w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Investigation
of
depression,
anxiety
and
quality
of
life
in
patients
with
knee
osteoarthritis:
a
comparative
study
夽
Alyne
Hevellen
Ferreira
a,
Priscilla
Brandi
Gomes
Godoy
a,
Nara
Rejane
Cruz
de
Oliveira
b,
Roger
Amorim
Santos
Diniz
c,
Ricardo
Edésio
Amorim
Santos
Diniz
c,
Ricardo
da
Costa
Padovani
d,
Regina
Cláudia
Barbosa
da
Silva
e,∗aDepartamentodePsicologia,UniversidadeFederaldeSãoPaulo,Santos,SP,Brazil
bDepartamentodeCiênciasdoMovimentoHumano,UniversidadeFederaldeSãoPaulo,Santos,SP,Brazil
cUniversidadeMetropolitanadeSantos,Santos,SP,Brazil
dDepartamentodeSaúde,Educac¸ãoeSociedade,UniversidadeFederaldeSãoPaulo,Santos,SP,Brazil
eDepartamentodeBiociências,UniversidadeFederaldeSãoPaulo,Santos,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30July2014 Accepted8March2015 Availableonline3August2015
Keywords:
Osteoarthritis Anxiety Depression Women Qualityoflife
a
b
s
t
r
a
c
t
Introduction:Osteoarthritis(OA)affectsthearticularcartilageandsubchondralbone, com-promisingthejointasawhole.Thekneejointischaracterizedasoneofthemainsites ofinvolvementofOAandthemostsignificantriskfactorsfordevelopingthediseaseare aging,overweightandfemalegender.OAisconsideredoneofthemostfrequentcausesof disability,whichmayaffectthequalityoflifeofthepatients,favoringtheonsetofmental disorders.
Objective:Toinvestigatewhetheranxietyanddepressionsymptomsaremoresignificantin womenwithOA,whencomparedwithwomenwithoutthisdiagnosis,andtowhatextent thisrheumaticdiseaseaffectsthequalityoflifeofthesepatients.
Methods:Thestudyincluded75women,meanage67years;40werediagnosedwithknee OAand35withoutthisdiagnosis.Thefollowinginstrumentswereused:State-TraitAnxiety Inventory(STAI),BeckDepressionInventory(BDI)andSF-36,aqualityoflifequestionnaire.
Results:WomenwithkneeOAhavehigherratesofdepressionandanxietywhencompared tocontrols;inaddition,theyhavealowerqualityoflife.
Conclusion:WebelievethatthetreatmentofpatientswithOAshouldconsiderthe combina-tionofpharmacotherapy,psychotherapy,counselingandfamilysupport,inordertoachieve abetterqualityoflife.
©2015ElsevierEditoraLtda.Allrightsreserved.
夽
StudyconductedattheDepartmentofBiosciences,UniversidadeFederaldeSãoPaulo(Unifesp),Santos,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.C.B.daSilva).
http://dx.doi.org/10.1016/j.rbre.2015.07.004
Investigac¸ão
da
ansiedade,
depressão
e
qualidade
de
vida
em
pacientes
portadores
de
osteoartrite
no
joelho:
um
estudo
comparativo
Palavras-chave:
Osteoartrite Ansiedade Depressão Mulheres Qualidadedevida
r
e
s
u
m
o
Introduc¸ão:Aosteoartrite(OA),artroseouosteoartroseacometeacartilagemhialinaeoosso subcondralecomprometeaarticulac¸ãocomoumtodo.Aarticulac¸ãodojoelho caracteriza-secomoumdosprincipaissítiosdeacometimentodaOA.Oenvelhecimento,osobrepesoe ogênero(prevalênciaemmulheres)sãoosfatoresderiscomaissignificativosparao desen-volvimentodadoenc¸a.AOAéconsideradaumadasmaisfrequentescausasdeincapacidade laborativaepodeafetaraqualidadedevidadeseusportadoresefavoreceraemergênciade transtornosmentais.
Objetivo:Avaliarseossintomasdeansiedadeedepressãosãomaisexpressivosemmulheres comOAquandocomparadoscommulheressemtaldiagnósticoeoquantoessadoenc¸a reumáticacomprometeaqualidadedevidadessespacientes.
Métodos:Participaramdesteestudo75mulheres,commédiade67anos,40comdiagnóstico deOAnojoelhoe35sem.Foramusadososseguintesinstrumentos:InventáriodeAnsiedade Trac¸oeEstado,InventáriodeDepressãodeBeckeSF-36,questionáriodequalidadedevida.
Resultados: Mulheres portadorasde OA no joelho têmníveis maiores de depressão e ansiedade,alémdeapresentarqualidadedevidainferioremcomparac¸ãocomogruposem adoenc¸a.
Conclusão: Acreditamos queo tratamento aosportadores de OA deveria considerar a combinac¸ãodefarmacoterapia,psicoterapia,orientac¸ãoeapoioporpartedosparentese/ou pessoaspróximasparaqueopacientepossaatingirmelhorqualidadedevida.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Osteoarthritis (OA)isthe mostcommon formof arthritis.1 Itcan bedefined as asyndrome that constitutes the final commonpathwayofbiochemical, metabolicand physiolog-icalchangesthatoccur,simultaneously,inarticularcartilage (causinggradualloss),subchondralbone(sclerosis),synovial tissue(inflammation),ligaments,jointcapsuleandmuscles surrounding the affected joint. There is also active bony growthatthejointmargins.2IntheearlystagesofOA, chon-drocytes,synovialcellsandosteoblastsmakeanattemptto repairthelesionsproducedinthecartilageandsubchondral bone.3
Thekneejointischaracterizedasoneofthemainsitesof involvementofOA,beingpresentinabout6%ofadultsabove 30years.2Theprevalenceincreasesto10%inpeopleover60 yearsofage.4OAoccurspredominantlyinwomenaftertheage of40intheperiodofmenopauseandinthepresenceof over-weight,causinglimitationsandadverselyaffectingthequality oflifeofthispopulation.1,2
Rheumatic diseases are characterized mainly by their chronicanddisablingimpairment,causingphysicaldamage thatlimitsthepatient’sfunctionalability,directlyinterfering withhis/herdailyactivities.Inthiscontext,OAemergesasone ofthemostfrequentcausesoflaborincapacityand,therefore, itiscriticaltoevaluatethepsychologicalimpactsthatsucha diseasemaycause,aswellasthequalityoflifeofwomenwith thisdiagnosis.5
Anxietyanddepressivedisorderscanaffectpatientswith adiagnosisofOA,asthechronicpaincausedbythedisease increases the risk ofemergence of these commorbidities.4
Elderly patientswithchronicmedicalillnesses haveshown anincreasedriskofnon-adherencetomedical recommenda-tions,aswellasthemortalityrateassociatedwithdepressive symptoms.6
The anxietydisorder ismore common inpatients with chronicdiseases,beingrelatedtothelimitationsexperienced byelderlypatients.7,8 ConsideringOAasachronic debilitat-ingdisease,itisreasonabletoassumethatitcanbeamajor stressor, favoring the emergence of this disorder. Anxiety, characterizedbyanuncomfortableemotionalstate,manifests itselfaccompaniedbyaseriesofcognitive,emotional, behav-ioralandphysiologicalchanges.Thesechangesofteninclude increasedmotortension,autonomichyperactivity,poor con-centration,distractibility, increasedvigilanceandattention, fearoflosingcontroland ofbeingunabletocope withthe imposedsituation,escapeandavoidancebehaviors, nervous-nessandincreasedirritability.9
Depression isapsychiatricdisorder whoseprevalenceis estimated ataround 3–5% of the generalpopulation.7 The mosttypicalfeaturesofdepressionare:prominenceoffeelings ofsadnessoremptiness,lossofabilitytoexperiencepleasure ingeneralactivitiesandreducedinterestintheenvironment. Depression may be associated with fatigue and excessive tiredness,aswellaswithpsychomotorchanges.6
Table1–Descriptivemeasuresofage.
Group Age
Withosteoarthritis
Mean 68.36
Standarddeviation 9.92
Withoutosteoarthritis
Mean 65.91
Standarddeviation 9.12
Descriptivelevel 0.276
Descriptive means of age of groups with and without knee osteoarthritis.
Methods
Thisisacross-sectional, quantitativestudy.Thestudywas approvedbytheResearchEthicsCommitteeofthe Universi-dadeFederaldeSãoPaulo(protocol10894/2012).
Sample
Thestudyincluded75womenaged50–72years.Ofthistotal, 40womenhadadiagnosisofkneeOAaccordingtothe Amer-icanCollegeofRheumatologycriteria,11and35werehealthy, asymptomatic subjects, matched by gender and age. The meanageofthegroupwithOAwas68years,whilethemean ageinthegroupwithoutOAwas65years(Table1).OApatients wereseenatanoutpatientclinicofauniversityinthecityof Santos/SP.Theywereselectedthroughasurveyconductedby thelocalmedicalteam,coordinatedbyarheumatologist.The patientswerebeingtreatedwithNSAIDsandphysiotherapy foratleast1yearandatmostfor2years.The35womenofthe controlgroupattendedtotheUniversidadeAbertadaTerceira Idade–UnATI,campusSantos,UNIFESP.
Instruments
Theinstrumentsusedindatacollectionwere:
State-TraitAnxietyInventory(STAI)12
TheSTAIcomprisestwoscales,eachconsistingof20items, assessingstate (STAI-S) and trait(STAI-T) levelsof anxiety respectively.ItisaLikertscale-typeinstrument,withscores rangingfrom1(almostnever)to4(almostalways)forSTAI-T, andfrom1(notatall)to4(verymuch)forSTAI-S.
BeckDepressionInventory13
Thisisaself-reportedscale whichcontains 21items, each with four alternatives, with scores ascribed of 0, 1, 2 or 3. BDI items relate to cognitive-affective symptoms and somatic/performancesensations.
Medicaloutcomesstudy36-itemShort-FormHealthSurvey (SF-36)14
Thisinstrumentconsistsof36itemsthatassessthequalityof lifeovereightsections,rangingfrom0to100,where0=worst and 100=best,foreach domain,namely: (1)physical func-tioning(10items);(2)rolelimitationsduetophysicalhealth
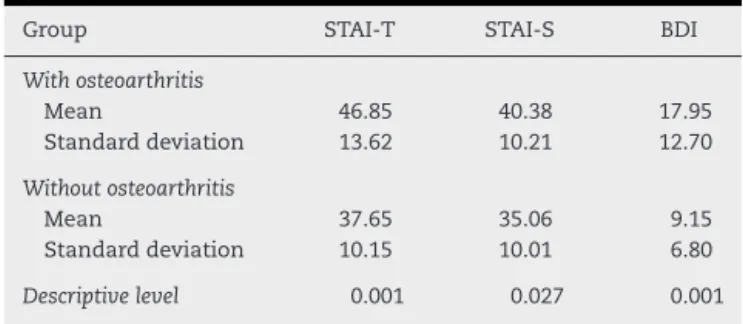
Table2–PerformanceinState-TraitAnxietyInventory (STAI)andBeckDepressionInventory.
Group STAI-T STAI-S BDI
Withosteoarthritis
Mean 46.85 40.38 17.95
Standarddeviation 13.62 10.21 12.70
Withoutosteoarthritis
Mean 37.65 35.06 9.15
Standarddeviation 10.15 10.01 6.80
Descriptivelevel 0.001 0.027 0.001
STAI,State-TraitAnxietyInventory;STAI-S,anxiety-state;STAI-T, anxiety-trait;BDI,BeckDepressionInventory.
(four items); (3) bodily pain (two items); (4) generalhealth status(fiveitems);(5)vitality(fouritems);(6)socialrole func-tioning (two items); (7) role limitations due to emotional problems(threeitems);(8)mentalhealth(fiveitems).
Procedures
Datacollectionwasperformedatanofficeintheoutpatient clinicorinanotherplacedefinedbytheparticipantin agree-ment withthe investigator. The instruments were applied individually,inasinglesession,lastingonaverage30min.
Analysis
Adescriptive analysiswasperformedinordertostudy the behavior ofgroupswith andwithout OA,for each variable ofinterest:StateTraitAnxietyInventory(STAI),Beck Depres-sion Inventory (BDI) and Medical Outcomes Study 36-item short-Form HealthSurvey(SF-36).Student’st-testfor unre-latedsampleswasusedtocomparethetwogroups,regarding thesevariables.Differenceswereconsideredsignificantwhen p≤0.05.
Results
In Table2onecansee thatthe patientsinthe groupwith
OAhavehigherratesinallvariablesstudied.Itisworth not-ingthatSTAIconsidersasmoreanxiousthosepeoplewhose scoresarehigheronthequestionnaire.Ontheotherhand,BDI scoresbetween 0–9are consideredas nodepression,10–18 asmilddepression,19–29asmoderatedepression,30–63as severedepression.14
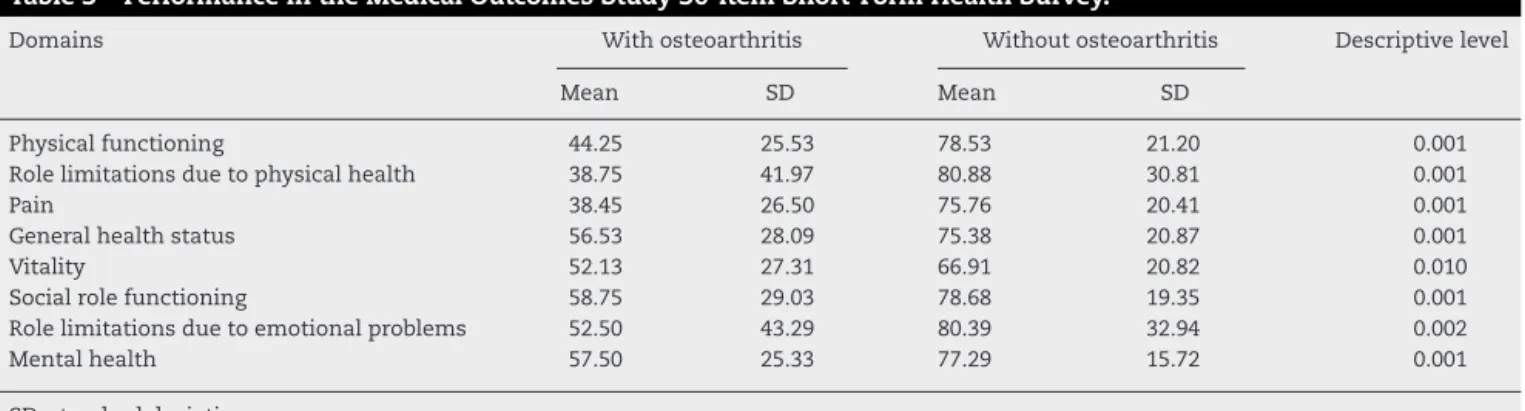
InTable3,onecanseethatpatientswithOAhada
signif-icantlylowerscoreinalldomainsexaminedbySF-36,when comparedwiththescoresofthecontrolgroup.
Discussion
Table3–PerformanceintheMedicalOutcomesStudy36-itemShort-FormHealthSurvey.
Domains Withosteoarthritis Withoutosteoarthritis Descriptivelevel
Mean SD Mean SD
Physicalfunctioning 44.25 25.53 78.53 21.20 0.001
Rolelimitationsduetophysicalhealth 38.75 41.97 80.88 30.81 0.001
Pain 38.45 26.50 75.76 20.41 0.001
Generalhealthstatus 56.53 28.09 75.38 20.87 0.001
Vitality 52.13 27.31 66.91 20.82 0.010
Socialrolefunctioning 58.75 29.03 78.68 19.35 0.001
Rolelimitationsduetoemotionalproblems 52.50 43.29 80.39 32.94 0.002
Mentalhealth 57.50 25.33 77.29 15.72 0.001
SD,standarddeviation.
Depressionintheelderlymayemergeasaconsequence ofgeneral medical illnesses, especiallythose, such as OA, thatcauseprolongedsuffering,leadingthepatientto physi-caldisabilityandlossofautonomy.15Inthisstudy,BDIresults demonstratethattheimpactofdepressionisimportant,since depressedindividualsaremorelikelytoreportchronicpain, orpainofgreaterintensity.Thisfactcanbeacomplicating factorintheprocessoftreatmentadherence,andmaystill increasethe perception ofpain.16 Thedepressive disorder, whenassociatedwithphysicalillness,cancause the emer-genceofanxietysymptoms.8 Inthiscontext,theresultsof thisstudycorroboratethisfinding.
Inadditiontodepressionandanxiety,painandits impli-cationson the physicaland mental state of patients with OAappeartobeimportantcomponents,affectingdecisively thequalityoflifeofthesepatients.Theresultsofthisstudy indicate a significant worsening in the domains of SF-36 instrument.This trendmanifested itself bothin the areas mostdirectlyrelatedtophysicalhealth(bodilypain,physical functioning,role limitationsduetophysicalhealth,vitality and generalhealth state)and in those domains related to socialaspectsandpsychologicalhealth(rolelimitationsdue toemotionalproblemsandmentalhealth).
Indomainsrelatedtophysicalhealth,itwasfoundthat thegroupwithOAhadsignificantlyhigherlevelsofbodypain comparedtothecontrolgroup,negativelyaffectingthe qual-ityoflife.Regardingthedomainphysicalfunctioning,which referstotheabilityofanindividualtoliveindependentlyin his/hercommunity,adecreasewasobservedinthegroupwith OA.Astudy indicativeofthequalityoflifeinpatientswith chronicrheumaticdiseases5showedthatOAischaracterized bybeing particularly debilitating, causing physicaldamage thataffectsthefunctionalabilityofthepatient.Theresults ofthisstudyalsocorroboratesuchclaims.Findingsofamore recentstudy15alsoshowthatpatientswithchronicpainand withdepressionexhibitahighdegreeofphysicaldisability– afindingwhichwasalsoevidencedinthisstudy.Theresults observedinthedomainrolelimitationsduetophysicalhealth indicatedascoretwicehigherinthegroupwithOA,compared tothecontrolgroup.
Thedomainvitalitywasevaluatedfromtheresponsesof thevolunteers,abouthowlongtheyfeltexhausted,fatigued andwithenergyandvigortocarryoutactivities.Thegroup withOAreportedfeelingmorefatigueandtirednessandlower
energyandvigortocarryoutactivities,demonstratingaloss in this domain.The same instrument also assessedsocial aspects,basedonquestionsabouthowandforhowlongthe physicalhealthinfluencedthedevelopmentofsocial activi-ties.
Painanddifficultyindailylifeactivities,physicaldisability andrestrictionofmobilityandsocialintegrationgeneratedby disabilitiescanincreaseanxietyanddiscouragement,17 inten-sifying theeffectsofOAand leadingtoaworseningofthe patient’sperceptionregardinghis/hermentalhealth.
Itis interestingtonote that the resultofan inferential analysis ofcomparisonbetween the two groups(with and without OA)showedsignificant differencesforallvariables investigatedinthisstudy,encompassingphysical,socialand emotionaldimensions.Theexceptionwasmadetothe vari-able“age”,inwhichthe differencebetweenthetwogroups wasnotsignificant.Thisfindingwasduetothefactthatthe minimumageof50waschosenforthecompositionofthe samples.TheresultsrevealedthatthegroupwithOAshowed declinesinallothervariables,whencomparedtothecontrol group.
Conclusion
Together,theresultsobservedinthisstudyshowedthat symp-toms of anxiety and depression were more significant in womenwithOAcomparedtowomenwithoutsucha diagno-sis,emphasizingthenegativeimpactthatthisdiseasecauses inthepsychicdomainandqualityoflifeofthepatients.In thiscontext,itisbelievedthatthetreatmentofpatientswith OA shouldconsider anumberofapproaches,involving the combinationofpharmacotherapy,psychotherapy,counseling andfamilysupport,sothatthesepatientscanachievea bet-terqualityoflife.Therefore,itwouldbecriticaltoinvolvea supportnetwork,includingprofessionalsfromdifferentareas suchasphysicians,psychologists,occupationaltherapistsand socialworkers.
Conflicts
of
interest
r
e
f
e
r
e
n
c
e
s
1. LopesJuniorOV,InacioAM.Useofglucosamineand
chondroitintotreatosteoarthritis:areviewoftheliterature.
RevBrasOrtop.2013;48:300–6.
2. TakahashiF,LadeiraJP,LimaAM.Osteoartrite.In:Ribeiro
ACM,TakahashiF,editors.Principaistemasemreumatologia
pararesidênciamédica.2aed.SãoPaulo:Medcel;2006.p.
59–70.
3. VanucciAB,SilvaL,LatorreLC,IkeharaZerbiniCAF.Como
diagnosticaretratarosteoartose.RBM.2000;57:35–46.
4. SantosNGB,FigueiredoNetoEM,ArêasGPT,ArêasFZS,Leite
HR,FerreiraMAC,etal.Capacidadefuncionalequalidadede
vidaemidososcomosteoartrosenomunicípiodeCoari(AM).
RevPesqFis.2012;2:107–20.
5. CiconelliRM.Avaliac¸ãodaqualidadedevidaemdoenc¸as
reumáticas.SinopseReumatológica.1999;2:1–4.
6. VismariL,AlvesGJ,PalermoNetoJ.Depressão,antidpressivos
esistemaimune:umnovoolharsobreumvelhoproblema.
RevPsiquiatrClín.2008;35:196–204.
7. TengCT,HumesEC,DemetrioFN.Depressãoecomorbidades
clínicas.RevPsiquiatrClín.2005;32:149–59.
8. Valenc¸aAM,FreireR,SantosLM,SenaIM,CampinhoJL,
MartuscelloNetoC,etal.Transtornosdeansiedadee
depressãoempacientesdeambulatóriodeclínicamédica.
RBM.2008;65:12–7.
9. ClarkDA,BeckAT.Terapiacognitivaparaostranstornosde
ansiedade:ciênciaeprática.PortoAlegre:Artmed;2012.
10.OliveiraP,MonteiroP,CoutinhoM,SalvadorMJ,CostaME,
MalcataAB.Qualidadedevidaevivênciadadorcrônicanas
doenc¸asreumáticas.ActaReumatolPort.2009;34:
511–9.
11.AltmanR,AschE,BlochD,BoleG,BorensteinD,BrandtK,
etal.Developmentofcriteriafortheclassificationand
reportingofosteoarthritis.Classificationofosteoarthritisof
theknee.ArthritisRheum.1986;29:1039–49.
12.SpilbergerCD,GorsuchRL,LusheneRE.Inventáriode
annsiedadetrac¸o-estado.RiodeJaneiro:CEPA;1979.
13.BeckAT.InventáriodedepressãodeBeck.SãoPaulo:Casado
Psicólogo;2001.
14.CiconelliRM.Traduc¸ãoparaoportuguêsevalidac¸ãodo
questionáriogenéricodeavaliac¸ãodequalidadedevida
MedicalOutcomesStudy36-ItemShort-FormHealthSurvey
(SF-36)[tese].SãoPaulo:UniversidadeFederaldeSãoPaulo,
EscolaPaulistadeMedicina;1997.
15.PimentaFAP,SimilFF,TôrresHOG,AmaralCFS,RezendeCF,
CoelhoTO,etal.Avaliac¸ãodaqualidadedevidade
aposentadoscomautilizac¸ãodoquestionárioSf-36.Revista
AssocMedBras.2008;54:55–60.
16.LeiteAA,CostaAJG,LimaBAM,PadilhaAVL,AlbuqueruqeEC,
MarquesCDL.Comorbidadesempacientescomosteoartrite:
frequênciaeimpactonadorenafunc¸ãofísica.RevBras
Reumatol.2011;51:118–23.
17.BerberJSS,KupekE,BerberSC.Prevalênciadedepressãoe
suarelac¸ãocomaqualidadedevidaempacientescom
síndromedafibromialgia.RevBrasReumatol.2005;45: