Rev. Col. Bras. Cir. vol.38 número5 en a02v38n5
Texto
Imagem
Documentos relacionados
A prospective study of dentoalveolar trauma epidemi- ology was carried out among emergency room patients treated by the internship students of the Oral and Maxillo- facial Trauma
An example based on a real cascaded hydro system is used to prove as a new contribution to earlier studies that the physical data defining the hydro chain parameters used in
Na PUCRS, como convidado do Seminário In- ternacional Inovação, Universidade e Prestação de Serviços, promovido pela Pró-Reitoria de Pesquisa e Pós-Graduação, compartilhou suas
Following this analysis, Kent & Karner (2018) used the LTS approach on a recent study to prioritize bicycle projects based on accessibility performance measures (PM). The
A metodologia utilizada no desenvolvimento do projeto baseou-se nas etapas propostas por Hanington e Martin (2012), sendo elas: (i) Planejamento, Escopo e Definição: etapa
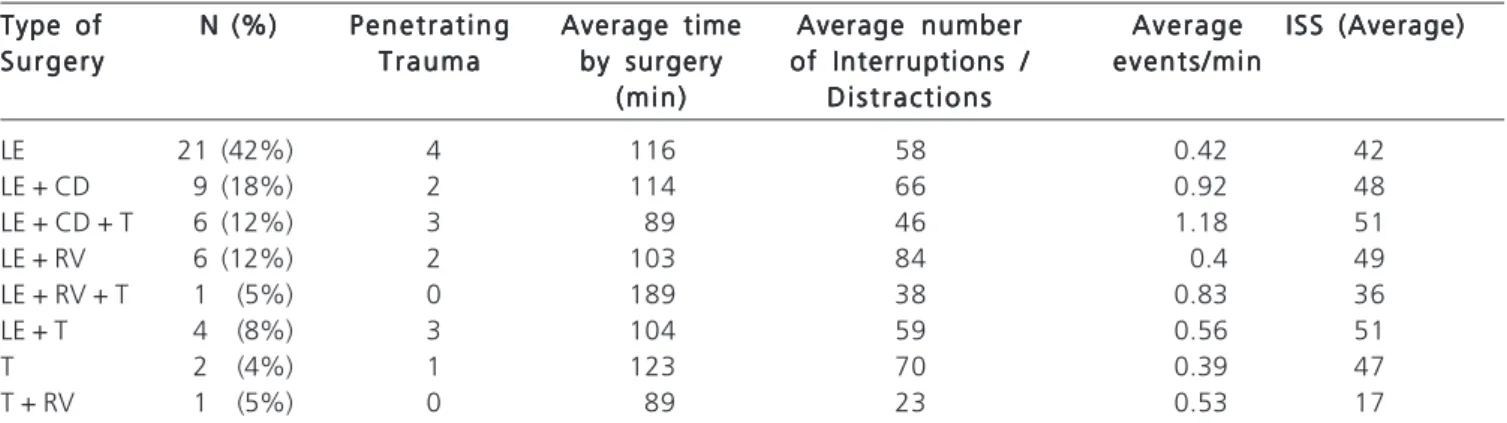
Identificação de distração e interrupção das atividades dos profissionais durante o intraoperatório; 2) Fatores contribuintes das distrações e das interrupções e
Data analysis revealed three thematic categories: 1) The identification of distractions and interruptions of the professionals' activities during the intraoperative period; 2)
Assim, as melhores opções de mapeamento estratégico se dão através da visão baseada em recursos, que irá explanar sua vantagem competitiva, junto ao modelo VRIO que faz
