w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Quality
of
life
and
functional
capacity
of
patients
with
adhesive
capsulitis:
identifying
risk
factors
associated
to
better
outcomes
after
treatment
with
nerve
blocking
Marcos
Rassi
Fernandes
a,∗,
Maria
Alves
Barbosa
a,
Ruth
Minamisawa
Faria
baUniversidadeFederaldeGoiás(UFG),Pós-Graduac¸ãoemCiênciasdaSaúde,Goiânia,GO,Brazil
bUniversidadeFederaldeGoiás(UFG),FaculdadedeEnfermagem,Goiânia,GO,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received26August2016 Accepted11April2017 Availableonline12June2017
Keywords:
Qualityoflife Nerveblock
Outcomeassessment Adhesivecapsulitis Shoulder
a
b
s
t
r
a
c
t
Introduction:Theobjectivesofthisstudyweretoassessthequalityoflifeandfunctional capacityofadhesivecapsulitispatientsatthebeginningandendofprocedureandtoidentify riskfactorsassociatedtobetteroutcomesaftertreatmentwithnerveblocking.
Methods:Aprospectivecohortstudywasperformed.Inclusioncriteriawereclinicalsigns ofadhesivecapsulitisanddiseasechangesonshoulderimagingexams.Theshortformof WorldHealthOrganizationQualityoflifeandDisabilitiesoftheArm,ShoulderandHand questionnaireswereadministeredatthebeginningandendoftreatment.Ascoreof55 pointsormoreontheConstantindexwasusedfordiscontinuationoftreatment.Weused theWilcoxontestforpairedsamples.MultipleregressionanalysisofPoissonwascarriedout usingexposurevariableswithp<0.20intheunivariateanalysisandthesatisfactoryquality oflifeandbetterfunctionalcapabilityasoutcomes.Thesignificancelevelwas5%.
Results:43 patients were evaluated. For the comparison between medians values at the beginning and end of treatment (physical domain: 46.43–67.86; psychologic domain: 66.67–79.17; social domain: 66.67–75; environment domain: 62.5–68.75; DASH: 64.16–38.33), p was <0.05. Aging (physical/psychologic/DASH), higher educational level (physical/environment/DASH),lessseverity(onlyphysical)andfewernerveblocking(only psychologic)weretheseindependentriskfactors.
Conclusions: Qualityoflifeandfunctionalcapacityofthepatientsimproveattheendof procedure.Olderpatientsandhighereducationlevelsaretheriskfactorsmostassociatedto satisfactoryqualityoflifeandbetterfunctionalcapacityaftertreatmentwithnerveblocking. ©2017PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](M.R.Fernandes).
http://dx.doi.org/10.1016/j.rbre.2017.05.003
Qualidade
de
vida
e
capacidade
funcional
de
pacientes
com
capsulite
adesiva:
identificac¸ão
de
fatores
de
risco
associados
a
melhores
desfechos
após
tratamento
com
bloqueio
de
nervo
Palavras-chave:
Qualidadedevida Bloqueiodenervo Avaliac¸ãodedesfecho Capsuliteadesiva Ombro
r
e
s
u
m
o
Introduc¸ão: Osobjetivos desteestudoforamavaliaraqualidadede vidaeacapacidade funcionaldepacientescomcapsuliteadesivanoinícioenofimdoprocedimentodebloqueio denervoeidentificarfatoresderiscoassociadosamelhoresdesfechosapósotratamento.
Métodos: Fez-seum estudodecoorteprospectiva.Oscritériosdeinclusãoforamsinais clínicosdecapsuliteadesivaealterac¸õesdadoenc¸anosexamesdeimagemdoombro. Administrou-seaformaabreviadadoquestionárioWorldHealthOrganizationQualityofLife
eoquestionárioDisabilitiesoftheArm,ShoulderandHandnoinícioenofimdotratamento. Foiusadaumapontuac¸ãode55pontosoumaisnoíndicedeConstantparadescontinuaro tratamento.Usou-seotestedeWilcoxonparaamostraspareadas.Aplicou-seaanálisede regressãomúltipladePoissoncomvariáveisdeexposic¸ãocomp<0,20naanáliseunivariada. Usou-seaqualidadedevidasatisfatóriaeamelhorcapacidadefuncionalcomodesfechos. Oníveldesignificânciafoide5%.
Resultados: Avaliaram-se43pacientes.Nacomparac¸ãoentreosvaloresmedianosno iní-cio e no fim do tratamento (Domínio Físico: 46,43 a 67,86; DomínioPsicológico: 66,67 a 79,17; DomínioSocial: 66,67 a 75; Domínio Ambiental: 62,5 a 68,75; DASH: 64,16 a 38,33), op foi<0,05.Oenvelhecimento (Físico/Psicológico/DASH),a maior escolaridade (Físico/Ambiental/DASH),amenorgravidade(apenasFísico)eamenorquantidadede blo-queiosdenervo(apenasPsicológico)foramfatoresderiscoindependentes.
Conclusões: Aqualidadedevidaeacapacidadefuncionaldospacientesmelhoramnofim doprocedimento.Pacientesmaisidososeumamaiorescolaridadesãoosfatoresderisco associados àqualidadedevida satisfatóriaeà melhorcapacidadefuncionaldepoisdo tratamentocombloqueiodenervo.
©2017PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobuma licenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Outcomemeasurementisanessentialcomponentfor defin-ing the effectivenessof clinical practice.In the orthopedic andrheumatologiccommunity,therehasbeenanincreased interestinoutcomemeasuresthatcapturethepatient’sown perspectiveoftheirclinicalstatus.Theseincludetheanalysis of quality of life (QoL) and functional capacity (FC) con-structs,healthindicatorsthatarewidelyacceptedinmedical interventions.1–3
TheshortformoftheWorldHealthOrganizationQuality ofLife questionnaire(WHOQOL-BREF)isageneric, multidi-mensionaland multicultural QoL measure.Itmay be used withpatients withpsychologicaland physical disorders as well as with healthy individuals.4,5 One limitation of this questionnaire is that it does not address all relevant QoL impairmentissues.Anotherinstrument,theDisabilitiesofthe Arm,ShoulderandHandQuestionnaire(DASH),evaluatesFC andreflectstheimpactofsymptomsandphysicalfunctionon patientswithchronicupper-limbmusculoskeletaldisorders.6 Theinclusionofatleastonegenericandonespecific ques-tionnaireinstudiesevaluatingshoulderdisordershasbeen recommendedsincetheycomplementeachother.7,8
Most studies of adhesive capsulitis patients deal with symptomsofthe disease.Thesestudies analyzetreatment resultsusingpain,strengthandrange-of-motionscales.The
use oftheseconventional clinical methodscan lead toan incompletehealthassessment.9However,ananalysisofthese outcomes(QoLandFC)canprovidecomplementary informa-tionandhelpcharacterizeaffectedindividuals’perceptionof life indifferent dimensions,since nothingis known about thesimultaneoususeoftheWHOQOL-BREFandDASHinthis disease, unless the correlation betweenthe instruments.10 Treatment ofadhesive capsulitis isachallenge sincemost patients havepartialresponse,chronicevolutionand func-tionallimitation.Physicalrehabilitationandmeasurestotreat painandinflammation/adhesionareinsufficientsuggesting thatthereisarelevantpsychosocialcomponent.The objec-tivesofthisstudyweretoevaluatetheQoLandFCofadhesive capsulitispatientsatthebeginningandendofprocedureand toidentifytheriskfactorsassociatedwithsatisfactory qual-ityoflifeandbetterfunctionalcapacityaftertreatmentwith nerveblocking.
Materials
and
methods
Participants
Adultsandelderlypatientswereconsideredtohave adhe-sivecapsulitisiftheyhadconstantandprolongedpainlasting over4weeks,limitationonactiveandpassiveshoulderrange ofmotions,anteriorelevationto130◦,externalrotationto50◦ andinternalrotationtoL5.11
Inclusioncriteriawereclinicalsignsofadhesivecapsulitis, presenceofdisuseosteopeniainshoulderradiographies(true AP,axillaryandscapularview)andvolumetricreductionofthe articularcapsuleassociatedwithobliterationoftheaxillary recessinnuclearmagneticresonanceoftheshoulderinthe preceding30days.
Exclusioncriteriawereagelessthan24years,concomitant diseasessuchascompletelesionoftherotatorcuff,instability, glenohumeralarthrosisandlockeddislocationofthe shoul-der;motorsequelaeofstroke(hemiplegiaorparesis),history ofbreastsurgeryintheprecedingthreemonths; chemother-apyorradiotherapy treatment;bilateral adhesivecapsulitis involvement,previoussurgeryontheaffectedshoulder; diag-nosisofdecompensateddiabetesorglycosylatedhemoglobin greaterthan7%inthepreceding30days;orsubacromial infil-trationorsuprascapularnerveblocking(SSNB)inthe15days priortorecruitment.
Assessmenttools
TheWHOQOL-BREFandDASHinstrumentswerefilledoutby thepatientsincludedinthestudyatthebeginningandendof treatmentinaprivatesettingwithnooneelsepresent.The questionnaireswereself-appliedandpatientsspentan aver-ageof15minperinstrument.Immediatelyafterthepatient wasincludedinthestudy,weeklytreatmentofadhesive cap-sulitiswithSSNBswasstarted.
The final evaluation was carried out when the
Constant–Murley score was greater than or equal to 55 points.Thisclinicalmethodevaluatespain(15points),daily lifeactivities(20points),activejointmobility(40points)and shoulderstrength(25points).12Thisparameterwasusedto decidewhetherornotthenerveblockingshouldbecontinued andwasappliedatthebeginningofeachweeklypatientvisit.
SSNBtechnique
TheSSNBswereperformedbyonlyonetrainedphysicianwith posterioraccessaccordingtothe Dangoissetechnique13on anoutpatientbasiswithouttheaidofaperipheralnerve sti-mulatororimagingtechniques.Weused8mLofbupivacaine chlorhydrate0.5%withepinephrinebitartrate1:200,000, with-outtheassociationofcorticoids.
Datacollection
Exposurevariablesweretreatedaccordingtopredetermined categories: age in years at the time of recruitment, gen-der (male/female), education (greater than/less than or equal to eight years of formal educational level), marital status (unmarried/married), pain at the time of recruit-ment (mild or moderate/severe),12 disease classification (primary/secondary),14diseaseseverityattimeofrecruitment (notsevere/severe),14 diseaseduration(lessthanorequalto three/morethanthreemonths),andnumberofnerveblocking
(lessthan three/greaterthanor equaltothree).Other vari-ableswerealsoconsidered:thesideoftheaffectedshoulder (right/left),dominance(right-handed/left-handed),andsleep (unaffected/affected).12
Endpoints
Outcome variables were QoLand FC. Thetwo instruments mentioned above,WHOQOL-BREFand DASH,wereusedfor theevaluation.WHOQOL-BREFincludes26generalQoL ques-tions and is composed of physical, psychological, social relationshipandenvironmentaldomains.Thefinalscorefor eachdomaincanvaryfromzerotoonehundred,wherezero correspondstoaworsegeneralstateofhealthandahundred toabetterhealthstatus.4DASHisaninstrumentwithgood internalconsistencywhichuses30questionstoevaluatethe FCofpatientswithupper-limbdisorders.Thehigherthescore, thegreaterthefunctionaldisability.6
This study was approved by the Dr. Henrique Santillo ResearchEthics Committee/GOon6/23/2010under number 0014.0.177.000-10.
Statisticalanalysis
DatawereenteredintoaMicrosoftOfficeExcelspreadsheet andanalyzedusingtheStatisticalPackageofSocialSciences (IBM –SPSS 20.0)and STATA12.0.Cronbach’scoefficientof reliabilitywasusedtoassesstheinstruments’internal con-sistency.
Exposurevariablesandothervariableswerepresentedas absolutenumbersandfrequencies.Eachpatient’sDASHand WHOQOL-BREF domain scoreswere calculated atboth the beginningandendoftreatment.DASHscoresandscoreson eachoftheWHOQOL-BREFdomainsweretransformedintoa scaleofzeroto100.
The medians,interquartile intervals and minimum and maximumvaluesfortheDASHandWHOQOL-BREFdomain scores were calculated because oftheir non-normal distri-bution. Tocompare the distribution ofscores (medians)at the beginning and endoftreatment, the Wilcoxon testfor pairedsampleswasused.Box-plotgraphsfortheDASHand WHOQOL-BREF domain scores were constructed using the medianandinterquartileintervals.
Toidentifyvariables associatedwithsatisfactory quality oflifeandbetterfunctionalcapacity,univariateanalysiswas performed usingthechi-square orFisherexact test,where appropriate.
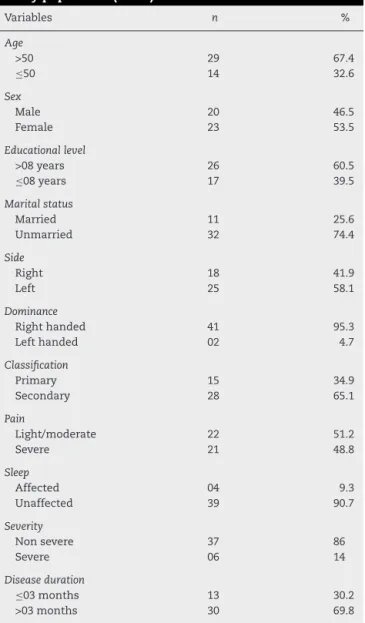
Table1–Clinicalandsociodemographicdataofthe studypopulation(n=43).
Variables n %
Age
>50 29 67.4
≤50 14 32.6
Sex
Male 20 46.5
Female 23 53.5
Educationallevel
>08years 26 60.5
≤08years 17 39.5
Maritalstatus
Married 11 25.6
Unmarried 32 74.4
Side
Right 18 41.9
Left 25 58.1
Dominance
Righthanded 41 95.3
Lefthanded 02 4.7
Classification
Primary 15 34.9
Secondary 28 65.1
Pain
Light/moderate 22 51.2
Severe 21 48.8
Sleep
Affected 04 9.3
Unaffected 39 90.7
Severity
Nonsevere 37 86
Severe 06 14
Diseaseduration
≤03months 13 30.2
>03months 30 69.8
Forallstatisticalanalyses,thesignificancelevelwassetat 5%.
Results
Atotalof47patientsparticipatedinthestudy.Itwasnot pos-sibletocalculatefourpatients’qualityoflifeandfunctional capacityscoresattheendoftreatment,sotheywereexcluded fromthestudy.Thus,thefinalsampleconsistedof43patients. Theaverageagewas54.7years,rangingfrom40to75,and 23(53.5%)oftheparticipantswerefemale.Most(60.5%)had morethaneightyearsofformaleducationallevel.The sec-ondaryformofthediseaseoccurredin65.1%ofcases,with hypothyroidismanddiabetesmellitusoccurringin11.6%and 4.7%ofthecasesrespectively(Table1).
TheinternalconsistencyoftheDASHandWHOQOL-BREF was assessed at the beginning and end of treatment. On theWHOQOL-BREF,Cronbach’salphawascalculatedforthe domains, the questions and each domain individually, as
Table2–WHOQOL-BREFandDASHCronbachcoefficient (n=43).
Cronbach’s˛ Itemsnumbers
WHOQOL-BREF 26questions
Initial 0.91 26
Final 0.91
Domains
Initial 0.90 24
Final 0.90
Physicaldomain
Initial 0.85 7
Final 0.68
Psychologicdomain
Initial 0.73 6
Final 0.82
Socialdomain
Initial 0.62 3
Final 0.70
Environmentdomain
Initial 0.77 8
Final 0.80
DASH
Initial 0.95 30
Final 0.96
Table3–Median,minimumandmaximumvaluesand interquartileintervaloftheDASHandWHOQOL-BREF scoresatthebeginningandendoftreatmentfor patientswithadhesivecapsulitis(n=43).
Domains Minimum–maximum Median Interquartileinterval
Physical
Initial 11–86 46.43 28.57–60.71
Final 36–93 67.86 60.71–78.57
Psychologic
Initial 25–88 66.67 50.00–79.17
Final 25–96 79.17 62.50–83.33
Social
Initial 17–100 66.67 58.33–83.33
Final 25–100 75.00 66.67–83.33
Environment
Initial 19–91 62.50 50.00–71.88
Final 22–94 68.75 56.25–75.00
DASH
Initial 16–100 64.16 50.00–74.16
Final 5–85 38.33 30.00–57.50
showninTable2.TheCronbachcoefficientvaluesobtainedfor thequestionsandforthedomainsshowedsatisfactory inter-nalconsistencyforboththe WHOQOL-BREFand theDASH. Whenassessedindividually,thesocialrelationshipsdomain hadthelowestvalues.
The median, interquartile intervals and DASH and
WHOQOL-BREFdomainsminimums andmaximumsvalues
Table4–UnivariateanalysisofassociatedriskfactorsassociatedwithWHOQOL-BREFdomainsandDASH(n=43).
Variablesofexposure Total PD PsD SD ED DASH
QoL+ p QoL+ p QoL+ p QoL+ p FC+ p
Sex
Male 20 16 0.056 15 0.935 17 1.000 12 0.954 13 0.158
Female 23 12 17 19 14 10
Age
>50 29 23 0.008 26 0.002 25 0.665 20 0.101 18 0.104
≤50 14 05 06 11 06 05
Maritalstatus
Married 11 07 1.000 09 0.698 09 1.000 08 0.480 07 0.434
Unmarried 32 21 23 27 18 16
Educationall.
>8years 26 20 0.045 21 0.295 23 0.407 19 0.036 17 0.053
≤8years 17 08 11 13 07 06
Diseased.
≤3months 13 11 0.096 09 0.709 10 0.655 08 0.925 08 0.486
>3months 30 17 23 26 18 15
Severity
Notsevere 37 26 0.161 28 0.637 31 1.000 23 0.666 20 1.000
severe 06 02 04 05 03 03
Classification
Primary 15 11 0.408 11 1.000 12 0.680 10 0.543 09 0.531
Secondary 28 17 21 24 16 14
N◦ofSSNB
<3 25 19 0.078 22 0.031 22 0.427 15 0.941 15 0.313
≥3 18 09 10 14 11 08
Pain
Light/moderate 22 17 0.087 16 0.795 19 0.698 13 0.850 12 0.887
Severe 21 11 16 17 13 11
PD,physicaldomain;PsD,psychologicaldomain;SD,socialdomain;ED,environmentdomain;QoL+,satisfactoryqualityoflife;FC+,better functionalcapacity;l.,level;d.,duration;N◦,number;SSNB,suprascapularnerveblocking.
asignificantincreaseinthefunctionalcapacityoftheaffected shoulderasmeasuredontheDASH(p<0.001).
After dichotomization of outcomes, univariate analysis identifiedexposurevariablesassociatedwithsatisfactoryQoL in each domain of the WHOQOL-BREF and better FC on theDASH. Onlythesocialdomain didnotobtain variables forinclusion in the Poisson multivariate regression model (Table4).
Olderpatientswereindependentlyassociatedwith satis-factoryQoLonthephysicalandpsychologicalWHOQOL-BREF domains.Highereducationallevelswerepredictiveofhigher scoresonthephysicalandenvironmentaldomains.Physical domain questions 3, 10, 17 and 18 were those that con-tributedmosttohighQoLscoresamongpersonsover50while questions 3, 4and 18 were the largest contributors tothe scoresofthosewithmorethan8yearsofeducationallevel. ThesetwofactorsalsofavoredincreasedFCintheaffected shoulderasmeasuredbytheDASH.Fewernerveblocking con-tributedtobetterQoLscoresonlyinthepsychologicaldomain and a diagnosis of not severe adhesive capsulitis resulted inhigherscores onlyinthe physicaldomainof WHOQOL-BREF(Table5).
Table5–Poissonmultivariateregressionanalysisofthe riskfactorsfortheDASHandWHOQOL-BREFdomains (n=43).
IRRa CI95%b p
Physicaldomainc
Age>50years 1.40 1.20–1.61 0.000
Notseverecapsulitis 1.37 1.13–1.68 0.002
Educationallevel>8years 1.19 1.01–1.40 0.041 Diseaseduration≤ 3months 1.19 0.99–1.43 0.063
Psychologicaldomaind
Age>50years 1.46 1.25–1.70 0.000
Numberofnerveblocking<3 1.34 1.15–1.57 0.000
Environmentdomaind
Age>50years 1.21 1.00–1.48 0.053
Educationallevel>8years 1.28 1.05–1.54 0.012
DASHd
Age>50years 1.21 1.01–1.45 0.040
Educationallevel>8years 1.21 1.00–1.45 0.048
a Incidencerateratio.
b Confidenceinterval.
c Adjustedforsexandpain.
Discussion
ThecomprehensionoftheQoLofpatientswithadhesive cap-sulitisis still limited eventhough the disease isrelatively common.Thepresentstudyshowedbetterqualityoflifeand functional capacity of these patients after treatment with SSNB.Ageabove50yearsandhighereducationwerethemain factorsassociatedwithsatisfactoryQoLandbetterFC.
ThepresentstudyconfirmedthefindingsofBaumsetal., who foundthat thephysical QoLdomain ofadhesive cap-sulitispatients wascompromisedbefore surgicalrelease.15 Thisresultmakessensebecause,inadditiontochronicpain, adhesivecapsulitispatientsfrequentlyexperiencechangesin sleeppatternsandtheabilitytoperformdailyactivities.16The resultsofourstudyconfirmedthatscoresonallQoLdomains increasedsignificantlyaftertreatment. Thesmallest differ-enceinscoresatthebeginningandendoftreatmentwasinthe socialdomain,asalsoreportedbyLorbachetal.,17suggesting thatadhesivecapsulitisdoesnotgreatlyimpactinterpersonal relationships.TheDASHscoresshowedsignificantdisability atthetimeofrecruitmentandincreaseofFCoverthestudy periodintheshoulderaffectedbyadhesivecapsulitis, corrob-oratingtheresultsofHsiehetal.18andBuchbinderetal.19
The relationship between age and QoL has been rela-tively controversial. A year after a traffic accident and in casesoftesticularcancer,respectively,Khatietal.20andFleer etal.,21foundthatyoungerindividualshadhigherQoLscores whilestudiesofpatientswithmentaldisordersandoral dis-eases found higher QoL scores among older subjects.22,23 Theseresultssuggestthatthevariabilityintheassociation betweenageand QoLisprobablydependentonthetypeof healthproblemandtheculturalsensitivitydifferencesofthe QoLassessmenttool.24–26 InBrazil,less experience in cop-ingwithdisabilities and/orfinanciallosses may meanthat youngerindividualshavemoredifficultyadaptingtotheirnew condition.27 Itisalsoreasonabletoassumethatthosewith highereducationallevelswouldnotmissoutonopportunities becauseofthe diseaseandthattheiradaptationto tempo-rarydisabilitywouldbefacilitatedbybetteraccesstohealth information.
Having fewerthan three nerve blocking was associated with higher scores in the psychological domain, possibly because successive invasive procedures have the potential to increase patient anxiety. Also it is possible that people withbetterpsychologicaloutcomesneededlessintervention, becausetheyweremoresatisfiedwiththeircondition.Itis indispensabletomentionthatthepsychologicstatusand pro-fileofhumanbeingisanimportantfactorofimprovement.28 Lessseverityofadhesivecapsulitispatientsresultedinhigher scores in the physical domain of WHOQOL-BREF, probably becauselowerlimitationofshouldermovementsfacilitated theabilitytoperformdailyactivities,aswellasworkcapacity andsatisfactionduringsleep.16
Aschronologicalageincreases,peoplebecomelessactive and gradually less able to perform everyday activities.29,30 However,anobjectiveevaluationofFCdoesnotalways coin-cide with the individual’s perception of his disability as measuredbytheDASH.Inthisstudy,olderpatientsreported bettershoulderFCthan youngerpatients, perhapsbecause
they had more resources available to adapt to or accept disease-imposed limitations. The association between low educationlevelsandthelowestFCcouldbeexplainedby inad-equatewaysofcopingwiththeirdisability.31
Amongthelimitationsofthestudy,theconvenience sam-ple may not be truly representative of all patients with adhesivecapsulitisandmayhavebeeninsufficienttodetect allassociations.Riskfactorssuchascomorbiditiesandother formsoftreatmentwerenotanalyzedinthisstudy.Onthe otherhand,allpatientsinthisstudyweregivenacomplete clinicalevaluationbythesameorthopedicsurgeonand adhe-sive capsulitis wasconfirmed byimaging(radiography and magneticresonance).Oneofthestrengthsofthestudyisits prospectivedesignandtheuseofQoLandFCassessmenttools translated into and validated for Portuguese, whichallows comparisonswithdifferentcultures.
Thisstudyprovidedevidenceforanassociationof sociode-mographiccharacteristicswithimprovedqualityoflifeand functionalcapacityinpatientswithadhesivecapsulitis.These resultscancontributetoabroaderviewofthehealthofthese patientsandmayproveusefulforprofessionalswhofollow individuals receivingthesame typeoftherapyusedinthis research.
Thereisanassociationbetweensociodemographicdatain improving the outcomes studied. Thisinformationmay be usefultoprofessionalswhousetheSSNBsinthetreatment ofthisdisease,whichneedtopayattentiontothesevariables toobtainbetterclinicalresults.Subjectiveevaluationofthe constructsQoLandFCexpandstheknowledgeofprofessional beyondthemerelyclinicalperspectives,understandinghow thepatientsthink,feelandactinthepresenceofadhesive capsulitis.Thecareofthesepatientswiththeappreciation ofitssubjectivityanditsrelatedfactors gainnewnuances, sincethephysicianwhoattendsthemmustrecognizethat dif-ferentindividualsdonotgiveimportancetothesamethings andthereforemustapproachthemindividually.Wereally rec-ommendapopulation-basedstudywithprobabilitysampling techniquestoaddressallvariablesofthepresentresearch.
Conclusions
TheQoLandFCofadhesivecapsulitispatientsimproveatthe endofSSNBprocedure.Olderageandmoreeducationallevel arethemainriskfactorsassociatedwithasatisfactoryquality oflifeandincreasedfunctionalcapacityoftheshoulderafter treatmentwithnerveblocking.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
2. PaananenM,TaimelaS,AuvinenJ,TammelinT,ZittingP, KarppinenJ.Impactofself-reportedmusculoskeletalpainon health-relatedqualityoflifeamongyoungadults.PainMed. 2011;12:9–17.
3. PiitulainenK,YlinenJ,KautiainenH,HäkkinenA.The relationshipbetweenfunctionaldisabilityandhealth-related qualityoflifeinpatientswitharotatorcufftear.Disabil Rehabil.2012;34:2071–5.
4. FleckMPA,LouzadaS,MartaX,CachamovichE,VieiraG, SantosL,etal.ApplicationofthePortugueseversionofthe abbreviatedinstrumentofqualitylifeWHOQOL-BREF.JPublic Health.2000;34:178–83.
5. FleckMP,LealOF,LouzadaS,XavierM,CachamovichE,Vieira G,etal.DevelopmentofthePortugueseversionoftheOMS evaluationinstrumentofqualityoflife.RevBrasPsiquiatr. 1999;21:21–8.
6. AktekinLA,EserF,BaskanBM,SivasF,MalhanS,ÖksüzE, etal.DisabilityofArm,ShoulderandHandQuestionnairein rheumatoidarthritispatients:relationshipwithdisease activity,HAQ,SF-36.RheumatolInt.2011;31:823–6.
7. StaplesMP,ForbesA,GreenS,BuchbinderR.Shoulder-specific disabilitymeasuresshowedacceptableconstructvalidityand responsiveness.JClinEpidemiol.2010;63:163–70.
8. BeatonDE,RichardsRR.Measuringfunctionoftheshoulder.J BoneJtSurg.1996;78:882–90.
9. DeCarliA,VadalàA,PerugiaD,FrateL,IorioC,FabbriM,etal. Shoulderadhesivecapsulitis:manipulationandarthroscopic arthrolysisorintra-articularsteroidinjections.IntOrthop. 2012;36:101–6.
10.FernandesMR.Correlationbetweenfunctionaldisabilityand qualityoflifeinpatientswithadhesivecapsulitis.ActaOrtop Bras.2015;23:81–4.
11.ZuckermanJD,RokitoA.Frozenshoulder:aconsensus definition.JShoulderElbowSurg.2011;20:322–5.
12.ConstantCR,MurleyAHG.Aclinicalmethodoffunctional assessmentoftheshoulder.ClinOrthopRelatRes. 1987;214:160–4.
13.FernandesMR,BarbosaMA,SousaALL,RamosGC.Bloqueio donervosupraescapular:procedimentoimportantena práticaclínica.ParteII.RevBrasReumatol.2012;52:616–22.
14.ZuckermanJD,CuomoF,RokitoS.Definitionand classificationoffrozenshoulder:aconsensusapproach.J ShoulderElbowSurg.1994;3:S72.
15.BaumsMH,SpahnG,NozakiM,SteckelH,SchultzW,Klinger HM.Functionaloutcomeandgeneralhealthstatusin patientsafterarthroscopicreleaseinadhesivecapsulitis. KneeSurgSportsTraumatolArthrosc.2007;15:638–44.
16.HandC,ClipshamK,ReesJL,CarrAJ.Long-termoutcomeof frozenshoulder.JShoulderElbowSurg.2008;17:231–6.
17.LorbachO,KiebM,ScherfC,SeilR,KohnD,PapeD.Good resultsafterfluoroscopic-guidedintra-articularinjectionsin thetreatmentofadhesivecapsulitisoftheshoulder.Knee SurgSportsTraumatolArthrosc.2010;18:1435–41.
18.HsiehLF,HsuWC,LinYJ,ChangHL,ChenCC,HuangV. Additionofintra-articularhyaluronateinjectiontophysical
therapyprogramproducesnoextrabenefitsinpatientswith adhesivecapsulitisoftheshoulder:arandomizedcontrolled trial.ArchPhysMedRehabil.2012;93:957–64.
19.BuchbinderR,HovingJL,GreenS,HallS,ForbesA,NashP. Shortcourseprednisoloneforadhesivecapsulitis(frozen shoulderorstiffpainfulshoulder):arandomised,double blind,placebocontrolledtrial.AnnRheumDis.
2004;63:1460–9.
20.KhatiI,HoursM,CharnayP,ChossegrosL,TardyH,Nhac-Vu H,etal.Qualityoflifeoneyearafteraroadaccident:results fromtheadultESPARRcohort.JTraumaAcuteCareSurg. 2013;74:301–11.
21.FleerJ,HoekstraHJ,SleijferDT,TuinmanMA,KlipEC, Hoekstra-WeebersJEHM.Qualityoflifeoftesticularcancer survivorsandtherelationshipwithsociodemographics, cancer-relatedvariables,andlifeevents.SupportCareCancer. 2006;14:251–9.
22.FontaniveV,AbeggC,TsakosG,OliveiraM.Theassociation betweenclinicaloralhealthandgeneralqualityoflife:a population-basedstudyofindividualsaged50–74inSouthern Brazil.CommunityDentOralEpidemiol.2013;41:154–62.
23.KuehnerC,BuergerC.Determinantsofsubjectivequalityof lifeindepressedpatients:theroleofself-esteem,response styles,andsocialsupport.JAffectDisord.2005;86:205–13.
24.LinSC,KakigiC.Additiveeffectofage-relatedmacular degenerationandglaucomaonqualityoflife.ClinExp Ophthalmol.2016;44:365–6.
25.YilmazF,SahinF,ErgozE,DenizE,ErcalikC,YucelSD,etal. QualityoflifeassessmentswithSF36indifferent
musculoskeletaldiseases.ClinRheumatol.2008;27: 327–32.
26.SchneebergerEE,MarengoMF,DalPraF,CoccoJAM,CiteraG. Fatigueassessmentanditsimpactinthequalityoflifeof patientswithankylosingspondylitis.ClinRheumatol. 2015;34:497–501.
27.MercierC,P’eladeauN,TempierR.Agegenderandqualityof life.CommunityMentHealthJ.1998;34:487–500.
28.VanWijkA,LindeboomJA,JonghA,TukJG,HoogstratenJ. Painrelatedtomandibularblockinjectionsandits relationshipwithanxietyandpreviousexperienceswith dentalanesthetics.OralSurgOralMedOralPatholOral Radiol.2012;114:S114–9.
29.GelfmanR,BeebeTJ,AmadioPC,LarsonDR,BasfordJR. Correlatesofupperextremitydisabilityinmedical transcriptionists.JOccupRehabil.2010;20:340–8.
30.GironP.Timetrendsinself-ratedhealthanddisabilityin olderSpanishpeople:differencesbygenderandage.IranJ PublicHealth.2016;45:289–96.
31.VanEijsden-BesselingMD,VandenBerghKA,StaalJB,DeBie RA,VandenHeuvelWJ.Thecourseofnonspecific