Artigo Original
Camila Bolivar Martins Vieira1 Fernanda Dreux Miranda Fernandes2
Descritores
Transtorno autístico Fonoaudiologia Irmãos Qualidade de vida Apoio social
Keywords
Autistic disorder Speech, language and hearing sciences Siblings Quality of life Social support
Correspondence address: Fernanda Dreux Miranda Fernandes R. Cipotânea 51, Cidade Universitária, São Paulo (SP), Brazil, CEP: 0536-160. E-mail: [email protected] Received: 05/23/2012
Accepted: 12/19/2012
Study carried out at the Department of Physical Therapy, Speech-Language Pathology and Audiology and Occupational Therapy, School of Medicine, Universidade de São Paulo – USP – São Paulo (SP), Brazil. (1) Speech-Language Pathology and Audiology program, Department of Physical Therapy, Speech-Language Pathology and Audiology and Occupational Therapy, School of Medicine, Universidade de São Paulo – USP – São Paulo (SP), Brazil.
(2) Department of Physical Therapy, Speech-Language Pathology and Audiology and Occupational Therapy, School of Medicine, Universidade de São Paulo – USP – São Paulo (SP), Brazil.
Conlict of interests: nothing to declare.
autism spectrum
Qualidade de vida em irmãos de crianças incluídas no
espectro do autismo
ABSTRACT
Purpose: To assess the Quality of Life in siblings of children of the autism spectrum through self-response to the World Health Organization Quality of Life (WHOQOL)-BREF questionnaire. Methods: Social-demographic data of 77 children included in the autism spectrum, aged 3 to 16 years, were collected. From these information, 21 older siblings, aged 16 to 30 years, were selected to answer said questionnaire, proposed by the World Health Organization Mental Health Program for quality of life evaluation. Results: The data have shown a difference between the Environmental domain and the Physical and Psychological domains. Conclusion: The aspects related to the environment have an important role to the perception of quality of life self-declared by the subjects. However, family individuality, coping behaviors, social support, and assistance received directly interfere on this perception.
RESUMO
INTRODUCTION
Autism is a global developmental disorder that involves early and severe impairments in the areas of socialization, communication, and cognition(1).
According to the diagnostic criteria included in the Diagnostic and Statistical Manual of Mental Disorders(2) and
the Classiication of Mental and Behavioural Disorders(3),
symptoms must be observed before the age of three and should include severe and pervasive qualitative impairment in several areas of development, such as: reciprocal social interaction skills, communication skills and presence of stereotyped and restricted behavior, interests and activities.
Whatever the conceptual approach of the etiological hy-pothesis or of the diagnosis criteria involving infantile autism, language always represents a fundamental aspect(4). Thus, the
participation of speech and language therapy in the context of research and intervention becomes important, both for patients and their families.
The dificulty faced by families with a child included on the autism spectrum reveals a higher level of stress in the family system when compared to a control group of families with typically developing children(5).
Families living with an autistic child have a peculiar life situation. Family dynamics suffers mobilizations, ranging from inancial strains to aspects related to physical, psychological and social quality of life (QoL) of caregivers(6).
A study with 40 autistic children reported that these chil-dren, in their perception of the world, are happy, regardless of their functional deicits, as they reported QoL indexes that were similar to those of normal children(7).
However, it is noticed in the literature that those who frequently suffer the consequences of the autism framework are their family members (5,8-12). Parents or caregivers of
children included in the autism spectrum may face tensions and therefore could beneit from a family-centered treatment proposals(10).
The QoL can be deined as the individual’s perception of his position in life, in the context of culture and value systems in which he lives, and in relation to his goals, expectations, standards and concerns(13).
The recognition of the multidimensional nature of QoL is relected on the WHOQOL-100, an instrument created in 1995 by the World Health Organization (WHO), by means of an international multicenter collaborative project(14).
In 1998, the WHO QoL group, realizing the need for short instruments with good psychometric characteristics created the ab-breviated version of the WHOQOL-100, the WHOQOL-BREF (15).
The WHOQOL-BREF (16) consists of 26 issues: two general
ones related to QoL and the others representing each of the 24 facets that comprise the original instrument(15).
The literature that relates QoL, social support and psychological and social adjustments involving siblings of children included in the autism spectrum is still scarce and contradictory. Few studies address this issue, which can provide important data about the family and the adaptive
context to which the autistic individual is exposed to for long life periods. A total of 22 siblings of children with autism were reported by their mothers as having more behavior problems and less social behaviors(17). Stressful
living conditions were verified in 14 siblings of autistic individuals, suggesting that family counseling would be recommended in these cases, to help them cope with their feelings and problems(18).
A study that assessed sibling relationships when one of the children has autism has provided new and important un-derstandings of these relationships, revealing similarities and differences in the quality of relationships between typically developing sibling dyads and autistic sibling dyads(19). That
study suggested that, despite having a sibling with autism being frequently related to family dificulties, family characteristics may inluence the relationship depending on coping character-istics and available parental support(19).
Thus, parents have an important role in sibling relation-ships, not only in adolescence but also in adulthood(19). It
was veriied in the literature that the number of studies involving families of autistic children do not correspond to what would be expected when considering the impact of the autistic child in the family dynamics and the importance of family involvement for diagnosis, intervention and educa-tion processes(1).
Thus, the purpose of this study was to assess the self-reported QoL of older siblings of autistic children using the WHOQOL-BREF(16).
METHODS
This research was submitted to the Ethics Committee in Research of the School of Medicine, Universidade de São Paulo (USP) and was approved under protocol 312/1. The subjects or their guardians signed an informed consent form (ICF).
Social-demographic data of 77 patients included in the au-tism spectrum were collected. Patients were between 3 and 16 years of age (mean=7.4 years), being 62 males and 15 females. The 52 brothers were aged between two months and 30 years (mean=13 years), being 28 males and 34 females.
Inclusion criteria for the application WHOQOL were that the siblings should be older than the individuals with autism and should be living in the same residence. Being older than the autistic child was defined as a criterion considering that the autism spectrum diagnosis has differ-ent impacts on older and younger siblings. Furthermore, among older siblings, all had proper age to answer the questionnaire. Living in the same residence was considered as inclusion criterion because this is the situation in which the presence of the autistic child may have more interfer-ence on the QoL of siblings. If the autistic individual had more than one sibling within the inclusion criteria, all would receive the questionnaire. Educational level and socioeconomic status were not considered.
females and six males - who were living with their autistic siblings at the time of the study. Individuals on the autism spectrum were 17 children and adolescents with diagnoses assigned by neurologists and/or psychiatrists according to the criteria of the DSM-IV(2) or ICD-10(3). These individuals
were aged between 6 and 16 years (mean=10.4) being three female and 14 male, who were attending weekly individual speech-language therapy.
Table 1 shows the distribution of subjects and their siblings regarding age.
To avoid the bias that could be caused by the application of the questionnaire by a professional associated with the care of the autistic sibling, the questionnaire (along with the ICF) was delivered to the family or caregiver who brought the patient to speech-language therapy. The content of the research was explained and their collaboration to deliver the questionnaire to the recipient (older sibling of the patient) and then return it on the next therapeutic sessions was asked. The researchers were available to answer any questions by phone or in person, although there was no contact.
The siblings answered the WHOQOL-BREF questionnaire, which consists of 26 questions divided into four domains (physical, psychological, personal relationships and environ-mental) (Appendix 1).
The data collected were statistically analyzed and quanti-tatively and qualiquanti-tatively described.
An estimated equivalence due to the difference in the number of questions per domain was carried out. Student t test and Pearson correlation were applied in order to deter-mine which pairs of variables presented signiicant values and correlations.
RESULTS
Seventy-seven autistic individuals, of whom 52 had siblings (68%) and 25 were only child (32%), were investigated. Of those who had siblings, 36 had older siblings (77%), 13 younger siblings (19%) and three both younger and older siblings (4%).
Of all the patients investigated, 21 had older siblings who it the inclusion criteria of the study (totaling 28 potential subjects to whom questionnaires were delivered). However, the siblings of only 17 patients participated in the study, totaling 21 subjects who completed the WHOQOL-BREF questionnaire.
The satisfaction index — identiied by the mean percent-age scores of each domain — revealed that the most affected domain was the environment.
Figure 1 shows the maximum and mean scores obtained by the subjects for each domain.
The comparison between the different domains identiied differences between the Environment and the Psychological and Physical domains. The Pearson correlation showed a ten-dency toward linear correlation between Psychological and Physical domains and between Environment and Personal Relationships domains (Chart 1).
DISCUSSION
The present study had as initial hypothesis a decrease in self-reported QoL of siblings and caregivers of children included in the autism spectrum(8-12). Demographic data were
collected in order to obtain an overview of the families and select the participants of this study. It was found that, of the 77 patients studied, 32% were only child. This percentage is similar to that observed in a study conducted by the Brazilian Institute of Geography and Statistics (IBGE)(20) in 2007,
showing that these families do not have fewer children than the general population.
Figure 1. Mean scores obtained according to domains 60 50 40 30 20 10 0 15 11.62 33.62 Physical Psychological
Maximum Obtained mean Personal relations Environment 45 15 10.71 55 37.62
On the other hand, it is believed that the predominance of older siblings may be related to the vicissitudes of creating an autistic child, which makes most parents cease to have other children, given the demand for care and attention posed by the autistic child (5,6,11,12,21,22).
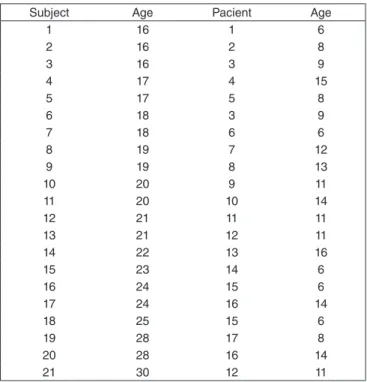
Chart 1. Distribution of subjects who responded to the WHOQOL-BREF questionnaire according to age and siblings (patients)
Subject Age Pacient Age
1 16 1 6
2 16 2 8
3 16 3 9
4 17 4 15
5 17 5 8
6 18 3 9
7 18 6 6
8 19 7 12
9 19 8 13
10 20 9 11
11 20 10 14
12 21 11 11
13 21 12 11
14 22 13 16
15 23 14 6
16 24 15 6
17 24 16 14
18 25 15 6
19 28 17 8
20 28 16 14
In Appendix 2 it is possible to visualize the outline(23) of the
24 questions of the WHOQOL-BREF(16).
In another study, the same questionnaire was used and QoL was assessed in a group of parents of children with pervasive developmental disorders, cerebral palsy or mental retardation. The results showed impairment of the Physical and Social Relations domains, besides worse overall perception of QoL and health(21).
A thesis drawn from the study of 31 siblings of autistic children compared to a control group of children with spe-ciic disorders of speech articulation using the questionnaire of quality of life assessment in children and adolescents (AUQUEI), aimed to verify whether the three aspects in-volved in this disorder (communication, socialization and stereotyped behavior) would also be compromised in sib-lings aged 7 to 11 years and whether this inluenced their QoL. The results showed impairment in QoL of siblings of autistic children, making clear the need for more attention and assistance to this population as well as further studies about this issue(8).
In the present study the domain with the lowest rate of satisfaction and the only one that presented difference was Environment in relation to the Physical and Psychological domains, showing the interference of this area in the QoL of the subjects in question.
This corroborates the study of 150 caregivers of children within the autism spectrum, in which, with the same question-naire, the only domain that was related to the others was also the Environment(12).
In the present study, another inding was the tendency to linear correlation between Psychological and Physical domains and between Environment and Personal Relationships domains. This result indicates a relationship: an increase in the score in one of these areas is directly proportional to the increase in the score of another area.
This way, one can see that both caregivers of autistic children and their siblings realize dificulties in their QoL, particularly in relation to access to health services and transpor-tation, living conditions, security, leisure, inancial resources, opportunities to acquire information and skills.
This inding conirms the international literature, which reports dificulties in accessing specialized medical care and other health areas, besides the lack of information on access to leisure and education for this speciic public, which ulti-mately intensiies stress and negatively inluence the QoL reported by these families(24). However, it is observed that the
self-reported QoL for these siblings was not as impaired as described in the literature(8,12,25).
It is noteworthy that in the current study there was no ap-plicator bias since the responses were obtained without any contact between the researcher and the subjects, which brings a high reliability to the responses provided.
It is believed that the fact that all patients are assisted by specialized health services, for example, speech-language therapy, contribute to the good QoL reported by the siblings.
It should benoted that some limitations were observed in this study, such as the limited number of subjects and the lack of a control group.
Future studies with a larger number of subjects and the in-clusion of a comparison of QoL of siblings of autistic children with a control group of siblings of children with other types of dificulties would bring results and conclusions that could contribute to the discussion and formulation of intervention strategies and adequate social support to these families.
CONCLUSIONS
The initial hypothesis of the study was that the QoL of these siblings would somehow be impaired as veriied on the national and international literature with caregivers and siblings of autistic children. However, the results of this study indicate that the siblings who responded to the questionnaire did not report a signiicantly impaired QoL.
It is concluded that family individuality, coping strategies, social support and received assistance directly inluence the perception of QoL of these subjects.
*CV performed it; FDMF was the counselor.
REFERENCES
1. Fernandes FDM. Famílias com crianças autistas na literatura internacional. Rev Soc Bras Fonoaudiol. 2009;14(3):427-32.
2. American Psychiatric Asssociation. Manual diagnóstico e estatístico de transtornos mentais. DSM- IV. Porto Alegre: Artes Médicas; 1995. 3. Organização Mundial de Saúde. Classiicação de transtornos mentais e
de comportamento do CID – 10. Porto Alegre: Artes Médicas; 1993. 4. Fernandes FDM. A questão da linguagem em autismo infantil: Uma
revisão crítica da literatura. Rev Neuropsiq Inf Adolesc. 1994;2(3):5-10. 5. Sivberg B. Family system and coping behaviours: a comparison between parents of children with autistic spectrum disorders and parents with non-autistic children. Autism. 2002;6(4):397-409.
6. Fávero MAB, Santos MA. Autismo infantil e estresse familiar: Uma revisão sistemática da literatura. Psicol Relex Crit. 2005;18(3):358-69. 7. Elias AV, Assumpção Jr FB. Qualidade de vida e autismo. Arq
Neuro-Psiquiatr. 2006;64(2-A):295-9.
8. Marciano ARF. Qualidade de Vida em irmãos de autistas [tese]. São Paulo: Faculdade de Medicina da Universidade de São Paulo; 2004. 216 p. Table 1. Comparison between WHOQOL-brief domains
P versus Ph P versus E P versus PR Ph versus E Ph versus PR E versus PR
p-value 0.19 0.04* 0.45 0.01* 0.19 0.28
Pearson correlation 0.70* 0.50 0.55 0.36 0.33 0.83*
9. Allik H, Larsson JO, Smedje H. Health-related quality of life in parents of school-age children with Asperger syndrome or high-functioning autism. Health Qual Life Outcomes. 2006;4(1):1-8.
10. Schieve LA, Blumberg SJ, Rice C, Visser SN, Boyle C. The relationship between autism and parenting stress. Pediatrics. 2007;119(Suppl 1): 114-21.
11. Schmidt C, Dell’aglio DD, Bosa CA. Estratégias de coping de mães de portadores de autismo: Lidando com diiculdades e com a emoção. Psicol Relex Crit. 2007;20(1):124-31.
12. Barbosa MRP. Suporte social e qualidade de vida em famílias de crianças do espectro autístico [tese]. São Paulo: Faculdade de Medicina da Universidade de São Paulo; 2010. 183 p.
13. The WHOQOL Group. Development of the WHOQOL: Rationale and current status. Monograph on Quality of Life Assessment: cross-cultural issues. Int J Mental Health. 1994;23(3):24-56.
14. The WHOQOL Group. The World Health Organization quality of life assessment (WHOQOL): position paper from the World Health Organization. Soc Sci Med. 1995;(10):1403-9.
15. World Health Organization. The WHOQOL Group. Developmental of the World Health Organization Basic Documents. Genebra: WHO; 1998.
16. Organização Mundial de Saúde. Divisão de saúde mental. Grupo WHOQOL [Internet]. Versão em português dos instrumentos de avaliação de qualidade de vida. 1998. [cited 2012 Nov 28]. Available from: http:// www.ufrgs.br/psiq/whoqol-100.
17. Hastings RP. Brief report: Behavioral adjustment of siblings of children with autism. J Autism Dev Disord. 2003;33(1):99-104.
18. Benderix Y, Sivberg B. Siblings experiences of having a brother or sister with autism and mental retardation: a case study of 14 siblings from ive families. J Pediatr Nurs. 2007;22(5):410-8.
19. Mailick M, Orsmond GI. Siblings of individuals with autism spectrum disorders across the life course. Ment Retard Dev Disabil Res Rev. 2007;13(1):59-80. 20. Brasil. Instituto Brasileiro de Geografia e Estatística. Síntese dos
Indicadores Sociais 2007 – Uma Análise das Condições de Vida da População Brasileira. Brasília: Instituto Brasileiro de Geografia e Estatística. 2007.
21. Mugno D, Ruta L, D’arrigo VG, Mazzone L. Impairment of quality of life in parents of children and adolescents with pervasive developmental disorder. Health Qual Life Outcomes. 2007;(5):22-9.
22. Ghanizadeh A, Alishahi MJ, Ashkani H. Helping families for caring children with autistic spectrum disorders. Arch Iran Med. 2009;12(5):478-82.
23. Fleck MPA. O instrumento de avaliação de qualidade de vida da Organização Mundial da Saúde (WHOQOL-100): Características e perspectivas. Cienc Saúde Col. 2000;5(1):33-8.
24. Kraus MW, Gulley S, Sciegaj M, Wells N. Access to specialty medical care for children with mental retardation, autism, and other special health care needs. Mental Retard. 2004;41(5):329-39.
Appendix 1. WHOQOL-brief questionnaire (quality of life)
Por favor, leia cada questão, veja o que você acha e circule no número e lhe parece a melhor resposta.
muito ruim ruim nem ruim nem
boa boa muito boa
1 Como você avaliaria sua qualidade de vida? 1 2 3 4 5
muito insatisfeito satisfeito nem satisfeito
nem insatisfeito satisfeito
muito satisfeito
2 Quão satisfeito (a) você está com a sua
saúde? 1 2 3 4 5
As questões seguintes são sobre o quanto você tem sentido algumas coisas nas últimas duas semanas.
nada muito pouco mais ou
menos bastante extremamente
3 Em que medida você acha que sua dor (física)
impede você de fazer o que você precisa? 1 2 3 4 5
4 O quanto você precisa de algum tratamento médico
para levar sua vida diária? 1 2 3 4 5
5 O quanto você aproveita a vida? 1 2 3 4 5
6 Em que medida você acha que a sua vida tem
sentido? 1 2 3 4 5
7 O quanto você consegue se concentrar? 1 2 3 4 5
8 Quão seguro(a) você se sente em sua vida diária? 1 2 3 4 5
9 Quão saudável é o seu ambiente físico (clima,
barulho, poluição, atrativos)? 1 2 3 4 5
As questões seguintes perguntam sobre quão completamente você tem sentido ou é capaz de fazer certas coisas nestas últimas duas semanas.
10 Você tem energia suficiente para seu dia-a-dia? nada muito pouco médio muito completamente
11 Você é capaz de aceitar sua aparência física? 1 2 3 4 5
12 Você tem dinheiro suficiente para satisfazer
suas necessidades? 1 2 3 4 5
13 Quão disponíveis para você estão as
informações que precisa no seu dia-a-dia? 1 2 3 4 5
14 Em que medida você tem oportunidades de
atividade de lazer? 1 2 3 4 5
Name of sibling:__________________________________________________________________________________________ Age:___________
Name of patient:_________________________________________________________________________________________Age:___________
As questões seguintes perguntam sobre quão bem ou satisfeito você se sentiu a respeito de vários aspectos de sua vida nas últimas duas semanas.
muito
insatisfeito satisfeito
nem satisfeito nem insatisfeito
satisfeito muito satisfeito
15 Quão bem você é capaz de se locomover? 1 2 3 4 5
16 Quão satisfeito(a) você está com o seu
sono? 1 2 3 4 5
17
Quão satisfeito(a) você está com sua capacidade de desempenhar as atividades
do seu dia-a-dia?
1 2 3 4 5
18 Quão satisfeito(a) você está com sua
capacidade para o trabalho? 1 2 3 4 5
19 Quão satisfeito(a) você está consigo mesmo? 1 2 3 4 5
20
Quão satisfeito(a) você está com suas relações pessoais (amigos, parentes,
conhecidos, colegas)?
1 2 3 4 5
21 Quão satisfeito(a) você está com sua
vida sexual? 1 2 3 4 5
22 Quão satisfeito(a) você está com o apoio
que você recebe de seus amigos? 1 2 3 4 5
23 Quão satisfeito(a) você está com as
condições do local onde mora? 1 2 3 4 5
24 Quão satisfeito(a) você está com o seu
acesso aos serviços de saúde? 1 2 3 4 5
25 Quão satisfeito(a) você está com o seu meio
de transporte? 1 2 3 4 5
As questões seguintes referem-se a com que freqüência você sentiu ou experimentou certas coisas nas últimas duas semanas.
Nunca Algumas vezes frequentemente Muito frequentemente sempre
26
Com que freqüência você tem sentimentos negativos tais como mau humor, desespero, ansiedade, depressão?
1 2 3 4 5
Alguém lhe ajudou a preencher este questionário?... Quanto tempo você levou para preencher este questionário?... Você tem algum comentário sobre o questionário?...
OBRIGADO PELA SUA COLABORAÇÃO
Appendix 2. WHOQOL domains and frameworks (23)
Domínio I- domínio físico
1. dor e desconforto 2. energia e fadiga 3. sono e repouso
Domínio II- domínio psicológico
4. sentimentos positivos
5. pensar, aprender, memória e concentração 6. autoestima
7. imagem corporal e aparência 8. sentimentos negativos
Domínio III- nível de independência
9. mobilidade
10. atividades da vida cotidiana
11. dependência de medicação ou de tratamentos 12. capacidade de trabalho
Domínio IV- relações sociais
13. relações pessoais 14. suporte (apoio) social 15. atividade sexual
Domínio V- meio ambiente
16. segurança física e proteção 17. ambiente no lar
18. recursos financeiros
19. cuidados de saúde e sociais: disponibilidade e qualidade 20. oportunidades de adquirir novas informações e habilidades 21. participação em, e oportunidades de recreação/ lazer 22. ambiente físico: poluição/ ruído/ trânsito/ clima 23. transporte
Domínio VI- aspectos espirituais/ religião/ crenças pessoais