol173: 6521-6525.
Vieira MGS, Oliveira F, Arruda S, Bittencourt AL, Barbosa Jr AA, Barral-Netto M, Barral A 2002. B-cell infiltration and frequency
of cytokine producing cells differ between localized and dissemi-nated human cutaneous leishmaniases. Mem Inst Oswaldo Cruz 97: 979-983.
von Stebut E 2007. Immunology of cutaneous leishmaniasis: the role of mast cells, phagocytes and dendritic cells for protective im-munity. Eur J Dermatol 17: 115-122.
Weigle K, Saravia NG 1996. Natural history, clinical evolution and the host-parasite interaction in new world cutaneous leishmania-sis. Clin Dermatol 14: 433-450.
Yang HZ, Li Z, Liu HZ, Mi S, Hu ZW 2009. The identification and advances of regulatory B cells. Sheng Li Ke Xue Jin Zhan 40: 297-302.
Yoneyama KAG, Peder LD, Lonardoni MVC, Silveira TGV 2007. Diagnosis of American cutaneous leishmaniasis by enzyme im-munoassay in patients from northern Paraná state, Brazil. Braz J