w w w . r b o . o r g . b r
Original
Article
Communication
between
the
musculocutaneous
and
median
nerves
in
the
arm:
an
anatomical
study
and
clinical
implications
Luis
Ernesto
Ballesteros
∗,
Pedro
Luis
Forero,
Edna
Rocío
Buitrago
UniversidadIndustrialdeSantander(UIS),Bucaramanga,Colombiaa
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received13July2014 Accepted21August2014
Availableonline27December2014
Keywords:
Mediannerve
Musculocutaneousnerve Communication
a
b
s
t
r
a
c
t
Objective:Todeterminethefrequencyandfeaturesofcommunicationbetweenthe muscu-locutaneousnerve(MCN)andmediannerve(MN)inasampleoftheColombianpopulation, andassessitsclinicalimplication.
Methods:Thearmsof53cadaverspecimensthathadbeensubjectedtonecropsyatthe NationalInstituteofForensicMedicine,inBucaramanga,Colombia,werestudied.The struc-turesoftheanteriorcompartmentofthearmweredissectedandcharacterizedregarding thepresenceofcommunicationbetweentheMCNandMN.
Results:Acommunicatingbranchwasfoundin21/106upperlimbs(19.8%),occurring bilat-erallyin10(47.6%)andunilaterallyin11(52.4%),withoutsignificantdifferenceregarding thesideofoccurrence(p=0.30).In17%ofthecases,therewasMCN-MNcommunication inwhichthecommunicatingbranchwasseenleavingtheMCNafterpiercingthe cora-cobrachialismuscle(TypeI).In2.8%,theconnectionwasfromtheMNtotheMCN(Type II).Thelengthofthecommunicatingbranchwas57.8±33.4mm.Thedistancesfromthe proximalanddistalpointsofthisbranchtothecoracoidprocesswere138±39.4mmand 188±48.3mm,respectively.Thecommunicatingbranchwaslocatedmostlyinthemiddle thirdofthearm.
Conclusions: ThefrequencyofMCN-MNcommunicationobservedinthepresentstudyisin themiddleoftherangeofwhatwasreportedinpreviousstudies.MCN-MNconnections needtobetakenintoaccountindiagnosingandmanagingperipheralnervelesionsofthe upperlimbs.
©2015PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.
∗ Correspondingauthor.
E-mail:[email protected](L.E.Ballesteros). http://dx.doi.org/10.1016/j.rboe.2014.08.009
Comunicac¸ão
entre
os
nervos
musculocutâneo
e
mediano
no
brac¸o:
estudo
anatômico
e
implicac¸ões
clínicas
Palavras-chave:
Nervomediano Nervomúsculo-cutâneo Comunicac¸ão
r
e
s
u
m
o
Objetivo: Determinar a frequência e características da comunicac¸ão entre os nervos músculo-cutâneo(MCN)emediano(MN)emumaamostrada populac¸ãocolombiana, e avaliarsuaimplicac¸ãoclínica.
Métodos: Osbrac¸osde53cadáveresforamavaliadosemnecropsianoNationalInstituteof ForensicMedicine,emBucaramanga,Colômbia.Asestruturasdocompartimentoanterior dobrac¸oforamdissecadasecaracterizadasemrelac¸ãoàpresenc¸adecomunicac¸ãoentre MCNeMN.
Resultados: Umramocomunicantefoiencontradoem21/106membrossuperiores(19.8%), ocorrendobilateralmenteem10(47,6%)eunilateralmenteem11(52,4%),semdiferenc¸a significativa emrelac¸ãoao ladoda ocorrência(p=0,30). Em17%doscasos, haviauma comunicac¸ãoentreMCN-MNnaqualoramocomunicanteeravistoemergindodoMCN apósperfuraromúsculocóraco-braquial(TipoI).Em2,8%doscasosaconexãofoidoMN paraoMCN(TipoII).Ocomprimentodoramocomunicantefoi57,8±33,4mm.As distân-ciasentreospontosproximaledistaldesteramoeoprocessocoracóidefoi138±39,4mme 188±48,3mm,respectivamente.Oramocomunicanteselocalizouprincipalmentenoterc¸o médiodobrac¸o.
Conclusão: Afrequênciadacomunicac¸ãoentreMCN-MNobservadanopresenteestudoestá namédiadaquelarelatadaemoutrostrabalhos.AsconexõesMCN-MNdevemserlevadas emconsiderac¸ãonodiagnósticoenomanejodaslesõesdosnervosperiféricosdosmembros superiores.
©2015PublicadoporElsevierEditoraLtda.emnomedaSociedadeBrasileirade OrtopediaeTraumatologia.
Introduction
Attheinfraclavicularlevel,thelateralfascicleofthebrachial plexususuallybifurcatesgivingorigin tothe musculocuta-neousnerve(MCN)andthelateralrootofthemediannerve (MN). However,duringtheembryologicaldevelopment pro-cessitispossiblethatbundlesoffiberscorrespondingtothe MNinitiallyruntogetherwithbundlesoffibersoftheMCN. TheMNrecoversthefibersrequiredtoperformitsmotorand sensorialfunctionsintheupperextremity,onlywhenthe bun-dlesoffiberswereconnectedwiththeirnerveoforigin(MN) attheproximalormid-thirdsofthearm.Althoughwithlow frequency,fibersoftheMCNhavealsobeenseentoinitially runalongoftheMNandlaterreestablishtheirconfiguration throughacommunicatingbranch.1–5
TheincidenceoftheMCN-MNcommunicationhasbeen reportedindiversepopulationgroupswithawide variabil-itybetween2.1and63.5%.5–8Themajorityofthestudiesonly
reporttheMCN-MNcommunication.Maedaetal.3and
Chiara-pattanakometal.6havereportedanoccurrenceof3–6.8%for
the communicationfrom the MNtothe MCN. Information abouttheprevalenceofsideofMCN-MNcommunicationis low.Fewstudiesreportpredominanceoftheleftsideandof theunilateralexpressionofthiscommunicatingbranch.4,9,10
Severalwaystoclassifythiscommunicatingbranchhavebeen proposedbythewidevariabilityinitsexpression.3,7,8,10,11
KnowledgeoftheexistenceoftheMCN-MN communica-tioninthearmisclinicallyimportant;itallowsanadequate
evaluationandmanagementofupperlimbmotordisorders causedbyperipheralnerveinjuriesaswellasacorrectsurgical planningandapproachesofaxillaandarm.10,12–14The
clini-calimplicationsofMCN-MNcommunicationsinthearmhave notbeendescribedindetailforotherpopulations.1,3,6,7,13,15–19
Taking into account that the ethnic factor is decisive for theemergenceofdiversemorphologicalexpressionsandthe absenceofthistypeofinformationfromtheMestizo popula-tion,whichispredominantinLatinAmerica,makesthisstudy highlyrelevantinfreshcadavericmaterial.
Methods
This descriptive study was designed to determine the frequency and morphologic features ofthe MCN-MN com-municationin106freshfrozenupperextremitiesof53male adultswhowereundergoingnecropsyattheNationalInstitute ofForensicMedicine.Thesamplemetthefollowinginclusion criteria:Mestizosubjectswithoutevidenceofdirecttraumaor conditionsinvolvingtheupperextremityandwhowerenot thesubjectsofforensicanalysis.
thearm.Then,theepineuralconnectivetissuewasremoved andboththeMCNandtheMNweredissectedfromtheir ori-ginstotheirrespectivemotorpoints,takingtheirtrajectories inthearmasareference.
TheexistenceofMCN-MNcommunicatingbranchesinthe armwasverifiedandtheirqualitativefeatureswererecorded inaccordancewiththeclassificationproposedbyMaedaetal.3
asfollows:Type Iwhen the communicationis observedat the mid or distalthirds ofthe arm. This classwas subdi-videdinto4subtypes.SubtypeIa:whenthecommunication arose from MCN in its intramuscular via into the coraco-brachialismuscle(CbM).SubtypeIb:whenthecommunicating branchexitsfromMCNbeforethebicepsmuscle(BM)branch. SubtypeIc:whenthecommunicationislocatedbetweenthe branchesgoingtoBMandbrachialismuscle(BrM).SubtypeId: whenthecommunicatingbranchexitsaftertheemergence ofBrMbranch. Similarly,theoccurrenceofcommunicating branches between the MN and the MCN was recorded as Type II with 2subtypes. SubtypeIIa: the branchfrom MN reached the segment between the origins of BM and BrM branches.SubtypeIIb:whenthecommunicatingbranchwas connectedwiththebranchtoBrM.Thelengthofthe commu-nicatingbranchaswellasthedistancesfromtheirproximal anddistalpointstotheacromionwasmeasured.Thelength ofthe arm from the anterior edgeof the acromion tothe bi-epicondylarlineoftheelbowwasmeasuredandthe seg-ment where the communicating branch was located was recorded.
Allmorphometricassessmentsweremadewithadigital caliper(Mitotuyo®)andthefindingswerephotographedwith
a DSLR camera. All findings were digitized in Exceltables andthe statisticalanalyseswerecarriedout.Nominal vari-ablesaredescribedwithratios,whilecontinuousvariablesare describedwithmeansandstandarddeviations.Statistical evi-dencesweretestedwiththesquarechi(2)testandStudentt
testacceptinganalphaerrorofupto5%.Ap-value<0.05was consideredassignificant.
Results
TheMCN-MNcommunicatingbranchwaspresentin21/106 (19.8%) upper limbs evaluated, occurring bilaterally in 10 (47.6%); unilaterallyin 11(52.4%)without significant differ-enceatthesideofoccurrence(p=0.30).Tenwerelocatedat therightandelevenattheleft(p=0.30).
Type I communication was observed in 18 cases (17%) (Fig.1),wheretheMCN-MNcommunicatingbranchemerged afterMCNpiercedCbMandit wasconnectedtothe MNin anobliquetrajectory.ThecommunicationarosefromMCNin itsintramuscularviaintoCbM(subtypeIa)in2cases(11.1%); fromtheproximalsegmentofMCNbeforetothebranchtoBM (subtypeIb)in2cases(11.1%)(Fig.1A);fromthemid-segment oftheMCNbetweentheemergenceofthebranchestoBMand BrM(subtypeIc)in8specimens(44.5%)(Fig.1B),andin6cases (33.3%)thecommunicatingbrancharosefromthebranchto BrM(subtypeId)(Fig.1C).
Inthreespecimens(2.8%)thecommunicatingbranchwas foundfromMNinanobliquetrajectoryatthelevelofthe mid-thirdofthearmandthenitwasconnectedwiththeMCN(Type
DM
a
b
c
DM DM
CbM
CbM
CbM
BM
BM
BM
BrM MN
MCN
MCN
MN
MN UN
Fig.1–Communicationbetweenthemusculocutaneousandmediannerves.(a)MCN–MNcommunicationoriginatedfrom theproximalsegmentofmusculocutaneousnerve(SubtypeIb).Lateralviewofrightarm.DM–deltoidmuscle,CbM– coracobrachialismuscle,BM–bicepsmuscle,MN–mediannerve,UN–ulnarnerve,(*)communicatingbranch,(**)BM additionalhead;(b)MCN–MNcommunication,originatedafterthebranchtothebicepsmuscle(subtypeIc).Lateralviewof leftarm,DM–deltoidmuscle,CbM–coracobrachialismuscle,BM–bicepsmuscle,BrM–brachialismuscle,MCN–
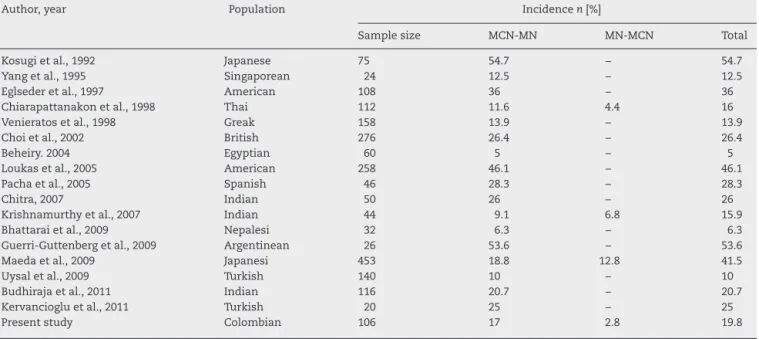
Table1–Incidenceofmusculocutaneous–mediannervescommunicationindiversepopulationaccordingtoseveral authors.
Author,year Population Incidencen[%]
Samplesize MCN-MN MN-MCN Total
Kosugietal.,1992 Japanese 75 54.7 – 54.7
Yangetal.,1995 Singaporean 24 12.5 – 12.5
Eglsederetal.,1997 American 108 36 – 36
Chiarapattanakonetal.,1998 Thai 112 11.6 4.4 16
Venieratosetal.,1998 Greak 158 13.9 – 13.9
Choietal.,2002 British 276 26.4 – 26.4
Beheiry.2004 Egyptian 60 5 – 5
Loukasetal.,2005 American 258 46.1 – 46.1
Pachaetal.,2005 Spanish 46 28.3 – 28.3
Chitra,2007 Indian 50 26 – 26
Krishnamurthyetal.,2007 Indian 44 9.1 6.8 15.9
Bhattaraietal.,2009 Nepalesi 32 6.3 – 6.3
Guerri-Guttenbergetal.,2009 Argentinean 26 53.6 – 53.6
Maedaetal.,2009 Japanesi 453 18.8 12.8 41.5
Uysaletal.,2009 Turkish 140 10 – 10
Budhirajaetal.,2011 Indian 116 20.7 – 20.7
Kervanciogluetal.,2011 Turkish 20 25 – 25
Presentstudy Colombian 106 17 2.8 19.8
II).TypeIIawasfoundin2cases(1.9%)andTypeIIbinonecase (Fig.2).
Thedistancebetweentheacromionandtheproximalpoint ofthecommunicatingbranchwas138±39.4mm.The emer-gencepointofthecommunicatingbranchwasmoredistalat therightsidethanattheleftside(rightside145.7mm;leftside 1329mm).Thedistancefromthedistalpointofthe communi-catingbranchtotheacromionwas188±48.3mm.Thelength ofthearmmeasuredfromthelateraledgeoftheacromion
BrM BM
MCN
MN
Fig.2–Communicationbetweenthemedianand
musculocutaneousnerves.Lateralviewofrightarm.DM– deltoidmuscle,CbM–coracobrachialismuscle,BM–biceps muscle,MCN–musculocutaneousnerve,MN–median nerve,(*)communicatingbranch,(**)BMadditionalhead.
tothebi-epicondylarlineoftheelbowwas298±18.6mm. Fif-teen(71.4%)communicatingbrancheswereseentobelocated atthemidthirdand6(28.6%)brancheswereprojectedfrom theinferioraspectofthemidthirdtothemidpointofthelower thirdofthearm.Thelengthofthecommunicatingbranches was57.8±33.4mm,itwaslongerattherightside(61.9mm) than atthe leftside (53.4mm),but thisdifference wasnot statisticallysignificant(p=0.51).
Discussion
About the frequency of the MCN-MN communication our results(19.8%)areagreewiththemid-range(17–36%)reported bysomeauthors.7,16–18,20,21Thehighestincidenceshavebeen
reported within a range of 37–54.7%.1,3,8,10 The low
inci-dence ofthis communicationisnotorious(range5–16%)in severalstudiesconductedindiversepopulations5,7,9,15,19,22–24
(Table1).Thewidevariabilityspectrumreportedbydiverse authorsisprobablygivenbymultiplefactorssuchasthesize ofthesamples,themethodologyusedandtheancestral bio-logicfeaturesthatdeterminethevariableexpressionofthese structuresintheevaluatedpopulations.
Similarly, ourfindings are consistentwith theliterature concerningtothepredominanceoftheunilateraloccurrence over the bilateral occurrence,1,7,10,12,17,22 and the
predomi-nanceoftheleftsidewithoutstatisticaldifference.5,7Allprior
studies establish thesignificant predominance ofthe pres-ence ofasinglecommunicatingbranchwithintherangeof 90–93.2%andthepresenceoftwocommunicatingbranches withalowfrequency(6.8–10.7%).8,10,17,18,22,25
OurseriesdescribesthepresenceofTypeIMCN-MN com-munication.Thiscommunicationisreportedbymostauthors as the most common with an incidence of 45–72%.3,7,8,22
Similarly, the communicating branch that arose from the mid-segment of the MCN (subtype Ib) indicated by some authors3,6,15asthemostcommononeisinagreementwith
stud-iesthatarepresentbeforetheMCNpiercestheCbM7,7,10,22
were not found in our study. It is probably due to differ-encesofresearcher’sinterpretationabouthowthelateraland medialfasciclesformtheMN.Mostauthorsonlyreferthatthe communicatingbranchgoesfromMCNtoMN5,9,10,15,16,18,22–25
howeverTypeIIcommunicationfromMNtoMCNwasfoundin ourstudyin2.8%accordingtoreportedinotherstudieswith anincidenceof4.4–12.8%,3,6,23wherebythecommunication
betweenMCNandMNmayoccurbothways.
Thedistancesfrom the emergence and endingpoint of the communicating branch to the acromion in our series (138–188mm)areconsistentwiththefindingsofmostprior studiesaswellasthehighprevalenceofthecommunicating branch(50–100%)arisingafterMCNperforatesCbMthathas reportedatthemid-thirdand attheuppersegmentofthe lowerthirdofthearm.4–6
Mostresearcheshavemadequalitativedescriptionabout MCN-MN communication, and onlyfew priorstudies have reportedthelengthofthe communicatingbranch.10,17,20In
ourseriesthelengthofthecommunicationbranch(57.8mm) isrelativelyhigherthan reportedbyChitraet al.17 (45mm)
andLoukasetal.10(46mm)whereasElgsederandGoldman20
reportaconsiderablyshorterlengthforthiscommunicating branch(18mm).
TheMCN-MNcommunicatingbranchwasassociatedtoan additionalheadofthe bicepsbrachii in23.8%casesinour study(Fig.2),ithasalsobeenhighlightedbyotherauthors.1,3,13
Duringtheplanning ofsurgicalproceduresinthearmit is importanttorememberthatapproximately1in4upperlimbs assessedmaypresentaMCN-MNcommunicationassociated withanadditionalheadofthebicepsbrachii.
TheMCNentrapmentisrare.Itcanoccurduetoan inade-quatepositioningofthearmduringsleep26,27becausetheCbM
andBMactasanchorpointforMCN.Ifthissituation coex-istswithacommunicatingbranchwhereapartofMNpasses throughCbM,theclinicalsignscouldbesimilartothosefound inMNneuropathyinthehand.12,14ThediagnosisofMCN-MN
communicationinthisclinical presentationby electromyo-graphicmethodscouldpreventunnecessaryreleases ofthe carpaltunnel.
TheMCN-MN communication should beconsidered for clinicalexaminationofnerveinjuries atthe axillaand the arm,aswellasinthesurgicalprocedurestothisregionlikethe neuromuscularflaps,peripheralnerverepairorevenforthe nerveblocksattheupperextremitiesinanestheticpractice. TheMCNor MNinjuriesproximalor distaltothe commu-nicatingbranchescoulddeterminebeneficial ordeleterious modifications inthe functionand movement of the upper extremity.10,15,24 TheMCN injuryproximal tothe MCN-MN
communicationcanleadtoanunexpectedweaknessofthe forearmflexormusclesandthenarmuscleswithclinicalsigns like seen in a MNinjury at the level of the arm. Further-more,theMNinjuryproximaltotheMN-MCNcommunication can lead to a clinical presentation characterized by func-tionalpreservationofforearmandhandmusclesinnervated byMN.12
In the peripheral nerve surgery, especially in nerve transferstechniques,agoodknowledgeoftheMCN-MN com-munications is required. The MCN has been successfully
usedasareceivernervetotherecoveryofelbowflexion.28,29
Furthermore, the MCN motor branch to BrM has been used as donor to anterior interosseous nerve and poste-rior interosseousnervefor thetreatment oflower brachial plexusinjuries30,31aswellasinthetreatmentoftretraplegic
patients.32Ourstudyisinagreementwithpreviousstudies
aboutTypeIIcincidenceobservedinarangeof16.7–33.3%.3If
theBrMmotorbranchisusedasdonorinnervetransfersand TypeIIccommunicationispresent,couldoccurcompromise oftheforearmpronation,wristandmiddlephalanxflexion and/orsensitivityoflateralfingersofthehand.
Conclusions
KnowledgeoftheexistenceoftheMCN-MNcommunication inthearmisclinicallyimportant;itallowsanadequate evalu-ationandmanagementofupperlimbmotordisorderscaused byperipheralnerveinjuriesaswellasacorrectsurgical plan-ningandapproachesofaxillaandarm.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
WewouldliketorecognizetheNationalInstituteofForensic Medicine,NortheasternColombianregion,forsupplyingthe anatomicalpiecesusedinthisstudy.
r
e
f
e
r
e
n
c
e
s
1.KosugiK,ShibataS,YamashitaH.Supernumeraryheadof bicepsbrachiiandbranchingpatternofthe
musculocutaneousnerveinJapanese.SurgRadiolAnat. 1992;14(2):175–85.
2.KausM,WotowiczZ.Communicatingbranchbetweenthe musculocutaneousandmediannervesinhuman.Folia Morphol(Warsz).1995;54(4):273–7.
3.MaedaS,KawaiK,KoizumiM,IdeJ,TokiyoshiA,MizutaH, KodamaK.Morphologicalstudyofthecommunication betweenthemusculocutaneousandmediannerves.AnatSci Int.2009;84(1–2):34–40.
4.MehtaV,YadavY,AroraJ,KumarH,SuriR,RathG.Anew variantinthebrachiummusculaturewithreinforced innervationfromamedian-musculocutaneousnerve communication.Morphologie.2009;93(301):63–6. 5.UysalII,KarabulutAK,BüyükmumcuM,UnverDoganN,
SalbacakA.Thecourseandvariationsofthebranchesofthe musculocutaneousnerveinhumanfetuses.ClinAnat. 2009;22(3):337–45.
6.ChiarapattanakonP,LeechavengvoongsS,WitoonchartK, VerpairojkitC,ThunasethakulP.Anatomyandinternal topografyofthemusculucutaneosnerveThenervestothe bicepsandbrachiallismuscles.JHandSurgAm.
1998;23(2):250–5.
8. Guerri-GuttenbergRA,IngolottiM.Classifying musculocutaneousnervevariations.ClinAnat. 2009;22(6):671–83.
9. BeheiryEE.Anatomicalvariationsofthemediannerve distributionandcommunicationinthearm.FoliaMorphol (Warsz).2004;63(3):313–8.
10.LoukasM,AqueelahH.Musculocutaneousmediannerve connectionswithinproximalanddistaltothe
coracobrachialismuscle.FoliaMorphol(Warsz). 2005;64(2):101–8.
11.LeMinorJM.Ararevariantofthemedianand
musculocutaneousnerveinman.ArchAnatHistolEmbryol. 1990;73:33–42.
12.ElFalougyH,SelmeciovaP,KubikovaE,StenovaJ,Haviarova Z.Thevariablecommunicatingbranchesbetween
musculocutaneousandmediannerves:amorphological studywithclinicalimplications.BratislLekListy. 2013;114(5):290–4.
13.OzturkNC,UzmanselD,OzturkH.Anunreportedpatternof musculocutaneousandmediannervecommunicationwith multiplevariationsofbicepsbrachii:acasereport.Surg RadiolAnat.2010;32(9):887–90.
14.WertschJJ,MelvinJ.Mediannerveanatomyandentrapment syndromes:areview.ArchPhysMedRehabil.
1982;63(12):623–7.
15.BhattaraiC,PoudelPP.Unusualvariationin
musculocutaneousnervesinNepalese.KathmanduUnivMed J.2009;7(4):408–10.
16.BudhirajaV,RastogiR,AsthanaAK,SinhaP,KrishnaA, TrivediV.Concurrentvariationsofmedianand
musculocutaneousnervesandtheirclinicalcorrelation.A cadavericstudy.ItalJAnatEmbryol.2011;116(2):67–72. 17.ChitraR.Varioustypesofintercommunicationsbetween
musculocutaneousandmediannerves:ananalyticalstudy. AnnIndianAcadNeurol.2007;10(2):100–4.
18.PachaVicenteD,Forcada-CalvetP,Carrera-BurgayaA, Llusá-PérezM.Innervationofbicepsbrachiiandbrachialis: anatomicalandsurgicalapproach.ClinAnat. 2005;18(3):186–94.
19.YangZX1,PhoRW,KourAK,PereiraBP.The
musculocutaneousnerveanditsbranchestothebicepsand brachialismuscles.JHandSurgAm.1995;20(4):671–5.
20.EglsederWAJr,GoldmanM.Anatomicvariationsofthe musculocutaneousnerveinthearm.AmJOrthop. 1997;26(11):777–80.
21.KervanciogluP,OrhanM,KilincN.Patternsofmotor branchingofthemusculocutaneousnerveinhumanfetuses andclinicalsignificance.ClinAnat.2011;24(2):168–78. 22.VenieratosD,AnagnostopoulouS.Classificationof
communicationsbetweenthemusculocutaneousand mediannerves.ClinAnat.1998;11(5):327–31.
23.KrishnamurthyA,NayakSR,VenkatrayaPrabhuL,HegdeRP, SurendranS,KumarM,etal.Thebranchingpatternand communicationsofthemusculocutaneousnerve.JHandSurg Eur.2007;32(5):560–2.
24.Laburthe-TolraY.Basesanatomiquesdeslésionsopératoires dunerfmusculo-cutanédanslachirurgiedel’épaule. Chirurgie.1995;120(3):171–6.
25.Prasada,RaoPV,ChaudharySC.Communicationofthe musculocutaneousnervewiththemediannerve.EastAfr MedJ.2000;77(9):498–503.
26.InabaA,YokotaT.Isolatedmusculocutaneousnervepalsy duringsleep.MuscleNerve.2003;28(6):773–4.
27.MautnerK,KeelJC.Musculocutaneousnerveinjuryafter simulatedfreefallinaverticalwind-tunnel:acasereport. ArchPhysMedRehabil.2007;88(3):391–3.
28.MerrellGA,BarrieKA,KatzDL,WolfeSW.Resultsofnerve transfertechniquesforrestorationofshoulderandelbow functioninthecontextofameta-analysisoftheEnglish literature.JHandSurgAm.2001;26(2):303–14.
29.YangLJ,ChangKW,ChungKC.Asystematicofnervetransfer andnerverepairforthetreatmentofadultupperbrachial plexusinjury.Neurosurgery.2012;71(2):417–29.
30.GarcíaA,FernándezE,MartínezF.Transferofbrachioradialis motorbranchtotheanteriorinterosseousnerveinC8-T1 brachialplexuspalsy.Ananatomicstudy.Microsurgery. 2013;33(4):297–300.
31.RayWZ,YarbroughCK,YeeA,MackinnonSE.Clinical outcomesfollowingbrachialistoanteriorinterosseousnerve transfers.JNeurosurg.2012;117(3):604–9.