Exercising Body and Mind: An Integrated Approach to Functional
Independence in Hospitalized Older People
Alison M. Mudge, MB, BS (Hons),
Andrea J. Giebel, BPhty (Hons), M App Mgt (Hlth),
wand
Alison J. Cutler, MB, BS
OBJECTIVES: To evaluate the effect of a structured, multi-component, early rehabilitation program on functional status, delirium, and discharge outcomes of older acute medical inpatients.
DESIGN: Prospective controlled trial with blinded out-come evaluation.
SETTING: Internal medicine service of a metropolitan ter-tiary teaching hospital in Brisbane, Australia.
PARTICIPANTS: One hundred twenty-four consecutive inpatients aged 65 and older admitted from the emergency department to control or intervention medical ward. Ex-clusions included patients completely dependent before ad-mission or admitted from a nursing home, patients too ill to participate or terminally ill, and patients with length of stay less than 72 hours.
INTERVENTION: Early physiotherapy review with pro-vision of an individualized graduated exercise program and activity diary, progressive encouragement of functional in-dependence by nursing staff and other members of the multidisciplinary team, and cognitive stimulation sessions.
MEASUREMENTS: Modified Barthel Index (MBI) at ad-mission and discharge, timed up-and-go at adad-mission and discharge, incidence of delirium and falls, measured activ-ity, length of hospital stay, discharge destination, 30-day readmission rate.
RESULTS: Intervention and control participants were well matched in terms of age, sex, diagnosis, and functional sta-tus. The intervention group had greater improvement in functional status than the control group, with a median MBI improvement of 8.5 versus 3.5 points (P5.03). In the
intervention group, there was a reduction in delirium (19.4% vs 35.5%, P5.04) and a trend to reduced falls
(4.8% vs 11.3%,P5.19). Length of stay, timed up-and-go,
discharge destination, and readmissions did not differ be-tween the groups.
CONCLUSION: This intervention was effective in im-proving function in a vulnerable patient group. J Am Geriatr Soc 56:630–635, 2008.
Key words: patient care team; hospitalization; exercise; activities of daily living; delirium
O
lder patients hospitalized with acute illnesses are at high risk of morbidity related to deterioration in mo-bility, cognition, and activities of daily living (ADLs). One-third to one-half of older patients are discharged from an acute medical hospitalization with greater dependency in their basic self-care activities than they had before the acute illness,1–3and 15% to 42% experience delirium.4,5Some ofthis decline results directly from the acute illness, but new decline may also result from the hospital environment.6
Delirium and functional decline both contribute to adverse outcomes of hospitalization, including death, falls, pro-longed hospitalizations, and discharge to institutional care.2,4
Poor mobilizing during hospitalization has been rec-ognized as a risk for hospital-related functional decline.7
The use of physical or medical restraints that impede mo-bility are also recognized risk factors for delirium.8Other
barriers to mobility include bed rest orders, unclear phy-sician orders regarding mobility, inadequate referral for physiotherapy assessment and support, limited nursing time, and concerns about potential falls risks.9,10
Two published studies11,12attempted to reduce
func-tional decline by providing a graded exercise program for hospitalized elderly patients using an allied health assistant but have demonstrated limited functional benefits. A recent systematic review13suggested that benefits may result from
a multidisciplinary approach to care that includes exercise protocols delivered by nursing or allied health staff. A mul-tidisciplinary model including exercise, cognitive stimula-tion, and nonpharmacological sleep protocols has also demonstrated benefits in reducing delirium.5
A multidisciplinary care model for general medical in-patients that was previously implemented demonstrated significant reductions in functional decline and inpatient
Address correspondence to Dr. Alison Mudge, Staff Specialist, Internal Medicine Department, 3rd floor James Mayne Building, Royal Brisbane and Women’s Hospital, Butterfield St, Herston, Brisbane, Queensland 4029, Australia. E-mail: [email protected]
DOI: 10.1111/j.1532-5415.2007.01607.x From the Departments ofInternal Medicine andw
Physiotherapy, Royal Brisbane and Women’s Hospital, Brisbane, Australia.
JAGS 56:630–635, 2008
r2008, Copyright the Authors
mortality,14although 6% to 8% of patients aged 70 and
older still declined during their hospitalization. The current study was designed to determine whether a focused pro-gram of physical exercise and cognitive stimulation, deliv-ered and supported by the existing multidisciplinary team, could further improve functional outcomes in older, acutely hospitalized medical patients.
METHODS Setting
The study was undertaken within the internal medicine de-partment of a metropolitan, tertiary public teaching hospi-tal in Brisbane, Australia. Five general medical units admit approximately 5,000 acute inpatients per year. Almost all patients are admitted from the hospital emergency depart-ment, with some referrals from intensive care or other spe-cialty units. Although subspespe-cialty units often provide care for patients with defined single-system disease, a strong tradition of general medicine means a diverse case mix and a prevalence of patients with multiple comorbidities, com-plex discharge planning needs, and diagnostic uncertainty. Each general medical unit consists of two medical teams (specialist physician, trainee registrar, and intern) and a consistent, unit-based multidisciplinary team, as de-scribed previously.14Patients are admitted on a cyclical
ro-tating roster, with central bed allocation based on bed availability. The five units nominally admit patients to four medical wards, including a Medical Assessment and Plan-ning Unit. High rates of access block often lead to pro-longed stays in the emergency department short-stay ward and other ‘‘flexible’’ bed capacity or ‘‘outlying’’ in other wards, including surgical and oncology wards. This may lead to frequent ward changes. Approximately two-thirds of patients are aged 65 and older. The hospital also has a geriatric rehabilitation unit, a stroke unit, and an extended (postacute) care unit but no acute care geriatric unit. There are limited formal rehabilitation and subacute beds avail-able in the district, and inpatient beds are therefore used for early rehabilitation; approximately 20% of bed days in in-ternal medicine are considered to be rehabilitation or con-valescence.
The proposed model required significant ward culture change, as well as patient-level intervention. In an environ-ment of significant access block and fixed rotating rosters, patient-level randomization was not practicable. The inter-vention was therefore evaluated using one medical ward as a control ward and one as an intervention ward. Previous research within the department suggested similar patient distribution between medical units and wards because of the rotating admissions roster.14The control and
interven-tion wards were on separate floors of the hospital and rarely admitted each other’s ‘‘home’’ patients, so the risk of con-tamination was considered small. Staff delivering the inter-vention were aware of the study hypothesis.
Participants
The study recruited participants over a 10-week period from August to October 2006. Consecutive patients aged 65 and older who were admitted to an internal medicine unit for at least 3 days and who received at least some of
their care on the designated intervention or control ward were eligible for inclusion in the study. The project officer identified prospectively all patients who might meet these criteria (aged 65 and eligible for admission to the control or intervention ward based on their unit allocation). Pa-tients were considered ineligible if they were already fully dependent before admission or came from a high-level res-idential care facility or were medically too unstable for early assessment or terminally ill. Patients were excluded if they were discharged or transferred within 72 hours, died in the hospital, or did not gain admission to the study wards dur-ing their admission. The Royal Brisbane and Women’s Hospital Human Research Ethics Committee approved the study. Individual patient consent was not required in view of the low risk and burden for participants, potential for public health benefits, and the desire to include participants with limited capacity to consent.
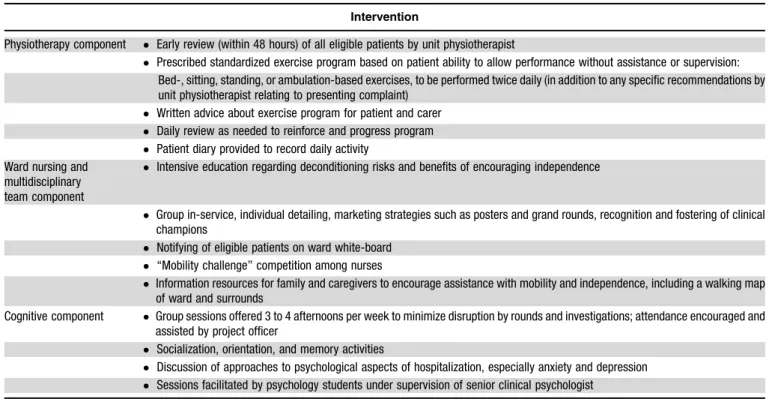
Intervention
The intervention consisted of three components: a gradu-ated exercise program prescribed and supervised by the unit physiotherapist; education of ward and multidisciplinary team staff, patients, and caregivers to actively encourage mobility and functional independence; and a cognitive in-tervention delivered in groups by psychology students su-pervised by a senior psychologist. Individual intervention components are described in Table 1.
Control ward patients received usual care from the multidisciplinary care team, including daily discussion of patient progress and discharge plan, and referral to the team physiotherapist or occupational therapist by medical or nursing staff if there were concerns about mobility or func-tion.
Outcomes
The primary outcome was change in functional status be-tween admission and discharge, measured using the mod-ified Barthel index (MBI).15Performance on stairs was not
evaluated, giving a score range of 0 to 90 (highest score indicating maximal independence in ADLs). A single, trained occupational therapist unaware of the study hy-pothesis and patient allocation performed evaluation of function within 48 hours of admission and of discharge.
Secondary outcomes were change in mobility between admission and discharge and delirium. The same blinded therapist assessor assessed mobility at admission and dis-charge using the timed up-and-go test.16A physician trainee
blinded to intervention group identified delirium according to chart review using validated methodology.17Other
out-comes included length of stay, incidence of falls, discharge destination, and readmission within 30 days. Trained, blinded research staff abstracted these outcomes, and pa-tient demographic and disease characteristics, from photo-copied chart extracts from which the principal investigator removed all references to ward or medical unit.
Patient activity on the ward was measured using direct observation using methods similar to those described pre-viously.18The project manager (who was aware of the
Patients who would be considered eligible for the interven-tion were observed for 2- to 3-hour periods at varying times of the morning and afternoon shift over a 7-day period. A total of 76 patient-hours of observation were undertaken during each observation period, divided equally between the control and intervention ward. Time spent in bed, seat-ed, standing, and walking was recorded.
Analysis
All analyses were according to intention to treat. Patient characteristics in the control and intervention groups were summarized using proportions for categorical variables and means (or medians for nonnormally distributed character-istics) for continuous variables. Intergroup comparison of categorical variables used contingency tables and the chi-square test; continuous variables were compared between the groups using the Studentt-test for normally distributed variables and the Mann-WhitneyU-test for others.
Change in functional status between admission and discharge (MBI score at discharge minus MBI score at ad-mission) was analyzed as a continuous variable using the Mann-WhitneyU-test. For additional descriptive purposes, scores were classified as better, unchanged, or worse at dis-charge compared with admission. The timed up-and-go score had a highly skewed distribution and was analyzed as a categorical variable (o20, 20–40, 440 seconds).19 All analyses were conducted using SPSS version 14.0 statistical software (SPSS Inc., Chicago, IL). A P-value of .05 was considered significant in all analyses.
RESULTS
During the 10-week study period, 377 patients aged 65 and older were admitted from the emergency department to medical units that admitted to the control or intervention
ward. Of these, 104 (27.6%) were discharged or transferred within 72 hours, and a further 45 (11.9%) were outlier patients (did not gain admission to a study ward). Details of
Table 1. Intervention Components
Intervention
Physiotherapy component Early review (within 48 hours) of all eligible patients by unit physiotherapist
Prescribed standardized exercise program based on patient ability to allow performance without assistance or supervision:
Bed-, sitting, standing, or ambulation-based exercises, to be performed twice daily (in addition to any specific recommendations by unit physiotherapist relating to presenting complaint)
Written advice about exercise program for patient and carer
Daily review as needed to reinforce and progress program
Patient diary provided to record daily activity
Ward nursing and multidisciplinary team component
Intensive education regarding deconditioning risks and benefits of encouraging independence
Group in-service, individual detailing, marketing strategies such as posters and grand rounds, recognition and fostering of clinical champions
Notifying of eligible patients on ward white-board
‘‘Mobility challenge’’ competition among nurses
Information resources for family and caregivers to encourage assistance with mobility and independence, including a walking map of ward and surrounds
Cognitive component Group sessions offered 3 to 4 afternoons per week to minimize disruption by rounds and investigations; attendance encouraged and assisted by project officer
Socialization, orientation, and memory activities
Discussion of approaches to psychological aspects of hospitalization, especially anxiety and depression
Sessions facilitated by psychology students under supervision of senior clinical psychologist
377 patients aged ≥65, potential admissions to control or
intervention units
96 screened in intervention units 21 discharge/transfer <72h 9 remained off home ward 4 died
103 screened in control units 19 discharge/transfer <72h 16 remained off home ward 6 died
178 ineligible for screening 44 fully dependent 34 medically unstable 9 palliative
64 discharge/transfer <72h 20 outside home ward
Intervention group n = 62
Control group n = 62
eligibility and patient allocation are given in Figure 1. Overall, 124 patients were eligible and agreed to the study. These patients were equally distributed between the inter-vention and control ward.
Complete outcome data were available on all study patients. Baseline MBI was measured within 48 hours of admission in 72% of patients and within 24 hours of dis-charge in 97.6%; there was no difference between groups with regard to timing of assessments. Patients in the control and intervention groups were well matched for age, sex, comorbidities, and baseline functional status (Table 2), al-though more patients in the control group came from as-sisted living (low-level residential care).
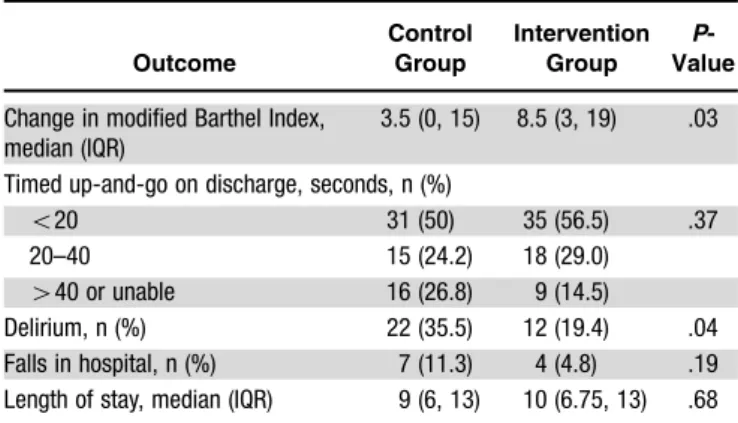
Table 3 summarizes the major findings. The interven-tion group showed a small but significant improvement in functional status at discharge, with a median change in MBI score of 8.5 (interquartile range (IQR) 3–19), versus 3.5 (IQR 0–15) in the control group (P5.03). In the
interven-tion group, one patient (1.6%) had in-hospital decline, six (9.7%) remained stable, and 55 (88.7%) improved; in the control group, four (6.5%) declined, 15 (24.2%) were sta-ble, and 43 (69.4%) improved (P5.03). Improvement of
5 points or more on the MBI was seen in 41 (66.1%) of the intervention group, compared with only 21 (33.9%) of the control group.
Timed up-and-go scores were not significantly different between the groups. Scores improved during the admission
in both groups with 35 (56.5%) intervention patients and 31 (50%) control patients, respectively, achieving a score of less than 20 seconds at discharge, compared with 24 (38.7%) and 23 (37.1%) at admission. Only 24 (38.7%) intervention patients required a walking aid at discharge from hospital, compared with 33 (53.8%) control patients (P5.11).
The overall occurrence of delirium was lower in the intervention group, occurring in 12 (19.4%) patients, com-pared with 22 (35.5%) in the control group (P5.04). There
was a trend to a lower incidence of new delirium during hospital stay (8.1% vs 14.5%,P5.26) and to fewer falls in
the intervention group (4.8% vs 11.3%P5.19).
Although the two groups were similar in terms of most participant characteristics, the control group had a greater number of residents in low-level residential care and a higher rate of prevalent delirium (delirium at the time of hospital presentation). To adjust for these differences, lo-gistic regression models for the outcome of functional im-provement (higher MBI score at discharge than on admission) during hospitalization were produced, adjust-ing for age, sex, comorbidity score, length of stay, prevalent delirium, and place of residence. Functional improvement was predicted by membership in the intervention group (odds ratio (OR)53.8, 95% confidence interval
(CI)51.3–11.0,P5.02) and by an admission MBI score
of less than 71 (OR54.2, 95% CI51.2–14.2, P5.02).
The other confounders did not contribute significantly to the model.
The intervention did not significantly affect discharge destination. Fifty-one (85%) intervention patients and 50 (83%) control patients returned to their previous living ar-rangements, five intervention and seven control patients required new residential care placement, and six interven-tion and three control patients were transferred for further rehabilitation. There was no significant difference between the groups in length of stay (intervention group median stay 10 days vs 9 days in control) or 30-day readmissions rate (17.7% in the intervention group, 19.4% in control).
In the intervention group, initial physiotherapist as-sessment and institution of an appropriate exercise program was completed in a median of 2 days (IQR 0–4 days). As expected, more patients in the intervention group had a physiotherapist visit recorded (96.8% vs 82.3%), but the mean number of physiotherapist visits per patient were not
Table 2. Participant Characteristics
Characteristic
Control Intervention P -Value n562 n562
Age, meanSD 82.4 (7.4) 81.7 (7.8) .58 Female, n (%) 37 (59.7) 35 (56.5) .72 Living arrangements, n (%)
Community alone 33 (53.2) 25 (40.3) .005 Community with others 21 (33.9) 36 (58.1) Low-level assisted living 8 (12.9) 1 (1.6) Comorbidity score, median (IQR) 2 (1,4) 2 (1,4) .77 Medications, n, meanSD 6.6 (3.6) 6.4 (3.9) .73 Recorded diagnosis of dementia, n (%) 5 (8.1) 6 (9.7) .75 Admission in previous 3 months, n (%) 15 (24.2) 19 (30.6) .42 Diagnosis, n (%)
Cardiovascular 8 (12.9) 11 (17.7) Respiratory 14 (22.6) 12 (19.4) Neurological 6 (9.7) 6 (9.7) Infectious 12 (19.4) 11 (17.7) Fall or fracture 5 (8.1) 9 (14.5) Other 17 (27.4) 13 (21.0) Modified Barthel Index on admission,
median (IQR)
72.5 (56, 85) 71.5 (58, 83) .89
Timed up and go score on admission, seconds, n (%)
o20 23 (37.1) 24 (38.7) .36 20–40 17 (27.4) 21 (33.9)
440 13 (21.0) 6 (9.7)
Unable to complete 9 (14.5) 11 (17.7) Days to home ward, median (IQR) 3.0 (1.75, 4.0) 2.0 (2.0, 4.0) .98
SD5standard deviation; IQR5interquartile range.
Table 3. Major Outcomes
Outcome
Control Group
Intervention Group
P -Value
Change in modified Barthel Index, median (IQR)
3.5 (0, 15) 8.5 (3, 19) .03
Timed up-and-go on discharge, seconds, n (%)
o20 31 (50) 35 (56.5) .37 20–40 15 (24.2) 18 (29.0)
440 or unable 16 (26.8) 9 (14.5)
Delirium, n (%) 22 (35.5) 12 (19.4) .04 Falls in hospital, n (%) 7 (11.3) 4 (4.8) .19 Length of stay, median (IQR) 9 (6, 13) 10 (6.75, 13) .68
significantly different between the two groups (3.21 vs 3.37, P5.53). Ninety-two percent of patients in the intervention
group received an exercise diary and made some record of exercise; one-third completed their diary every day. Fifty percent of the intervention group attended at least one cog-nitive group session. Nonattendance was mainly attributed to clashes with patient investigations, delays in transferring to the home ward where the intervention was offered, and patient fatigue.
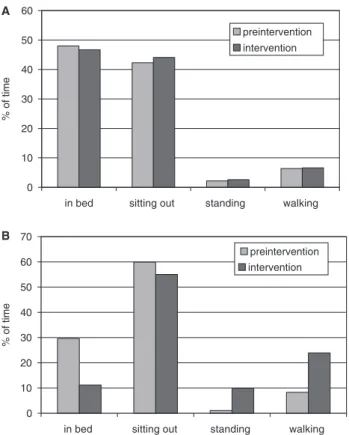
Observation of patient mobility in 34 elderly patients before the trial showed low levels of mobility on both trial wards, with less than 10% of observed time spent standing or walking. During the intervention, patients on the inter-vention ward were much less likely to be observed in bed and spent significantly more time standing or walking with-in the ward (Figure 2B). More hallway walkwith-ing was ob-served and occurred independently, as well as with a range of people, including families, nursing staff, and physiother-apists. Mobility patterns on the control ward were un-changed (Figure 2A).
DISCUSSION
These results suggest that a structured multidisciplinary in-tervention targeting physical and cognitive aspects of func-tioning can reduce the decline in functional status commonly seen during acute hospitalization of elderly pa-tients. The measured difference in improvement in the MBI
of 5 points translates clinically into independence in one or more additional self-care activities. This was achieved with-out an increase in falls risk, and delirium may also have been reduced. There was no measurable change in length of stay or discharge destination in this study, but the sample esti-mates of these variables indicate that the study was signifi-cantly underpowered for these secondary outcomes, and a larger trial would be required to provide confident estimates. A similar approach was used in the Hospital Elder Life Program model in older medical patients in the United States who were considered at high risk of developing delirium.5
This model included early mobilization, in-hospital exercise, and daily reorientation and cognitive stimulation, as well as protocols directed at vision, hearing, adequate hydration, and nonpharmacological sleep enhancement. A controlled trial demonstrated a significant reduction in new delirium but no significant change in ADL function. Other multidisciplin-ary models including an emphasis on mobility have reduced functional decline. For example, an Acute Care for Elders unit demonstrated a reduction in ADL decline between hos-pital admission and discharge and less need for new residen-tial care placement.20Delirium was not measured.
In contrast, trials of exercise interventions added to usual ward care appear to have had less influence on func-tional outcomes. A recent Australian trial of graded inpa-tient exercise and mobilization12 showed limited benefits,
with a trend to improvement in timed up-and-go scores but no improvement in the MBI. Multivariate analysis suggest-ed an improvement in MBI in patients with an admission MBI score less than 70 but no benefit in more-independent patients. Delirium was not measured. An allied health as-sistant delivered the intervention without attempts to alter ward or team culture to incorporate mobilization into the patients’ routine. Similarly, a previous study11evaluated an
exercise program for hospitalized older medical and surgi-cal patients that included a postdischarge home-based ex-ercise program. Allied health assistants also administered this intervention, which resulted in improvement in the number of instrumental ADLs performed by the interven-tion group at 1 month postdischarge but no other signifi-cant improvements in function or mobility.
The current intervention may have been more effective at reducing functional decline than previous models for several reasons. Broad patient targeting simplified the pro-gram. The cognitive and physical interventions reinforced one another; the cognitive groups provided a walking ‘‘des-tination’’ and also encouraged greater social interaction between patients, which in turn encouraged patients away from their bedside. Perhaps most importantly, the program had a strong, multidisciplinary leadership and implemen-tation team so that ambulation and mobility became ev-eryone’s business.6The intervention engaged the members
of the existing multidisciplinary team and nursing staff, who were able to reinforce the prescribed exercise regime with encouragement of general mobility.
Of particular interest is the observation that there was no measurable increase in physiotherapy occasions of ser-vice; the intervention group tended to have earlier and less-frequent review, perhaps because other team members, caregivers, and the patients themselves were more confident mobilizing without formal physiotherapy assistance. The previously established multidisciplinary model has allowed
0 10 20 30 40 50 60
A
B
in bed sitting out standing walking
% of time
preintervention
intervention
0 10 20 30 40 50 60 70
in bed sitting out standing walking
% of time
preintervention intervention
relatively generous allied health resourcing, and the model may have greater resource implications to implement else-where, although in view of the high level of physiotherapy review in the control group, it is likely that this study un-derestimated the potential benefits of this type of interven-tion in other environments. Other studies have not reported the proportion of control group patients receiving ‘‘usual’’ physiotherapy.
The study has some weaknesses. It was underpowered for secondary outcomes such as delirium, falls, and length of stay, although the results seen in the first two measures are encouraging, in particular, allaying fears that greater mobility is risky in frail patients.21A number of potentially
eligible patients were excluded, because they were not ad-mitted to the ‘‘home’’ medical ward. The Royal Brisbane and Women’s Hospital, like many others, is subject to sig-nificant access block; median time to admission to the home medical ward was 3 days for intervention and control pa-tients. Although most (71%) intervention patients received their exercise program by day 2, the full benefits of the ward-based and cognitive intervention may not have been realized because of these delays. In particular, only half of the intervention participants attended the cognitive group sessions. As with all multicomponent interventions, it is difficult to ascribe the observed benefits to individual ele-ments.
The study design also demonstrates a number of strengths. Although it was not randomized, patient groups were well matched and were representative of patients at risk of functional decline in the hospital. A range of clearly defined outcomes was measured, and data collection was complete on eligible patients. Mobility levels on the ward, which reflect changes in healthcare provider and patient behavior and provide a plausible mechanism for the ob-served outcomes, were also directly obob-served.
In summary, this article describes a simple and effective multicomponent intervention targeting physical and cogni-tive risk factors for functional decline in hospitalized older patients. The intervention did not require detailed screening for suitable patients or major changes to workforce in the environment and should be possible to replicate in other units or hospitals caring for elderly patients with multidis-ciplinary teams.
ACKNOWLEDGMENTS
The authors are grateful for the assistance of Julie Hul-combe, Kate Mason, and Dr. Charles Denaro for executive support; Carly Mansbridge for data collection; Anne Clair and the University of Queensland School of Psychology students for coordinating the psychology component; Dr. Shanthi Kanagarajah, Toni Houghton, Nathan McGrath, Kath Richter, Sandra Watson, Tracey Beaton, Elaine Un-kles, and Karen Gilbert for assisting on the steering com-mittee; and the committed staff of the medical wards.
Conflict of Interest: This study was supported by a grant from Queensland Health under the Strengthening Aged Care program and by a fellowship received by Dr. Mudge from the Internal Medicine Society of Australia and New Zealand.
The authors report no financial arrangements with any for-profit companies in the previous 12 months and no other conflict of interest.
Author Contributions:Dr. Mudge was responsible for design, methods, and evaluation of the trial and assisted in securing funding. Ms. Giebel was responsible for the design and operation of the project and assisted in data collection and analysis and in securing funding. Dr. Cutler contributed to data collection and analysis. All authors contributed to drafting the manuscript.
Sponsor’s Role:The sponsors had no role in the design, analysis, or preparation of this manuscript.
REFERENCES
1. Sager MA, Franke T, Inouye SK et al. Functional outcomes of acute medical illness and hospitalization in older persons. Arch Intern Med 1996;156: 645–652.
2. Carlson JE, Zocchi KA, Bettencourt DM et al. Measuring frailty in the hos-pitalized elderly. Concept of functional homeostasis. Am J Phys Med Rehab 1998;77:252–257.
3. Lindenberger EC, Landefeld CS, Sands LP et al. Unsteadiness reported by older hospitalized patients predicts functional decline. J Am Geriatr Soc 2003; 51:621–626.
4. O’Keeffe S, Lavan J. The prognostic significance of delirium in older hospital patients. J Am Geriatr Soc 1997;45:174–178.
5. Inouye SK, Bogardus ST Jr, Charpentier PA et al. A multicomponent inter-vention to prevent delirium in hospitalized older patients. N Engl J Med 1999;340:669–676.
6. Creditor M. Hazards of hospitalization in the elderly. Ann Intern Med 1993;118:219–223.
7. Brown CJ, Friedkin RJ, Inouye SK. Prevalence and outcomes of low mobility in hospitalized older patients. J Am Geriatr Soc 2004;52:1263–1270. 8. McCusker J, Cole M, Abrahamowicz M et al. Environmental risk factors for
delirium in hospitalized older people. J Am Geriatr Soc 2001;49:1327–1334. 9. Johnson JH, Sager MA, Hirn G et al. Referral patterns to physical therapy in elderly hospitalized for acute medical illness. Phys Occup Ther Geriatr 1994;12:1–12.
10. Lazarus BA, Murphy JB, Coletta EM et al. The provision of physical activity to hospitalized elderly patients. Arch Intern Med 1991;151:2452–2456. 11. Siebens H, Aronow H, Edwards D et al. A randomized controlled trial of
exercise to improve outcomes of acute hospitalization in older adults. J Am Geriatr Soc 2000;48:1545–1552.
12. Jones CT, Lowe AJ, MacGregor L et al. A randomised controlled trial of an exercise intervention to reduce functional decline and health service utilisation in the hospitalised elderly. Australas J Ageing 2006;25:126–133.
13. de Morton N, Keating J, Jeffs K. Exercise for acutely hospitalised older med-ical patients. Cochrane Database Syst Rev 2007, (1): CD005955.
14. Mudge A, Laracy S, Richter K et al. Controlled trial of multidisciplinary care teams for acutely ill medical inpatients: Enhanced multidisciplinary care. In-tern Med J 2006;36:558–563.
15. Shah S, Vanclay F, Cooper B. Improving the sensitivity of the Barthel index for stroke rehabilitation. J Clin Epidemiol 1989;42:703–709.
16. Podsiadlo D, Richardson S. The timed ‘‘up and go’’ test: A test of basic func-tional mobility for frail elderly persons. J Am Geriatr Soc 1991;39:142–148. 17. Inouye SK, Leo-Summers L, Zhang D et al. A chart-based method for iden-tification of delirium: Validation compared with interviewer ratings using the confusion assessment method. J Am Geriatr Soc 2005;53:312–318. 18. Callen BL, Mahoney JE, Grieves CB et al. Frequency of hallway ambulation by
hospitalized older adults on medical units of an academic hospital. Geriatr Nurs 2004;25:212–217.
19. Hansen K, Mahoney JE, Palta M. Risk factors for lack of recovery of ADL independence after hospital discharge. J Am Geriatr Soc 1999;47:360–365. 20. Landefeld CS, Palmer RM, Kresevic D et al. A randomized trial of care in a
hospital medical unit especially designed to improve the functional outcomes of acutely ill older patients. N Engl J Med 1995;332:1338–1344.