SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Clinical
evaluation
of
patients
submitted
to
osteogenic
distraction
in
the
lower
limb
at
a
university
hospital
夽
Francisco
Macruz
Baltazar
Sampaio,
Leilane
Passoni
Marc¸al,
Diogo
Gontijo
dos
Reis,
Adolfo
Watanabe
Kasuo,
Carlos
Eduardo
Cabral
Fraga,
Frederico
Barra
de
Moraes
∗UniversidadeFederaldeGoiás(UFG),FaculdadedeMedicina,Goiânia,GO,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17October2015 Accepted26November2015 Availableonline20August2016
Keywords:
Pseudoarthrosis Osteogenesis,distraction Ilizarovtechnique
a
b
s
t
r
a
c
t
Objective:Toevaluatetheclinicalcharacteristicsfrompatientssubmittedtoosteogenic dis-tractiontocorrectbonegapatauniversityhospital.
Methods:Retrospective transversal study, with a convenience sample, from 2000 to 2012,evaluatingclinicalaspectsofpatientstreated,submittedtoosteogenicdistraction (bone transport)with Ilizarov’sexternal fixation device.The chi-squared, Fisher’s,and Mann–Whitney’sUtestswereusedwitha5%levelofsignificance(p<0.05).
Results:33patientswerestudied,ofwhom28men(84.8%).Themorefrequentagewasfrom 21to40years.Mostpatientswerefromthemetropolitanregionofthecapital(57.6%).The legwasthemostaffectedlimb(75.8%),andtheleftsidewasthemostaffected (66.7%). Themostcommoncausewasinfectedpseudoarthrosis(75.8%).Themostcommonbone transportationtypewasbifocal(75.8%).Meanprevioussurgeryatothersinstitutionswere 2.62(1.93standarddeviation),andmeansurgeriesaftertreatmentwere1.89(1.29standard deviation).Ilizarov’sexternalfixationdevicewasusedfor1.94years(1.34meandeviation), fromonetosixyears.Themostcommoncomplicationswerepininfection(57.6%),equinus (30.3%),deepinfection(24.2%),andshortening(21.2%).
Conclusion: Osteogenicdistractionforbonegapsweremorefrequentinyoungadults,men, intheleg,withbifocaltransportation,afterseveralprevioussurgeries,treatedforamean oftwoyears,withmanycomplications(infectionswerethemostcommon).
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Avaliac¸ão
clínica
de
pacientes
submetidos
à
distrac¸ão
osteogênica
no
membro
inferior
em
hospital
universitário
Palavras-chave:
Pseudoartrose
r
e
s
u
m
o
Objetivo:Avaliarascaracterísticasclínicasdospacientessubmetidosàdistrac¸ãoosteogênica porfalhaósseaemhospitaluniversitário.
夽
StudyconductedattheDepartmentofOrthopedicsandTraumatology,HospitaldasClínicas,FaculdadedeMedicina,Universidade FederaldeGoiás,Goiânia,GO,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](F.B.deMoraes).
http://dx.doi.org/10.1016/j.rboe.2016.08.010
Osteogênesepordistrac¸ão TécnicadeIlizarov
Métodos:Estudotransversal,retrospectivo,comamostradeconveniência,de2000a2012,das característicasclínicasdepacientestratadosesubmetidosàdistrac¸ãoosteogênica (trans-porteósseo)comusodefixadorexternocirculartipoIlizarov.Foramusadosostestesde qui-quadrado,exatode Fishere UdeMann–Whitney,comníveldesignificânciade5% (p<0,05).
Resultados:Foram33casos,28homens(84,8%).Aidademaisfrequentefoientre21e40anos. Amaioriadospacientes(57,6%)eradaregiãometropolitana.Osegmentomaisafetadofoi aperna(75,8%)eoladofoioesquerdo(66,7%).Acausamaisfrequentefoiapseudoartrose infectada(75,8%).Otipodetransporteósseofeitofoiprincipalmenteobifocal(75,8%dos casos).Amédiadeprocedimentospréviosemoutrainstituic¸ãofoide2,62cirurgias(desvio padrãode1,93)eadosfeitosapósoiníciodotratamentofoide1,89cirurgia(desviopadrão de1,29).Otempodeusodefixadorexternofoide1,94ano(desviopadrãode1,34),com mínimodeumanoemáximodeseis.Asquatrocomplicac¸õesmaisencontradasforam infecc¸ãodebasedepinos(57,6%doscasos),equino(30,3%),infecc¸ãoprofunda(24,2%)e encurtamento(21,2%).
Conclusão: Anecessidadededistrac¸ãoosteogênicaporfalhasósseasfoimaisfrequenteem adultosjovens,homens,naperna,comtransportebifocal,apósmúltiplascirurgiasprévias, commédiadeaproximadamentedoisanosdetratamentoecomváriascomplicac¸ões(as infecc¸õesforamasprincipais).
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Injuries to the appendicular skeleton due to high-energy trauma show a high prevalence of severe bone lesions, which can develop complications such as delayed union, pseudarthrosis,infection,malunion, orbonegap.The chal-lenge posedby the treatment ofbone gaps has instigated researchers to find appropriate solutions for the different typesofinjury.1
Amongthemaintechniquesusedfordiaphysealboneloss reconstructionaretheuseoftraditionalbonegraft, tibializa-tionofthefibula,vascularizedbonetransposition,andbone transport(distractionosteogenesis).2Thelatterisdividedinto: (1)isolatedshortening;(2)shorteningfollowedimmediatelyby stretchingthroughdistractioninthefocusofpseudoarthrosis afterashortcompressionperiod;(3)shorteningfollowedby stretchingaway fromthe focus ofpseudoarthrosisthrough corticotomy; and (4) progressive vertical segmental bone transportaftercorticotomy.
Thefirstreportsdescribinglimbstretchingwereprovided byCodvilla,3in1905,andtheuseofexternalfixatortoproduce bonelengtheningbegan in1913, withOmbredanne.4 How-ever,thistechniquedidnotgainwidespreadacceptanceuntil Ilizarov identifiedthe mechanicaland physiologicalfactors governingboneregenerationduringdistractionosteogenesis. In1969,IlizarovandLedyaev5wereabletofillthebonedefect andextendthelimbafterdebridementoftheinfectedbone and,atthesametime,correctdeformities.Theirmethodwas revolutionarybythestandardsoforthopedictreatmentsofthe time.1,6,7
Ilizarovrecommendedthistechniqueforcorrectingbone defectssecondarytocongenitalabnormalities,tumor resec-tions,traumaticboneloss,orasaresultofdebridement in osteomyelitiswithunviablebonetissue.8,9
Thisstudyaimedtoevaluatetheclinicalcharacteristicsof patientsundergoingdistractionosteogenesisduetobonegap inauniversityhospital.
Methodology
This wasa cross-sectionalstudy,with aretrospective con-veniencesample,from2000to2012,whichincludedtreated patientswhounderwentdistractionosteogenesis(bone trans-port)usinganIlizarovcircular externalfixator.Thepresent researchwasapprovedbytheUniversityHospitalEthics Com-mittee.
Datawerecollectedfromareviewofmedicalchartsand storedinanExcel2007spreadsheet.Statisticalanalysiswas performed using SPSS forWindows, version 16.0.The chi-squaredtest,Fisher’sexacttest,andtheMann–WhitneyUtest wereusedtoassesstheinfluenceofthevariablesonthetypes ofcomplications,withasignificancelevelof5%(p<0.05).
Reviewofmedicalchartsretrieved33casestreatedinthis periodusingthismethod.Thefollowingdatawerecollected: sex;ageofpatientsatthebeginningoftreatment,avariable whichwasdividedintoagegroups;areaoforigin;affected seg-ment(tibiaand/orfemur);side;cause;typeofbonetransport performed(bifocal,ortrifocalconvergentortrifocaltandem bonetransport);numberofprevioussurgeriesandnumberof surgeriesafterthetreatmentwasinstituted;timeofexternal fixatoruse;andcomplicationsobservedduringtreatment.
0 2 4 6 8 10 12 14 16 18
41-60 years 21-40 years
10-20 years >60 years
Fig.1–Distributionaccordingtoagegroups.
0 5 10 15 20 25
Congenital diseases
Infected pseudarthrosis
Non-infected pseudarthrosis
Chronic osteomyelitis Tumor
Fig.2–Distributionofcasestreatedaccordingtocause.
thosethatrequiredsurgeryforcorrection(Group2),andthose consideredassequelaeduetotreatmentfailure(Group3).
Results
Thirty-threesubjectswereincluded,28men(84.8%)andfive women(15.2%).Agewasstratifiedintogroups(Fig.1);themost frequentagegroupwas21–40years.
Most patients (57.6%) came from Greater Goiânia; the remainder camemainlyfrom countryside Goiás. Themost affectedsegment was asingleleginjury (75.8%),and most affectedsidewastheleftsideintwothirdsofcases(66.7%).
Thecausesthatledtothechoiceoftreatmentmethodwere stratifiedintofivesubgroups(Fig.2);themostfrequentwas infectedpseudarthrosis(75.8%ofcases).
Thetypeofbonetransport(Fig.3)wasmainlybifocal(75.8% ofcases).
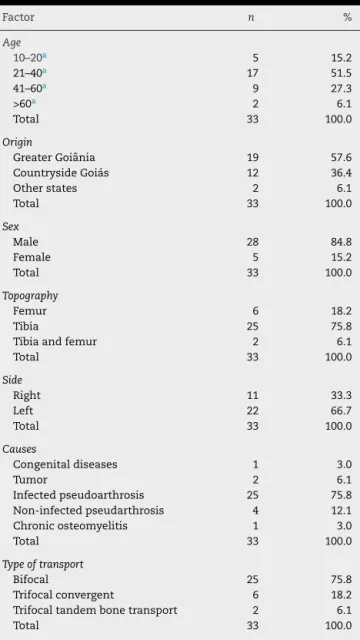
ThevariablesweredistributedandorganizedinTable1. Thenumber ofprevious surgeries performed and those madeduringthetreatmentthroughbonetransportmethod are listedin Table2. Meannumberofprevious procedures atother institutionswas2.62 (standarddeviation1.93)and thatoftheproceduresperformedaftertreatmentonsetwas 1.89(standarddeviation1.29).Meantimeofexternalfixation deviceusewas1.94years(1.34standarddeviation),ranging from1to6years.
0 5 10 15 20 25
Bifocal Trifocal convergent
Trifocal tandem bone trasnport
Fig.3–Typeofbonetransportperformed.
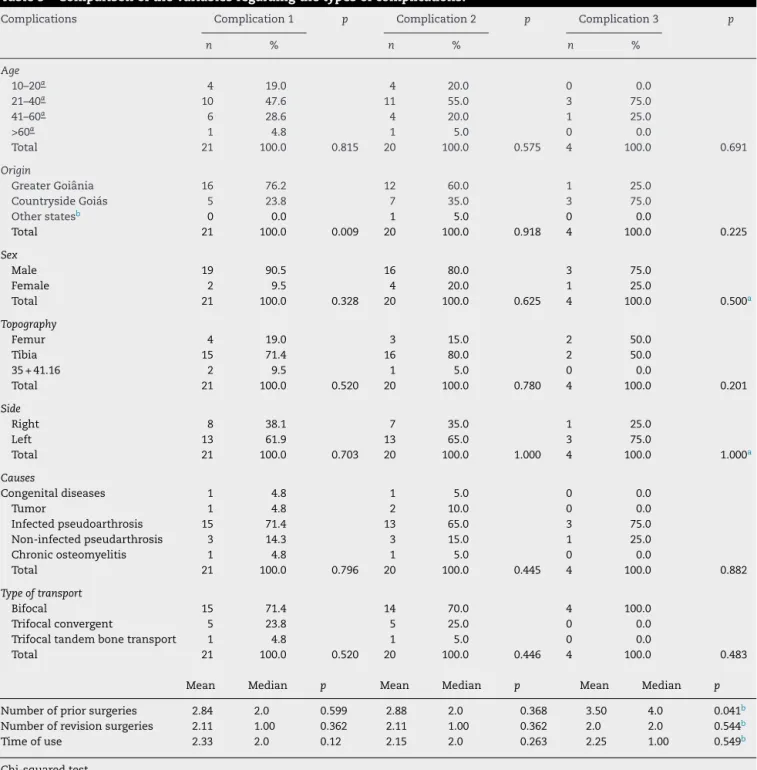
The most common complications were pin infection (57.6%), equinus (30.3%), deep infection (24.2%), and short-ening (21.2%). There was a positive correlation between complications and the number of surgical procedures (p=0.041)andtimeofexternalfixationdeviceuse(p=0.012)
Table1–Distributionofthesampleaccordingtothe variables.
Factor n %
Age
10–20a 5 15.2
21–40a 17 51.5
41–60a 9 27.3
>60a 2 6.1
Total 33 100.0
Origin
GreaterGoiânia 19 57.6
CountrysideGoiás 12 36.4
Otherstates 2 6.1
Total 33 100.0
Sex
Male 28 84.8
Female 5 15.2
Total 33 100.0
Topography
Femur 6 18.2
Tibia 25 75.8
Tibiaandfemur 2 6.1
Total 33 100.0
Side
Right 11 33.3
Left 22 66.7
Total 33 100.0
Causes
Congenitaldiseases 1 3.0
Tumor 2 6.1
Infectedpseudoarthrosis 25 75.8
Non-infectedpseudarthrosis 4 12.1
Chronicosteomyelitis 1 3.0
Total 33 100.0
Typeoftransport
Bifocal 25 75.8
Trifocalconvergent 6 18.2
Trifocaltandembonetransport 2 6.1
Total 33 100.0
Table2–Meanandstandarddeviationofthenumberof surgeriesinthesample.
Factor n Mean SD Min Max
Numberofpriorsurgeries 29 2.62 1.93 1 10
Numberofrevisions 28 1.89 1.29 1 6
Table3–Distributionofthesampleaccordingto complications.
Factor n %
Complications
1.Screwinfection 19 57.6
2.Deepinfection 8 24.2
3.Equinus 10 30.3
4.Kneeflexion 2 6.1
5.ROMlimitation 1 3.0
6.Axialdeviation 6 18.2
7.Repeatedfracture 1 3.0
8.Amputationordisarticulation 3 9.1
9.Shortening 7 21.2
10.Softtissueimpingement 2 6.1
11.Others 5 15.2
(Fig.4).ComplicationswerelistedandcomparedinTables3–5, in which theywere divided into three groups, not includ-ingsuperficialpinsinfections:group1,minorcomplications thatdidnotrequirefurthersurgeryforcorrection(e.g.,mild equinus);group2,complicationsrequiringsurgicalcorrection (e.g.,pronouncedaxialdeviation);andgroup3,complications requiringamputation(e.g.,serious,deepinfections).
Discussion
Distractionosteogenesisisasurgicaltechniquewidelyusedin orthopedicsurgeryforthetreatmentofvariouspathological
Table4–Distributionofcomplicationspergroup accordingtothesample.
Factor n %
Complication1
No 12 36.4
Yes 21 63.6
Total 33 100.0
Complication2
No 13 39.4
Yes 20 60.6
Total 33 100.0
Complication3
No 29 87.9
Yes 4 12.1
Total 33 100.0
conditions suchas limblengthdiscrepancy, bone deformi-ties,and largebonedefectssecondarytotrauma,infection, or resection of malignant tumors, a profilesimilar to that observedinthepresentstudy.Thebasicprincipleofthe tech-nique is a process of bone regeneration from the gradual distraction oftwovascularizedsurfaces, thus formingnew bonetissue.6
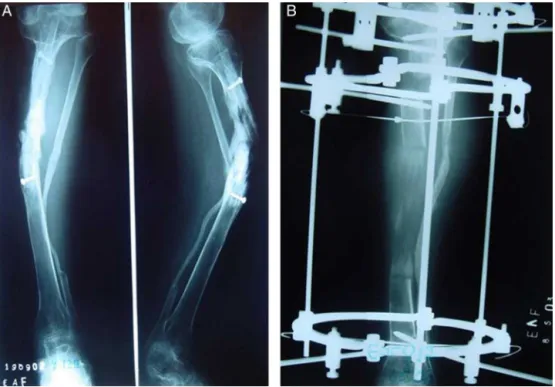
Newboneisgeneratedinthespacebetweentwobone seg-ments,whicharegraduallyandprogressivelydistracted.The distraction rate may vary according to the distraction site, usuallyaround11mm/day.Distractioncanbedonewithan externalfixator, suchas acircularIlizarov fixator ora lon-gitudinalmonoplanarfixator,whichfillstheinterimdefect, whereasintheplacesubjectedtodistraction,anewbone for-mationoccurs,knownasboneregenerate.
Onelimitationofthistechniqueisthelongtimerequired for the newly formed bonetissue mature, mineralize, and
Table5–Comparisonofthevariablesregardingthetypesofcomplications.
Complications Complication1 p Complication2 p Complication3 p
n % n % n %
Age
10–20a
4 19.0 4 20.0 0 0.0
21–40a
10 47.6 11 55.0 3 75.0
41–60a
6 28.6 4 20.0 1 25.0
>60a
1 4.8 1 5.0 0 0.0
Total 21 100.0 0.815 20 100.0 0.575 4 100.0 0.691
Origin
GreaterGoiânia 16 76.2 12 60.0 1 25.0
CountrysideGoiás 5 23.8 7 35.0 3 75.0
Otherstatesb 0 0.0 1 5.0 0 0.0
Total 21 100.0 0.009 20 100.0 0.918 4 100.0 0.225
Sex
Male 19 90.5 16 80.0 3 75.0
Female 2 9.5 4 20.0 1 25.0
Total 21 100.0 0.328 20 100.0 0.625 4 100.0 0.500a
Topography
Femur 4 19.0 3 15.0 2 50.0
Tibia 15 71.4 16 80.0 2 50.0
35+41.16 2 9.5 1 5.0 0 0.0
Total 21 100.0 0.520 20 100.0 0.780 4 100.0 0.201
Side
Right 8 38.1 7 35.0 1 25.0
Left 13 61.9 13 65.0 3 75.0
Total 21 100.0 0.703 20 100.0 1.000 4 100.0 1.000a
Causes
Congenitaldiseases 1 4.8 1 5.0 0 0.0
Tumor 1 4.8 2 10.0 0 0.0
Infectedpseudoarthrosis 15 71.4 13 65.0 3 75.0
Non-infectedpseudarthrosis 3 14.3 3 15.0 1 25.0
Chronicosteomyelitis 1 4.8 1 5.0 0 0.0
Total 21 100.0 0.796 20 100.0 0.445 4 100.0 0.882
Typeoftransport
Bifocal 15 71.4 14 70.0 4 100.0
Trifocalconvergent 5 23.8 5 25.0 0 0.0
Trifocaltandembonetransport 1 4.8 1 5.0 0 0.0
Total 21 100.0 0.520 20 100.0 0.446 4 100.0 0.483
Mean Median p Mean Median p Mean Median p
Numberofpriorsurgeries 2.84 2.0 0.599 2.88 2.0 0.368 3.50 4.0 0.041b
Numberofrevisionsurgeries 2.11 1.00 0.362 2.11 1.00 0.362 2.0 2.0 0.544b
Timeofuse 2.33 2.0 0.12 2.15 2.0 0.263 2.25 1.00 0.549b
Chi-squaredtest.
a Fisher’sexacttest. b Mann–Whitney’sUtest.
finallyconsolidate.Theexternalfixatorshouldbemaintained foranextendedperiod,untiltheconsolidation,whichcanlead tosurgical,social,andpsychologicalcomplications.6,10–12On average,thepresentpatientsunderwentoverfoursurgeries untiltheendoftreatment,usingadynamicfixatorfor2years and with several complications, but approximately 90% of themdidnotexperienceserioussequelae.Thismethodoften eliminatestheneedforsurgeryforskinandamputation cov-erage,astheskinaccompaniesthetransportedbone;italso allowsforthecorrectionofbonedeformitiesanddysmetria, andcuresinfections.
amputation, similar to what was observed in the present sample.
Inmanycases,ablativetechniquessuchaslimb amputa-tionarethebestoptionforthetreatmentofboneloss,since theyobtainresultsfasterandare less costlytothepatient and the healthsystem. During the choice oftreatment, in additiontobiologicalaspects,socialandpsychologicalfactors ofthepatientshouldbeanalyzed.Thebiologicalfactorsthat needtobeconsideredincludebloodsupply,jointandmuscle function,andpresence,location,andseverityofnerve dam-age.Reconstructionisindicatedonlyifitcanprovideagood functional prognosis and if patient has good psychosocial condition.1,5
During distraction osteogenesis, bothboneand soft tis-suesarestretched;thiscanhelpspontaneousclosureofsoft tissueinjuries withoutthe need forskincoverage through plasticsurgery.Someauthors consider thatthe restoration oftheenvelopeofsoftpartsmustbedonebeforeoratthe timeofbonereconstruction.7TheuseofanIlizarovexternal fixatorallowsforthesimultaneouscorrectionof pseudarthro-sis, bone gap, shortening, and angular deformities; it also providesanadequateenvironmentforresolutionofthe infec-tion,evidencedbynumerouspublicationsassuperiortoother methodsoftreatment,whichwasconfirmedbythepresent results.20–23
Conclusion
Theneed for distraction osteogenesis due to bonedefects wasmostfrequentinyoungadults(21–40years),male, com-ingfromGoiânia,forthetibia,duetoinfectedpseudarthrosis aftermultipleprevioussurgeries.Themostusedmethodof transportwasbifocal,withameanofapproximately2years oftreatment,andwithseveralcomplications,ofwhich infec-tionswerethemostfrequent.Mostpatientsdidnotpresent serioussequelaeattheendoftreatment.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. RodriguesFL,MercadanteMT.Tratamentodafalhaóssea parcialpelotransporteósseoparietal.ActaOrtopBras. 2005;13(1):9–12.
2. RigalS,MerlozP,LeNenD,MathevonH,MasqueletAC.Bone transporttechniquesinposttraumaticbonedefects.Orthop TraumatolSurgRes.2012;98(1):103–8.
3. CodivillaA.Theclassic:onthemeansoflengthening,inthe lowerlimbs,themusclesandtissueswhichareshortened throughdeformity.ClinOrthopRelatRes.2008;466(12):2903–9.
4. OmbredanneL.Allongementd’unfemursurunmembretrop court.BullMemSocChirParis.1913;39:1177–80.
5.IlizarovGA,LedyaevVI.Thereplacementoflongtubularbone defectsbylengtheningdistractionosteotomyofoneofthe fragments.ClinOrthopRelatRes.1992;(280):7–10.
6.SailhanF.Bonelengthening(distractionosteogenesis):a literaturereview.OsteoporosInt.2011;22(6):2011–5.
7.TuffiGJ,BongiovanniJC,MestrinerLA.Tratamentodas pseudartrosesinfectadasdatíbiacomfalhasósseaspelo métododeIlizarov,utilizandootransporteósseo.RevBras Ortop.2001;36(8):292–300.
8.PicadoCHF,PaccolaCAJ,AndradeFilhoEF.Correc¸ãodafalha ósseafemoraletibialpelométododotransporteósseode Ilizarov.ActaOrtopBras.2000;8(4):178–91.
9.IlizarovGA.Clinivalapplicationofthetension–stresseffect forlimblengthening.ClinOrthopRelatRes.1990;(250):8–26.
10.BlumAL,BongioVanniJC,MorganSJ,FlierlMA,dosReisFB. Complicationsassociatedwithdistractionosteogenesisfor infectednonunionofthefemoralshaftinthepresenceofa bonedefect:aretrospectiveseries.JBoneJointSurgBr. 2010;92(4):565–70.
11.SangkaewC.Distractionosteogenesiswithconventional externalfixatorfortibialboneloss.IntOrthop.
2004;28(3):171–5.
12.RobertRozbruchS,WeitzmanAM,TraceyWatsonJ,
FreudigmanP,KatzHV,IlizarovS.Simultaneoustreatmentof tibialboneandsoft-tissuedefectswiththeIlizarovmethod.J OrthopTrauma.2006;20(3):197–205.
13.LaviniF,Dall’OcaC,BartolozziP.Bonetransportand compression–distractioninthetreatmentofbonelossofthe lowerlimbs.Injury.2010;41(11):1191–5.
14.MekhailAO,AbrahamE,GruberB,GonzalezM.Bone transportinthemanagementofposttraumaticbonedefects inthelowerextremity.JTrauma.2004;56(2):368–78.
15.El-AlfyB,El-MowafiH,El-MoghazyN.Distraction osteogenesisinmanagementofcompositeboneandsoft tissuedefects.IntOrthop.2010;34(1):115–8.
16.DharSA,MirMR,AhmedMS,AfzalS,ButtMF,BadooAR,etal. Acutepeginwholedockinginthemanagementofinfected non-unionoflongbones.IntOrthop.2008;32(4):559–66.
17.SakurakichiK,TsuchiyaH,WatanabeK,TakeuchiA, MatsubaraH,TomitaK.Distractionosteogenesisofafresh fracturesiteusinganexternalfixator.JOrthopSci. 2006;11(4):390–3.
18.MahaluxmivalaJ,NadarajahR,AllenPW,HillRA.Ilizarov externalfixator:acuteshorteningandlengtheningversus bonetransportinthemanagementoftibialnon-unions. Injury.2005;36(5):662–8.
19.GrivasTB,MagnissalisEA.Theuseoftwin-ringIlizarov externalfixatorconstructs:applicationandbiomechanical proof-ofprinciplewithpossibleclinicalindications.JOrthop SurgRes.2011;6:41.
20.SongHR,ChoSH,KooKH,JeongST,ParkYJ,KoJH.Tibialbone defectstreatedbyinternalbonetransportusingtheIlizarov method.IntOrthop.1998;22(5):293–7.
21.BernerA,ReichertJC,MüllerMB,ZellnerJ,PfeiferC, DienstknechtT,etal.Treatmentoflongbonedefectsand non-unions:fromresearchtoclinicalpractice.CellTissue Res.2012;347(3):501–19.
22.VidalPC,HumbertoP,BenazzoF,CicilianiF,OliveiraK.O métodoIlizarovnotratamentodaspseudartrosesinfectadas. RevBrasOrtop.1997;32(1):905–8.