r e v b r a s r e u m a t o l . 2017;57(3):274–277
ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Brief
communication
Use
of
the
Lower
Extremity
Functional
Scale
(LEFS-Brazil)
questionnaire
compared
to
Lequesne
Algofunctional
Index
for
definition
of
knee
and
hip
osteoarthritis
severity
Uso
do
questionário
Lower
Extremity
Functional
Scale
(LEFS-Brasil)
em
comparac¸ão
com
o
Índice
Algofuncional
de
Lequesne
para
definic¸ão
de
gravidade
na
osteoartrite
de
joelho
e
quadril
João
Paulo
M.
Santos
a,
Rubens
A.
da
Silva
a,
Marcos
Tadeu
P.
Fernandes
a,b,
Regina
Célia
Poli-Frederico
a,
Denis
C.
Santos
c,
Rodrigo
A.C.
Andraus
a,
Thais
Maria
F.
Fernandes
a,
Karen
B.P.
Fernandes
a,b,∗aUniversidadeNortedoParaná(UNOPAR),Londrina,PR,Brasil bIrmandadedaSantaCasadeLondrina(ISCAL),Londrina,PR,Brasil cUniversidadeEstadualdeLondrina(UEL),Londrina,PR,Brasil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received7July2015 Accepted18April2016 Availableonline2August2016
Introduction
Osteoarthritis(OA)isachronicjointdiseasewithahigh preva-lenceintheelderly.1OAaffectsmoreoftenthehipandknee,
compromisingimportantaspectsinactivitiesofdailyliving suchaswalking,transpositionofobstacles,homecareand workactivities.2
Severalquestionnaireshaveemergedtoevaluatethe func-tionalcapacityofpatientswithOA,whichstandoutbytheir simplicityand the abilitytoevaluatetheperceptionofthe
∗ Correspondingauthor.
E-mail:[email protected](K.B.Fernandes).
individualaboutthediseaseandhis/herlimitations.3Inthis
context,theLequesneAlgofunctionalIndex(translatedand validatedforthePortuguese)hasaspecialemphasis,bybeing an instrument internationallyrecommended bythe World Health Organizationtoassesspainand functionofthe hip andknee,4,5Lequesne’sIndexiswidelyusedinEurope,6being
oftenusedaspartofaclinicalevaluation.7
Another questionnaire, the Lower Extremity Functional Scale(LEFS),7withaversiontranslatedandvalidatedforthe
Portuguese (LEFS-Brazil),8 has excellentreliability and high
internal consistency and is considered a reliable and easy
http://dx.doi.org/10.1016/j.rbre.2016.07.010
2255-5021/©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
rev bras reumatol.2017;57(3):274–277
275
instrumenttobeappliedbothforresearchandforthe reha-bilitationofpatientswithOA.9
Althoughthereisevidencetodemonstratetheapplicability oftheLEFSquestionnaireinpatientswithOAofthekneeand hip,thereisagapintheabilityoftheinstrumentto discrim-inatebetweendifferentdegreesofseverityofosteoarthritis. Thus,thisstudy aimedtoestablish acutoffpointfor iden-tifyingsevere functional impairmentfor the LEFS-Brazil in elderlypatientswithhipand/orkneeOA,usingasabasisthe LequesneAlgofunctionalIndex.
Method
Ethicalaspects
TheprojectwasapprovedbytheResearchEthicsCommitteeof theUniversityofNorthernParana(OpinionNo.135016).The selectedsubjectswereinformed abouttheobjectivesofthe studyandsignedaConsentform,agreeinginparticipatingin thestudy.
Studydesignandsample
This is a cross-sectional analytical study, based on crite-ria established by the STROBE list – Strengthening the Reportingof ObservationalStudies in Epidemiology,10 with
aconvenience sampleofsecondarydatafrom EELO (Study of Aging and Longevity) project. The EELO project was a thematic project developed by the Universidade do Norte do Paraná (UNOPAR) that aimed to evaluate the indica-torsofthe health statusof elderlysubjects in Londrina, a northerncityofParana. Moreinformationcan befoundat
http://www2.unopar.br/sites/eelo.Thisstudywasconducted
inLondrina,sincetheelderlypopulationofthiscity repre-sents12%ofthe totalpopulation, anumber similartothat foundinotherdevelopedcountries.11,12
ThetotalsampleofEELOprojectconsistedof508 individ-uals,basedontheSampleCalculationforFinitePopulations formula,whichisrepresentativeofthe43,610elderlylivingin LondrinaandregisteredinBasicHealthUnits(SUS).Ofthese seniors,113ofbothgendersreportedhavinghipand/orknee OA,andthatwerephysicallyindependent,accordingto Spir-dusoclassificationsystemforFunctionalStatus(levels3and 4).13
Eligibilitycriteriaofthestudypopulation
The inclusion criteria were: being elderly (age over 60 years), had participated in EELO project, having reported hipand/orkneeOA inthe EELOproject,confirmedby clin-ical examination previously performed by an orthopedist followingthe criteriaproposed bythe American Collegeof Rheumatology,14,15 plusconfirmationbyradiographic
exam-inationperformedbyaspecialistphysician,accordingtothe criteriadescribedbyVasconcelosetal.16
Theexclusioncriteriawere:havingother rheumatic dis-easesaffectingthelowerlimbs(suchasrheumatoidarthritis, gout,andfibromyalgia,determinedbyself-report), osteoporo-sisinthelowerlimbs(verifiedbybonedensitometrywithaT score<-2,517carriedoutsubsequentlytotheEELOProjectand
evaluatedclinicallybyanorthopedist),hip orknee replace-ment(assessedbyself-report),strokesequelae,orParkinson disease (checkedbyself-report),or havinganyother injury that would compromise the locomotor system (such as a tendinopathy,determinedbyself-report).
Clinicalandradiographicevaluation
Thediagnosisandclassificationofsymptoms15,16 of
individ-uals who reported OA were determined byan orthopedist. Subsequently,onlyindividualsdiagnosedwithOAunderwent radiographicexaminationsofthehipsandkneesinthesupine position,withfrontalandsideviews,basedonthecriteriaof KellgrenandLawrence18;allindividualswhoweresubmitted
tothestudywerewithgradeII(mildOA)toIV(advancedOA).A specialistwasresponsiblefortheclassificationofthese sub-jectsincategoriesrelating tothe radiographicfindings;this professionalwasblindedtotheanalyzedoutcomes.
Evaluationoffunctionality
Twoinstrumentstoevaluatethefunctionalstatusofelderly patientswithOAwereemployed:theLequesneAlgofunctional Index,translatedandvalidatedforthePortuguese,which con-tains11questionsinvolvingpain,discomfortandfunctional limitation,6withscoresrangingfrom0to24(noinvolvement
atalltoanextremelysevereimpairment)5;theother
instru-mentusedwastheLEFS-Brazil(LowerExtremityFunctional Scale) questionnaire, which contains 20 specific questions relatedtomusculoskeletalconditionsofthelowerlimbs.In this latterinstrument, the questions relate toactivities of daily living and each question can be classified from 0 to 4 (from extremely difficult, to with no difficulty for carry-ing outactivities)and itsscoresrange from0to80 points, withthevalueof80pointsrepresentingmaximumfunctional capacity.9
Statisticalanalysis
IBMSPSS(StatisticalPackageforSocialSciences,SPSSInc., Chicago)version20.0wasusedforstatisticalanalysisofthe results,anda95%confidenceintervalandasignificancelevel of5%(p<0.05)wereadoptedforalltests.
Initially,descriptivestatisticswerecarriedoutto charac-terize the sample.Then,the cutoffpointforthe definition ofsevereconditionofosteoarthritisthroughLEFS-Brazilwas determined using anROC (Receiver Operating Characteris-tic)curve,andthecategoriesoftheLequesneAlgofunctional Indexwereusedasabaselinetool.
Inaddition,theSpearman’scorrelationtestwasappliedin ordertoverifytherelationshipbetweentheLequesne Algo-functional Indexand LEFS-Brazil,consideringthat thedata isnotnormallydistributedoncethesedatahavearosefrom questionnaires.
Results
276
rev bras reumatol.2017;57(3):274–2771.0
0.8
0.6
0.4
0.2
0.0
0.6 0.4
0.2 0.0
1-specificity
Sensitivity
1.0 0.8
Fig.1–ROCcurveforLEFSforseverefunctional impairment.
wereincluded infinal sample.Ofthese,36 (34.3%)hadhip OA,42(40.0%)hadkneeOAand27(25.7%)hadhipandknee OA.Thesampleconsistedof32men(30.5%)and73women (69.5%)withameanageof70.83±6.06yearsandameanBMI of28.71±5.16.Theelderlysubjectshadamedianof11.5(1stQ: 6.25;3rdQ:17.50)fortheLequesneAlgofunctionalIndexanda medianof48.00(1stQ:35.00;3rdQ:61.00)fortheLEFS-Brazil.
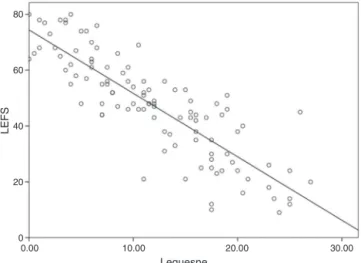
Thedata from the ROC curve was used to identifythe severestatusofosteoarthritisfromLEFS-Brazil,basedonthe Lequesne questionnaire and it is shown in Fig. 1. It was observedthat,foracutoffpointof48,theareaunderthecurve was0.94,withagooddiscriminatorypower ofthispointto characterizemoreseverecaseswithgoodsensitivity(84.4%) andspecificity (81.7%),and withpositiveand negative pre-dictive values of69.89 and 87.50, respectively. Moreover, a correlationbetweentheLequesnequestionnairesand LEFS-Brazil(rS=−0.86,p<0.001)wasobservedandisshowninFig.2.
80
60
40
20
0
0.00 10.00 20.00
Lequesne
LEFS
30.00
Fig.2–CorrelationbetweenLEFSeLequesne
AlgofunctionalIndex.
Discussion
Thisstudy aimedtoidentifysevere statusofosteoarthritis usingtheLEFS-Brazilscore,basedonLequesneAlgofunctional Index. Our findings have demonstrated the existenceof a strong correlation betweenthe questionnairesused, allow-ingtoidentifytheseverestatusoffunctionalimpairmentfor theLEFS-BrazilinelderlypatientswithOA.Thiscategorization couldfacilitatetheclassificationoffunctionalimpairmentof theseindividuals,providingadditionalcriteriatocheckthe impactofthetherapeuticapproachesinactivitiesofdaily liv-ingofelderlypatientswithOA.
Therearemanyquestionnairesassessingindividualswith knee and/orhipOA,withemphasisfortheLequesne Algo-functionalIndexthatreflectsthefunctionalimpairmentand thepainfulpictureoftheindividualinhis/herdailylife,being aninstrumentwithexcellentpsychometricproperties.5,19
Severalstudieshaveevaluatedtheresponsiveness, reliabil-ity,constructvalidityandconvergentvalidityoftheLequesne Indexagainstanotherquestionnaire(WOMAC).20–23
Inapreviousstudy,24weobservedthattheLEFS
question-naireshowsastrongcorrelationwiththeLequesneIndexand alsowithWOMAC,confirmingitsvalidityasaclinicaltoolfor theanalysisoffunctionalimpairmentinelderlypatientswith OA.However,the definitionofcut-off pointsinits scaleof severityofOAhavenotbeenpreviouslypublished,andthese findingscould haveaclinicalrelevance,bothforevaluation andforanalysisoftheeffectivenessofinterventionsinthis patientgroup.
Despite the WOMAC questionnaire being widely used in OA and recommended by the American College of Rheumatology,5thereisnodescriptionofcut-offpointsfor
theseverityofthedisease;thus,thisinstrumentcouldnotbe usedinobtainingtheaccuracyofanalysisproposedinthis study.
Aslimitationsofourstudy,wecanhighlightthesample sizeandthecross-sectionaldesignofthestudyasthe follow-upofthesesubjectswasnotperformed.Anotherimportant aspect isthatthe LEFSquestionnaireisnotan instrument recommendedbytheAmericanCollegeofRheumatologyor bytheEuropeanLeagueofRheumatology.However,LEFSmay representapromisingalternativecomparedtotheWOMAC, becauseit hasgoodinternalconsistencyandisableto dis-criminateissuessuchaspainandfunctionassupportedby thefindingsbyPuaetal.25
ItmaybenotedthattheLEFSquestionnairecanbeusedas amethodforassessingtheprogressionandefficacyof treat-mentofOA,asithastwomainpropertiesoftheinstruments forfunctionalstatusmeasurement8:(1)documentationofthe
outcome oftherapeuticinterventions,toensurethequality and establish clinical standards; and (2) LEFS helps in set-tingobjectivesand targetsforthe treatment,inadditionto measuringtheindividual’sfunctionalprogress.
Conclusion
rev bras reumatol.2017;57(3):274–277
277
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. FelsonDT,NaimarkA,AndersonJ,KazisL,CastelliW,Meenan
RF.Theprevalenceofkneeosteoarthritisintheelderly:
theFraminghamStudy.ArthritisRheum.1987;30:
914–8.
2. SalvatoKF,SantosJP,Pires-OliveiraDA,CostaVS,MolariM,
FernandesMT,etal.Analysisoftheinfluenceof
pharmacotherapyonthequalityoflifeofseniorswith
osteoarthritis.RevBrasReumatol.2015;55:83–8.
3. FaucherM,PoiradeuS,Lefevre-ColauMM,RannouF,
FermanianJ,RevelM.Assessmentofthetest–retestreliability
andconstructvalidityofamodifiedLequesneindexinknee
osteoarthritis.JointBoneSpine.2003;70:520–5.
4. LequesneM.Thealgofunctionalindicesforhipandknee
osteoarthritis.JRheumatol.1997;24:779–81.
5. MarxFC,OliveiraLM,BelliniCG,RibeiroMC.Traduc¸ãoe
validac¸ãoculturaldoquestionárioalgofuncionaldelequesne
paraosteoartritedejoelhosequadrisparaalíngua
portuguesa.RevBrasReumatol.2006;46:253–60.
6. DawsonJ,LinsellL,DollH,ZondervanK,RoseP,CarrA,etal.
AssessmentoftheLequesneindexofseverityfor
osteoarthritisofthehipinanelderlypopulation.Osteoarthr
Cartil.2005;13:854–60.
7. BinkleyJM,StratfordPW,LottSA,RiddleDL.TheLower
ExtremityFunctionalScale(LEFS):scaledevelopment,
measurementproperties,andclinicalapplication.North
AmericanOrthopaedicRehabilitationResearchNetwork.
PhysTher.1999;79:371–83.
8. PereiraLM,DiasJM,MazuquinBF,CastanhasLG,Menacho
MO,CardosoJR.Translation,cross-culturaladaptationand
analysisofthepsychometricpropertiesofthelower
extremityfunctionalscale(LEFS):LEFS-BRAZIL.BrazJPhys
Ther.2013;17:272–80.
9. MetsavahtL,LeporaceG,SpositoMMM,RibertoM,BatistaLA.
Qualomelhorquestionárioparaavaliaraspectosfí-sicosde
pacientescomosteoartritenojoelhonapopulac¸ãobrasileira?
RevBrasOrtop.2011;46:256–61.
10.VonElmE,AltmanDG,EggerM,PocockSJ,GotzschePC,
VanderbrouckeJP.TheStrengtheningtheReportingof
ObservationalStudiesinEpidemiology(STROBE)statement
guidelinesforreportingobservationalstudies.PLoSMed.
2007;4:e296.
11.InstitutoBrasileirodeGeografiaeEstatística.Censo
Demográfico.Brasil:IBGE;2010.
12.LutzW,SamirKC.Dimensionsofglobalpopulation
projections:whatdoweknowaboutfuturepopulationtrends
andstructures?PhilosTransRSocLondBBiolSci.
2010;365:2779–91.
13.SpirdusoWW.Dimensõesfísicasdoenvelhecimento.Barueri:
Manole;2005.p.482.
14.AltmanR,AschE,BlochD,BoleG,BorensteinD,BrandtK,
etal.Developmentofcriteriafortheclassificationand
reportingofosteoarthritis;classificationofosteoarthritisof
theknee.ArthritisRheum.1986;29:1039–49.
15.AltmanR,AlarcónG,AppelrouthD,BlochD,BorensteinD,
BrandtK,etal.TheAmericanCollegeofRheumatology
criteriafortheclassificationandreportingofosteoarthritisof
thehip.ArthritisRheum.1991;34:505–14.
16.VasconcelosKSS,DiasJMD,DiasRC.Relac¸ãoentre
intensidadededorecapacidadefuncionalemindivíduos
obesoscomosteoartritedejoelho.RevBrasFisiot.
2006;10:213–8.
17.InternationalSocietyforClinicalDensitometry.TheISCD’s
officialpositions(updated2005).Washington:ISCD;2005.
18.KellgrenJH,LawrenceJS.Radiologicalassessmentof
osteo-arthrosis.AnnRheumDis.1957;16:494.
19.BellamyN,BuchananWW,GoldsmithCH,CampbellJ,Stitt
LW.ValidationstudyofWOMAC:ahealthstatusinstrument
formeasuringclinicallyimportantpatientrelevantoutcomes
toantirheumaticdrugtherapyinpatientswithosteoarthritis
ofthehiporknee.JRheumatol.1988;15:1833–40.
20.TheilerR,SanghaO,SchaerenS,MichelBA,TyndallA,DickW,
etal.Superiorresponsivenessofthepainandfunction
sectionsoftheWesternOntarioandMcMasterUniversities
OsteoarthritisIndex(WOMAC)ascomparedtotheLequesne
algofunctionalindexinpatientswithosteoarthritisofthe
lowerextremities.OsteoarthrCartil.1999;7:515–9.
21.CacchioA,DeBlasisE,NecozioneS,RosaF,RiddleDL,diOrio
F,etal.TheItalianversionofthelowerextremityfunctional
scalewasreliable,valid,andresponsive.JClinEpidemiol.
2010;63:550–7.
22.Gentelle-BonnassiesS,LeClaireP,MezieresM,AyralX,
DougadosM.Comparisonoftheresponsivenessof
symptomaticoutcomemeasuresinkneeosteoarthritis.
ArthritisCareRes.2000;13:280–5.
23.StuckiG,SanghaO,StuckiS,MichelBA,TyndallA,DickW,
etal.ComparisonoftheWOMAC(WesternOntarioand
McMasterUniversities)osteoarthritisindexandaself-report
formatoftheselfadministeredLequesne-algofunctional
indexinpatientswithkneeandhiposteoarthritis.Osteoarthr
Cartil.1998;6:79–86.
24.SantosJPM,FerreiraDR,SilvaJúniorRA,OliveiraDAAP,
OliveiraRF,FernandesMTP,etal.Avaliac¸ãodafuncionalidade
deidososcomosteartriteutilizandooLowerExtremity
FunctionalScale.TerMan.2012;10:480–5.
25.PuaYH,CowanSM,WrigleyTV,BennellKL.TheLower
ExtremityFunctionalScalecouldbeanalternativetothe
WesternOntarioandMcMasterUniversitiesOsteoarthritis
Indexphysicalfunctionscale.JClinEpidemiol.