www.rpped.com.br
REVISTA
PAULISTA
DE
PEDIATRIA
ORIGINAL
ARTICLE
Functional
performance
of
school
children
diagnosed
with
developmental
delay
up
to
two
years
of
age
Lílian
de
Fátima
Dornelas
a,∗,
Lívia
de
Castro
Magalhães
baPrefeituraMunicipaldeUberlândia,Uberlândia,MG,Brazil
bDepartamentodeTerapiaOcupacional,EscoladeEducac¸ãoFísica,Fisioterapia,Educac¸ãoFísica(EFFTO),UniversidadeFederal
deMinasGerais(UFMG),BeloHorizonte,MG,Brazil
Received7January2015;accepted26May2015 Availableonline20October2015
KEYWORDS
Evaluation;
Childdevelopment;
Students
Abstract
Objective: Tocomparethefunctionalperformanceofstudentsdiagnosedwithdevelopmental delay(DD)uptotwoyearsofagewithpeersexhibitingtypicaldevelopment.
Methods: Cross-sectionalstudywithfunctionalperformanceassessmentofchildrendiagnosed withDDuptotwoyearsofagecomparedtothosewithtypicaldevelopmentatseventoeight yearsofage.Eachgroupconsistedof45children,selectedbynon-randomsampling,evaluated formotorskills,qualityofhomeenvironment,schoolparticipationandperformance.ANOVA andtheBinomialtestfortwoproportionswereusedtoassessdifferencesbetweengroups.
Results: ThegroupwithDDhadlowermotorskillswhencomparedtothetypicalgroup.While 66.7%ofchildreninthetypicalgroupshowedadequateschoolparticipation,receivingaidin cognitiveandbehavioraltaskssimilartothatofferedtootherchildrenatthesamelevel,only 22.2%ofchildrenwithDDshowedthesameperformance.Although53.3%ofthechildrenwith DDachievedanacademicperformanceexpectedfortheschoollevel,therewerelimitationsin someactivities.Onlytwoindicatorsoffamilyenvironment,diversityandactivitieswithparents athome,showedstatisticallysignificantdifferencebetweenthegroups,withadvantagebeing shownforthetypicalgroup.
Conclusions: ChildrenwithDDhavepersistentdifficulties atschoolage,withmotordeficit, restrictionsinschoolactivityperformanceandlowparticipationintheschoolcontext,aswellas significantlylowerfunctionalperformancewhencomparedtochildrenwithoutDD.Asystematic monitoringofthispopulationisrecommendedtoidentifyneedsandminimizefutureproblems. ©2015SociedadedePediatriadeSãoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(https://creativecommons.org/licenses/by/4.0/).
∗Correspondingauthor.
E-mail:liliandefatima@hotmail.com(L.F.Dornelas).
http://dx.doi.org/10.1016/j.rppede.2015.10.001
2359-3482/©2015SociedadedePediatriadeSãoPaulo.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY
PALAVRAS-CHAVE
Avaliac¸ão; Desenvolvimento infantil;
Escolares
Desempenhofuncionaldeescolaresquereceberamdiagnósticodeatraso
dodesenvolvimentoneuropsicomotoratéosdoisanos
Resumo
Objetivo: Compararodesempenhofuncionaldeescolaresquereceberamdiagnósticodeatraso dodesenvolvimentoneuropsicomotor(ADNPM)atédoisanoscomparescomdesenvolvimento típico.
Métodos: Estudotransversal comavaliac¸ãododesempenhofuncionalemcrianc¸as que rece-beram diagnóstico de ADNPM até os dois anos e em crianc¸as com desenvolvimento típico nasidadesdeseteeoitoanos.Cadagrupofoiconstituídopor45crianc¸as,selecionadaspor amostragemnão aleatória,avaliadas quantoàcoordenac¸ãomotora,qualidade doambiente familiar,participac¸ãoedesempenhonaescola.OstestesAnovaebinomialparaduasproporc¸ões foramusadosparaverificardiferenc¸aentreosgrupos.
Resultados: OgrupocomADNPMobtevedesempenhomotorinferiorquandocomparadocom ogrupo típico.Enquanto 66,7%dascrianc¸as dogrupotípico tiveramparticipac¸ãoadequada naescola, receberamauxílionastarefas cognitivasecomportamentaissimilar aooferecido àsdemaiscrianc¸asdomesmonível,apenas22,2%crianc¸ascomatrasoapresentaramomesmo desempenho.Embora53,3%dascrianc¸ascomatrasotenhamatingidodesempenhoacadêmico esperadoparaonívelescolar,houvelimitac¸õesemalgumasatividades.Apenasdoisindicadores doambientefamiliar,diversidadeeatividadecomospaisemcasamostraramdiferenc¸a esta-tisticamentesignificativaentreosgrupos,comvantagemparaogrupotípico.
Conclusões: Crianc¸ascomADNPMapresentamdificuldadespersistentesnaidadeescolar,com déficitmotor,restric¸õesnodesempenhodeatividadesescolaresebaixaparticipac¸ãono con-texto escolar,alémdedesempenhofuncionalsignificativamenteinferioraodecrianc¸as sem históriadeatraso.Recomenda-seoacompanhamentosistemáticodessapopulac¸ãopara identi-ficarnecessidadeseminimizarproblemasfuturos.
©2015SociedadedePediatriadeSãoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Developmentaldelay(DD)isaconditioninwhichthechildis
notdevelopingand/ordoesnotachieveskillsconsistentwith
whatisexpectedfortheirage.1Althoughtheterm‘‘delay’’
gives the impression of a relatively benigncondition that improveswithage,many ofthosechildrendonotreceive follow-upwithsystematic assessmentsand haveproblems at schoolage andadult life.2 Infact,it is estimated that
60---70%ofchildrenbornwithriskconditionswillrequire sup-portfromspecialeducationservicesinelementaryandhigh school,andthereisevidencethatgapsinthedevelopment of childrenabout toenterschool mayimpairtheir school performanceandfutureopportunities.3
Studies4,5 on the development outcome at school age
indicate that DD has an effect on a complex range of symptoms, without a defined disease profile, and thus it isimportanttoobtaininformationaboutwhatthechildis capableofdoinginadailycontext,tobetterunderstandits consequences.Althoughitisrecommendedthattheuseof theterm‘‘DD’’berestrictedtothefirstfiveyearsoflife,6
inBrazilitsuseiscommonthroughoutchildhoodand adoles-cence,withoutabetterunderstandingofthedevelopment outcomeofthesechildren,especiallyregardingfunctional performance in the school context. We should therefore investigatetheoutcomeofthesechildreninterms offinal diagnosis,aswell asthe impactof thedelayonthe func-tionalandacademicperformance.
AsexplainedbytheInternationalClassificationof Func-tioning, Disability and Health---ICF---WHO (World Health Organization),7inordertounderstandtheimpactofahealth
conditionsuchasDDonthechild’slife,itisimportantto per-formanextensiveassessmenttoobtaininformationnotonly aboutbasicbodyfunctions,butalsoontheactivityand par-ticipationindifferentcontexts.Inthisstudy,theICF---WHO modelwasusedtoguidetheprocessofassessingchildren withahistory ofDD anddescribethechild’sperformance intheschoolcontext.Theaimofthestudywastocompare thefunctionalperformanceofstudentswhowerediagnosed withDD upto two yearsof age, withthat of peers with typicaldevelopment.
Method
Thiswasacross-sectionalstudytoevaluatethefunctional
performanceof students whowere diagnosed withDD up
totwoyearsofageandthosewithtypicaldevelopmentat
seventoeightyearsofage,selectedbynon-random
samp-lingandmatchedforage,genderandfamilyincome.Each
group consisted of 45 children and the subjects with DD
were recruited from Associac¸ão de Assistência à Crianc¸a
Deficiente de Minas Gerais (AACD/MG); their peers were
selectedfromthesameschoolswherethechildrenfromthe
AACD/MGisspecializedintreatingindividualswith phys-icaldisabilities.Babieswhohavepre-,peri-,andpostnatal
complicationsand/ordevelopmentalproblemsarereferred
byphysiciansfrombasichealthunitsorhospitalsandbythe
parents,beingevaluatedbytheAACD/MGteam,who
ver-ifytheneedforintervention.ThediagnosisofDDisbased
onaclinicalassessmentcarriedoutbythephysicianofthe
institution, throughneurological assessment. As the term
‘‘DD’’ is not found in the ICD-10, in order tobe treated
at the institution, these children are classified according
tothe categoriesof ChapterVI(NervousSystemDiseases)
--- code:G00-G99,specificallyin thesubcategory closerto
theterm,UnspecifiedCerebralPalsy---code:G80.9.After
medicalassessment,childrenarereferredtooverall
assess-ment,inwhich themultidisciplinaryteam,consisting ofa
physiotherapist, speech therapist, psychologist and
occu-pational therapist, makes the direct clinical observation,
describesthechild’sdevelopment,discussesthecasewith
thephysiciananddefineswhetherthechildwillbenefitfrom
interventionandwhattherapiesarenecessary.Allchildren
admittedtotheAACDundergoaninitialmedicalevaluation,
aswellasafinalevaluation,whentheymeetthecriteriafor
discharge.Assessmentsarepredominantlyclinical,without
theuseofstandardizedtests.ChildrenwithDDadmittedat
AACDusuallyexhibitmotordelayandhaveweekly
consulta-tionswithphysicaltherapy,hydrotherapyandoccupational
therapyprofessionalstoacquiretypicalgait,whentheyare
dischargedfromcare.EventhoughtheAACD/MGdoesnot
providealongitudinalfollow-upprogramforthesechildren,
astheyhave nophysicaldisability,theymayreturntothe
institutiontoreceiverecommendationsortoundergo
ther-apieswithspecificgoals,albeitintheshortterm.Thereis
nospecific follow-upprogramfor thispopulation,andthe
returnvisitsdependontheparents’decision.
Inthiscontext,eligiblechildrenforthestudywere
iden-tifiedthrough the review of medical files withthe G80.9
codefromICD-10,fromAugust2001toAugust2009,inthe
AACD/MGfilingsector.Theinitiallistcontained329records
thatwerescreened,accordingtotheinclusionandexclusion
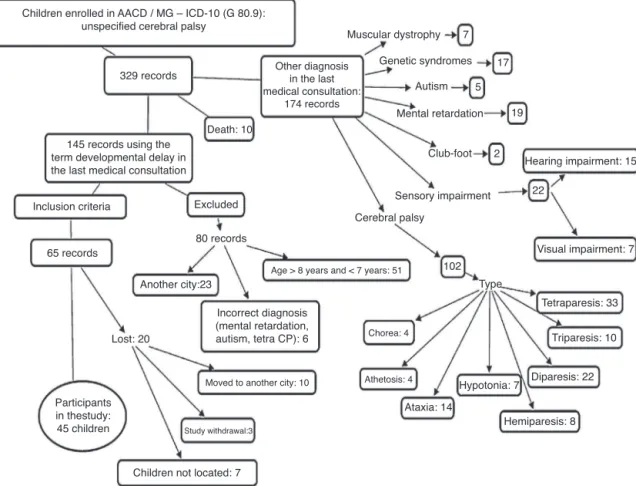
criteria,until45studyparticipantswereobtained,asshown inFig.1.Theinclusioncriteriawerechildrenofboth gen-ders,bornbetweenJanuary2003andApril2006,livinginthe cityofUberlândia(MG),diagnosedwithDD,whichhadpre-, peri-,andpostnatalcomplications,withnoevident neuro-logicaland/ororthopedicdisorders,malformations,aswell asvisual or hearingimpairments. The studyonly included children who had,in the last medicalevaluation, typical gait,theoneswhoweredischargedfromtherapeuticcare, attendedschoolregularlyandwhose parents or guardians signed theinformed consentform(ICF), authorizingtheir participationin thestudy.Childrenwereexcludediftheir diagnosis changed to cerebral palsy, muscular dystrophy, autism,mentalretardationorsyndromes, aswellasthose whoremainedwithadiagnosisofDD,buthadevident neu-rologicaland/or orthopedicdisorders,malformations,and visualorhearingimpairment.
The children with typical developmentwere recruited fromthesameschoolsthecasesfromAACD/MGattended. Therecruitment ofeach child fromthetypicalgroup was carriedoutinthesameclassroom ofeachchilddiagnosed withDD.The authors, afterreceiving parentalconsentof the child with DD, went to the school and made contact
with the teacher. Each teacher was asked to identify, in therollcall,studentsofthesamegenderandageasthose diagnosedwithDD.Afterthechildrenwereidentified,they werechosenbydrawinglots,andaninvitationletter(ICF) was sent tothe parent/guardian. Along with the ICF, the parent/guardianansweredabriefquestionnaireabout the development history in order to ensure that the child fit thegroupprofile.Onlychildren whoseICFswerereturned withtheparents’/guardian’ssignatureandwiththe ques-tionnaireanswered by parents/guardians wereevaluated; otherwise, the teacher choseanother studentby drawing lots.Childrenwereexcludediftheyhad,accordingtothe questionnaire,adiagnosisofspecificneurologicalorgenetic disordersand risk factorssuch asprematurity and/or low birth weight, hearing and visual impairments, as well as orthopedicproblems (fractureofthelowerlimbsand oth-ers),continuoususeofanticonvulsants,prolongedillnessin thethreemonthsprior tothetest, historyofgrade repe-titionanddifficultiesthatrequiredpedagogicalsupportor somekindofspecializedtherapy(physicaltherapy,speech therapy,psychologicalsupport,occupationaltherapy).
Thefollowingtoolswereusedintheresearch:
• Semi-structuredsystemfordataextractionfromrecords of DD children from the AACD/MG. Information was obtainedaboutthechild’shistory(gestationalage,birth weight and neonatal conditions), medical diagnosis on enteringtheinstitutionandtheoneregisteredinthelast consultation in the unit, parents/guardian information (maternalandpaternalschooling,familyincome),school data(name,address,telephone,teacherandgrade),as wellasrehabilitationaspects(child’sinitialandfinal eval-uationsmadebytherehabilitationteamandthetherapies performedduringtheinterventionperiod).Astheinitial andfinalevaluationsofeachchildismadedescriptively, theinformationwascategorizedintothreecomponents: (a)motor,fortheevaluationofthephysicaltherapy sec-tor;(B)activity,fortheoccupationaltherapysector,and (c)participation,for thepsychology sector assessment; theinformationofeachcomponentwascodedtoindicate whether the child’s developmental level was delayed, suspected or appropriate. Data collection from medi-calrecordswasperformedbytworesearchers,whohad beenpreviouslytrainedwith20records,obtainingagood Kappaagreementindex(0.63---0.79).
Children enrolled in AACD / MG – ICD-10 (G 80.9): unspecified cerebral palsy
329 records
Death: 10
Muscular dystrophy
Genetic syndromes
Autism
Mental retardation Other diagnosis
in the last medical consultation:
174 records
Incorrect diagnosis (mental retardation, autism, tetra CP): 6
Club-foot
Sensory impairment
Hearing impairment: 15
Visual impairment: 7
Tetraparesis: 33
Triparesis: 10
Diparesis: 22
Hemiparesis: 8 Hypotonia: 7
Ataxia: 14 Athetosis: 4
Chorea: 4 Cerebral palsy
7
17
5
2
22
102
19
Excluded Inclusion criteria
65 records
Another city:23
Lost: 20
Study withdrawal:3 Participants
in thestudy: 45 children
145 records using the term developmental delay in the last medical consultation
Moved to another city: 10
Age > 8 years and < 7 years: 51
Children not located: 7 80 records
Type
Figure1 Screeningofpatients’recordstoselecttheparticipantsintheDDgroup.
masteryoftheskillsexpectedfortheschoolyear---
pre-sentedpre-syllabicleveland/orgrading.
• MovementAssessmentBatteryforChildren---MABC-28:
It is a standardized test toidentify motor coordination disorders in children aged4---16 years old, divided into three areas: manualdexterity, hand grasping, throwing andbalance.Thesumofscoresforeachcategoryprovides astandardizedscore,andthesumofthethreecategories providesthetotalscore,whichisconvertedtopercentile. Acut-off≤15%indicatespossiblemotorimpairment,and ascore≤5%indicatesdefinitivemotordeficits.Children withscore≤5%wereconsideredashavingmotor coordi-nation problemsorsignsofDevelopmentalCoordination Disorder (DCD); ascoreof 6---15%,suspectedcases, and children with a score >15% were considered as having normalmotorperformance.
• School Function Assessment --- SFA9: This is a
ques-tionnaire to assess functional performance and the participation of children aged5---12 years in the school environment, consisting of three parts: participationin differentschoolenvironments,assistancewithtasksand taskperformance.TherawSFAscoresareconvertedinto ascaleof0---100,withthelatterbeingthehighestpoint or a fully operational degree in the assessed area. SFA resultscanbeinterpretedintwoways,atthebasicand advancedlevels.Forthisstudy,weusedthebasiclevel, whichshowsifthechild’sfunctionintheschool environ-mentisasexpectedforchildrenofthesameageandat thesameschoolyear.
• FamilyEnvironmentResourceInventory---FERI10:Itisa
questionnaireusedtoassessresourcesofthefamily envi-ronment, divided into threeareas: material resources, activities that signal family life stability and parent-ingpractices. To obtainthe relativescorein 10 points, the following formula wasused: raw score/topic maxi-mumscore×10,inwhichtherawscoreisthenumberof checkeditemsandthemaximumscoreisthetotal num-berofitems,exceptintopics8---10,whichhavespecific scores.Therelativescoreisusefultocomparethescores betweeninventoryitems.
DatawerecollectedfromJanuary2010toJanuary2012. Allchildren whoparticipatedin thisstudy wereevaluated byMABC-2test,theSFAandFERIquestionnaires,anda clas-sification of school performance was made based on the teachers’reports. The MABC-2 is one of the most widely used tests in research for the diagnosis of DCD and was usedinthisstudy toevaluatethe children’smotor devel-opment.The MABC-2 hasgoodlevels oftest-retest (0.75) andinter-raterreliability(0.70)11,12;ithasbeenusedin
dif-ferentcountriesandthereisevidenceofscorevalidityfor Brazilianchildren.13 AsMABC-2 isaperformance test,the
inter-rater reliabilitywas verified before data collection, yieldinganindexof0.80(IntraclassCorrelation).
standardizedforBrazilianchildren,North-Americanstudies supportthe validityand reliabilityof thistool.14 TheFERI
hasshowntobeusefultodifferentiatefamilyenvironment characteristics of children with different levels of school performance and behavior problems and has appropriate parametersoftest-retestreliability(0.92---1.00),aswellas goodinternal consistency(0.84).15 Althoughthisinventory
doesnothaveacut-off,ithasbeenusedinBraziltocompare groupsofchildren.
All children lived in the city of Uberlândia (MG), and all were evaluatedby the first author,previously trained to apply the tests and questionnaires. The SFA question-naireandinformationaboutschool performance(grading) wereappliedtogetherwiththechild’steacherinthechild’s school. On that visit, the first author explained to the teacheraboutthedrawingofonechild’snameinthesame classroomthechildwithDDattended.Thesechildrenwere subsequentlyevaluatedaftertheybroughtthesignedICF.
Thefirstauthorvisited35schools(20municipalschools, eightstateschools,sixprivateandonefederalschool)as, of the 45 children from the DD group, only ten students attendedthesameschool.Toenterthemunicipalschools, theresearcherhadtoobtaintheconsentfromthe Educa-tionSecretariat of theUberlândia MunicipalGovernment. Intheotherschools(state,federalandprivate),individual contactwasmade,andallschools receivedthe documen-tation demonstratingthat the children with DD had their parents’ permission (ICF) andthe study had the approval fromtheInstitutionalReviewBoardofAACD(No.09/2010) andtheInstitutionalReviewBoardofUniversidadeFederal deMinasGerais(COEP/UFMGNo.ETIC0482.0.203.000-10). The Statistical Package for Social Sciences (SPSS) for Windows, version 17.0, was used for data analysis. The descriptionofthegroupswasmadebymeasuresofcentral tendency(meanandstandarddeviation)orfrequency.The Shapiro-Wilk’snormalitytestwasapplied,whichfoundthat mostof the variableshad anormal distributionand thus, parametrictestswerechosen.AnalysisofVariance(ANOVA) wasusedforinferentialstatistics,aimingtoidentifypossible differencesbetweenthegroupsDDandtypicaldevelopment regardingthequantitativevariablesofmotorperformance, environmental resource and participation at school. The Binomial test for two proportions wasused for the cate-gorical variable performance in the academic content. A significancelevel≤0.05wasconsideredforallanalyses.
Results
Of the65 children from AACD/MG diagnosedwith DD, 45
(69.3%)participatedin thestudy,whereastheothers(20;
30.7%)werelostduetostudywithdrawal,movingtoanother
cityandchildrennotbeingfound.Therefore,theDDgroup
consistedof45childrendiagnosedwithDD,andthetypical
group consisted of 45 children with typical development,
selectedbynon-randomsampling,matchedbygender,age
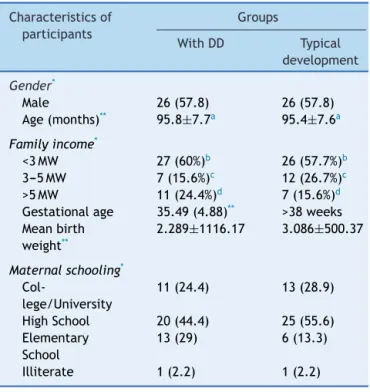
andhouseholdincome.Table1showsthedescriptive
infor-mationofthegroups.
IntheDD group,23(51.1%)children wereborn prema-turely,withgestationalagerangingfrom24to36weeks;in the neonatalperiod, 17 (37.8%) hadjaundice, 13 (28.9%) had seizures, 14 (31.1%) reported the need for oxygen
Table1 Characteristicsofchildrenwithdelayed neuropsy-chomotor development (DD) and typical development at schoolage.
Characteristicsof participants
Groups
WithDD Typical development
Gender*
Male 26(57.8) 26(57.8)
Age(months)** 95.8±7.7a 95.4±7.6a
Familyincome*
<3MW 27(60%)b 26(57.7%)b
3---5MW 7(15.6%)c 12(26.7%)c
>5MW 11(24.4%)d 7(15.6%)d
Gestationalage 35.49(4.88)** >38weeks
Meanbirth weight**
2.289±1116.17 3.086±500.37
Maternalschooling*
Col-lege/University
11(24.4) 13(28.9)
HighSchool 20(44.4) 25(55.6)
Elementary School
13(29) 6(13.3)
Illiterate 1(2.2) 1(2.2)
MW,minimumwages. n=45ineachgroup.
a p=0.794. b p=0.830. c p=0.197. d p=0.292.
* Frequency(percentage)ofchildrenineachcategory. ** Mean±standarddeviation.
supplementation, and 12 (26.7%) had signs of perinatal
hypoxia. Thetypicaldevelopmentgroupconsisted of
chil-dren born at term, with no record of relevant neonatal
complications.
ThechildrenfromtheDDgroupcommonlyhad,asinitial
developmentcharacteristics, motor delay (24;55.6%) and
suspectedlevelofdevelopmentintheareasofactivity(27;
60%)andparticipation(27;60%).The endofthe
multidis-ciplinaryintervention, whichlastedonaverage2.61±1.96
years,wasmainlyduetothefactthatmotordevelopment
hadbeenconsideredappropriateforage(41;91.1%).
Therewasameandifferencebetweenthe groupswith
statisticalsignificanceinallMABC-2areas(Table2).TheDD grouphadlowerperformanceinalltestdomains,withmost children from this group (28; 62.2%) showing motor diffi-culty,whilefour(8.9%)wereatriskformotordifficulty.In thetypicalgroup,five(11.1%)childrenhadmotordifficulty andsix(13.3%)wereatriskformotordifficulty.
Table2 Comparisonsbetweenpercentilesofmotorperformanceforthegroupswithdevelopmentaldelay(DD)andtypical development.
MABC-2 Mean±SD Minimum---maximum p-valuea
WithDD Typical WithDD Typical
Manualdexterity 20.1±26.2 48.7±31.2 0.5---98 2---99.9 <0.001
Throwingandgrasping 19.8±21.2 30±23.5 0.5---91 1---91 0.034
Balance 14±21.8 33.2±26 0.1---95 2---99 <0.001
Totalmotor 13.2±21.6 34.3±27 0.1---91 2---98 <0.001
MABC-2,movementassessmentbatteryforchildren;SD,standarddeviation;n,45ineachgroup. a ANOVA.
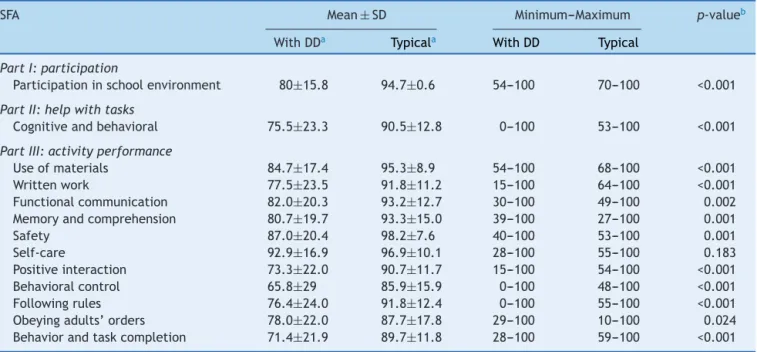
Table3 Comparativedataintheschoolparticipationquestionnairescoreforgroupswithdevelopmentaldelay(DD)andtypical development.
SFA Mean±SD Minimum---Maximum p-valueb
WithDDa Typicala WithDD Typical
PartI:participation
Participationinschoolenvironment 80±15.8 94.7±0.6 54---100 70---100 <0.001
PartII:helpwithtasks
Cognitiveandbehavioral 75.5±23.3 90.5±12.8 0---100 53---100 <0.001
PartIII:activityperformance
Useofmaterials 84.7±17.4 95.3±8.9 54---100 68---100 <0.001
Writtenwork 77.5±23.5 91.8±11.2 15---100 64---100 <0.001
Functionalcommunication 82.0±20.3 93.2±12.7 30---100 49---100 0.002 Memoryandcomprehension 80.7±19.7 93.3±15.0 39---100 27---100 0.001
Safety 87.0±20.4 98.2±7.6 40---100 53---100 0.001
Self-care 92.9±16.9 96.9±10.1 28---100 55---100 0.183
Positiveinteraction 73.3±22.0 90.7±11.7 15---100 54---100 <0.001 Behavioralcontrol 65.8±29 85.9±15.9 0---100 48---100 <0.001
Followingrules 76.4±24.0 91.8±12.4 0---100 55---100 <0.001
Obeyingadults’orders 78.0±22.0 87.7±17.8 29---100 10---100 0.024 Behaviorandtaskcompletion 71.4±21.9 89.7±11.8 28---100 59---100 <0.001
SFA,schoolfunctionassessment;SD,standarddeviation;n,45ineachgroup. a Meanrawdatatransformedtoascaleof0---100.
b ANOVA.
typical development group showed a consistent, superior
performanceinalltaskswhencomparedwiththeDDgroup.
ChildrenfromtheDDgrouphadlimitedperformance,
espe-cially in activities that required positive interaction (26;
57.8%),behavioralcontrol(26;57.8%)andcompletingtasks
(28;62.2%)(Table3).
Regarding academic performance, there were differ-ences between thegroups, with statisticalsignificance at levelsI(p=0.001)andII(p=0.008).Most(38;84.5%)ofthe childrenfromthetypicaldevelopmentgroupshowed mas-teryoftheacademic content(levelI---alphabeticand/or excellentgrading),andtherest(6,13.3%---levelII: syllabic-alphabetic or syllabic, good grading; 1, 2.2% --- level III: pre-syllabicand/or fairgrading) werein thedevelopment phase.Inthe DD group,most (24;53.3%)achievedlevel I andlevelII (17;37.8%),withonlyfour(8.9%)childrenstill receivingfairgrading.
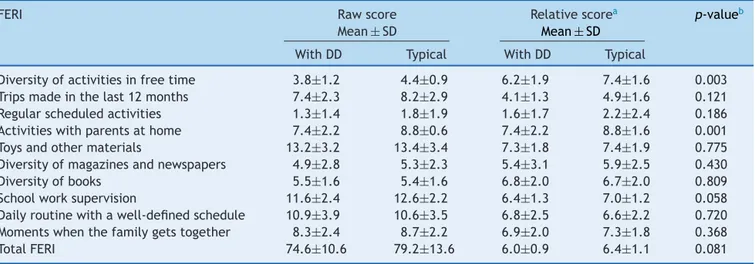
AsindicatedinTable4,althoughthereisadifferencein themeans betweengroups regarding theFERIitems,only twoindicators reachedstatisticalsignificance(p≤0.05).In
theDDgroup, childrenwereless activeintheirfree time andsharedfeweractivitieswiththeirparentsathome.
Discussion
AlthoughthetermDDiswidelyusedinBrazilianliterature,
littleis knownabout the outcome of thesechildren. This
study demonstrates that children with a diagnosis of DD
attaineduptotwoyearsofageshow,atschoolage,motor
limitations,restrictionsinschoolactivityperformance,low
participationinthe schoolcontext andsignificantlylower
functional performance when compared to the children
without a history of delay.Although children persist with
thedelay,thefunctionaloutcomewasbetterthanthemotor
one,suggestingthepossibilityofadaptation,whichis
con-sistentwiththeWHO---ICFperspective7thattheassociation
Table4 ComparativedataoftheFamilyEnvironmentResourceInventory(FERI)forgroupswithdevelopmentaldelay(DD)and typicaldevelopment.
FERI Rawscore
Mean±SD
Relativescorea
Mean±SD
p-valueb
WithDD Typical WithDD Typical
Diversityofactivitiesinfreetime 3.8±1.2 4.4±0.9 6.2±1.9 7.4±1.6 0.003 Tripsmadeinthelast12months 7.4±2.3 8.2±2.9 4.1±1.3 4.9±1.6 0.121 Regularscheduledactivities 1.3±1.4 1.8±1.9 1.6±1.7 2.2±2.4 0.186 Activitieswithparentsathome 7.4±2.2 8.8±0.6 7.4±2.2 8.8±1.6 0.001 Toysandothermaterials 13.2±3.2 13.4±3.4 7.3±1.8 7.4±1.9 0.775 Diversityofmagazinesandnewspapers 4.9±2.8 5.3±2.3 5.4±3.1 5.9±2.5 0.430
Diversityofbooks 5.5±1.6 5.4±1.6 6.8±2.0 6.7±2.0 0.809
Schoolworksupervision 11.6±2.4 12.6±2.2 6.4±1.3 7.0±1.2 0.058 Dailyroutinewithawell-definedschedule 10.9±3.9 10.6±3.5 6.8±2.5 6.6±2.2 0.720 Momentswhenthefamilygetstogether 8.3±2.4 8.7±2.2 6.9±2.0 7.3±1.8 0.368
TotalFERI 74.6±10.6 79.2±13.6 6.0±0.9 6.4±1.1 0.081
SD,standarddeviation;n,45ineachgroup.
aRelativescore:meanrawdatatransformedtoascalefrom0to10. b ANOVA,relativescore.
Itisknownthattheriskfactorsfordelayaremultipleand
theaccretionofconditionscandetermineahigherimpacton
childdevelopment.16,17ChildrenfromtheDDgroupincluded
in this study came from low-income families, with most familiesreceivinglessthanthreeminimumwages,andthe majorityofthe mothershadonlyhigh-schoollevel educa-tion.Additionally,51.1%ofchildrenintheDD grouphada historyofprematurity,lowbirthweightandneonatal neu-rologicalcomplications. Although one cannotexclude the effectofotherfactorsnotassessedontheoutcomeofthe DDgroup,biologicalrisk,representedespeciallyby prema-turity,was decisiveon theother factors. As discussed by someauthors,18,19in spiteofthelowinvestmentin
deter-miningtheetiology,manystudiesindicatebiologicalfactors as determinants of most DD cases. In the study of Srour etal.,20 for instance,which investigatedthe causeofthe
delaythroughclinicalandlaboratorytests,theetiologyof 77% of the cases wasidentified, and brain malformation, hypoxic-ischemicencephalopathyandchromosomal abnor-malitieswerethemostcommoncauses.
Thehighfrequency(62.2%)ofmotordisordersatschool age found in the DD group corroborates the literature. A meta-analysisby Williams et al.,21 includingstudies on
school children born prematurely, indicated a prevalence ofupto40.5%ofmotoralterationsversus6%inthegeneral population.Althoughthetypicalgroupalsoincludeschildren withmotordifficulties(11.1%),thefrequencywascloseto thatexpectedforthegeneralpopulation,asobservedinthe studybyGoyenandLui22 who,whenassessingpretermand
full-terminfantswiththeMABC-2test,foundaprevalence ofmotordeficitof42%inthepretermand8%inthefull-term infants.
As for school performance,measured by the academic contentdomain according tothe teacher’sassessment, it was observed that just a little over half (53.3%) of the children from the DD group had excellent grading, indi-cating advancement in the literacy process. It is worthy notingthat,evenin thepresenceofmotor alterations,as mentionedbefore,thesechildrenachievedmasteryofthe academiccontent.Eventhoughthechildrenpersistedwith
thedelay,thefunctionaloutcomewasbetterthanthemotor one,suggestingthatchildrenareabletoadaptorthatitis possibletomodifytheenvironmenttofacilitate participa-tionandlearning.5
ChildrenfromtheDDgroup,however,hadworsescoresin allareasofschoolparticipationintheSFAandonly22.2%of them,versus66.7%inthetypicaldevelopmentgroup, effec-tivelyparticipatedintheschoolenvironment,without the needforextrahelpincognitiveandbehavioraltasks.Riou etal.5alsofoundthatonly17%ofchildrenwithDD
partic-ipatedin the classroom without help. Possibly, the motor delay, asrecorded in this study,had more impacton the performance of the necessary activities to participate in class(e.g.handling materials,written work) thanon aca-demic performance measured byliteracy, which does not necessarilyrequirethemotorcomponent.
Thestudy’slimitationsincludetheuseofimportedtests, withoutfullyvalidatedcut-offsfortheBrazilianpopulation, usingtheteachers’reportstoclassifytheacademic perfor-mance,andthefactthatitisaconveniencesample.Foreign testshavebeenroutinelyusedinBrazilianstudies,andthe MBC-2wasrecentlyvalidated.13Additionally,carewastaken
to collect comparative data. As many children in the DD grouphadliteracyproblems,itwouldbeimportantto per-forma language assessment, whichshould beincluded in futurestudies.Teachers’reportswereusedinotherstudies, suchastheonebyPritchardetal.,23which,when
compar-ing thequalitative teacher’sevaluationwithstandardized measurements,foundthatthereportdetectedtwotothree times morechildren likelyto have learningdifficulties. It is recommendedthat futurestudies leave the rehabilita-tion center contextto includea broader population from basic health units,in ordertoinvestigate theoutcome of milderandmorevariedcasesofDD,asitcanprovide neces-sarystatisticalpowertodetectdifferencesinenvironmental factors.
asignoffutureconditionsthatshouldbebettermonitored anddiagnosedasearlyaspossible.Themonitoringshouldbe performedatleastuntilschoolage,inordertoidentifythe needsastheyarise,minimizingproblemsatschoolageand adulthood.Sporadicevaluationscanhelpprofessionalsand parentsunderstandwhatishappening,soadequatesupport canbeprovidedtothechilduptothe‘‘finaldiagnosis’’ defi-nition,asthe‘‘DD’’termshouldbeusedonlyasatemporary diagnosis.
Funding
CNPq---No.483652-2011-3.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
References
1.ShevellMI. Global developmentaldelayand mental retarda-tionorintellectualdisability:conceptualization,evaluationand etiology.PediatrClinNorthAm.2008;55:1071---84.
2.Shevell MI, Majnemer A, Platt RW, Webster R, Birnbaum R. Developmentalfunctionaloutcomesatschoolageofpreschool children with global developmental delay. J Child Neurol. 2005;20:254---65.
3.MannJR,CrawfordMS,WilsonL,McDermottS.Doesrace influ-enceageofdiagnosisforchildrenwithdevelopmentaldelay?J DisabilHealth.2008;1:157---62.
4.Shevell MI, Majnemer A, Platt RW, Webster R, Birnbaum R. Developmental functional outcomes in children with global developmentaldelayordevelopmentallanguageimpairment. DevMedChildNeurol.2005;47:678---83.
5.RiouE,GhoshS,FrancouerE,ShevellMI.Globaldevelopmental delayanditsrelationshiptolatercognitiveskills.DevMedChild Neurol.2009;2:145---50.
6.ShevellMI,AshwalS,DonleyD,FlintJ,GingoldM,HirtzD,etal. Practiceparameter:evaluationofthechildwithglobal develop-mentaldelay:reportoftheQualityStandardsSubcommitteeof theAmericanAcademyofNeurologyandThePractice Commit-teeoftheChildNeurologySociety.Neurology.2003;60:367---79. 7.Organizac¸ãoMundialdeSaúde.CIF:Classificac¸ãoInternacional deFuncionalidade,IncapacidadeeSaúde.Traduc¸ãodoCentro ColaboradordaOrganizac¸ãoMundialdaSaúdeparaaFamíliade Classificac¸õesInternacionais.SãoPaulo:EDUSP;2003.
8.Henderson SE, Sugden DA,Barnett A. Movement assessment batteryforchildren-2(MABC-2).2nded.SanAntonio,TX:The PsychologicalCorporation;2007.
9.CosterWJ,DeeneyT,HaltiwangerJ,HaleyS.Schoolfunction assessment.SanAntonio:Pearson;1998.
10.MarturanoEM.OInventáriodeRecursosdoAmbienteFamiliar ---RAF.PsicolReflexCrit.2006;19:498---506.
11.VanWelvelde H,WeerdtW, De CockP,Smits-EngelsmanBC. Aspectsofthevalidityofthemovementassessmentbatteryfor children.HumMovSci.2004;23:49---60.
12.WilsonPH.Practitionerreview:approachestoassessmentand treatmentofchildrenwithDCD:anevaluativereview.JChild PsycholPsychiatry.2005;46:806---23.
13.ValentiniNC,RamalhoNH,OliveiraNA.Movementassessment batteryforchildren-2:translation,reliability,andvalidityfor Brazilianchildren.ResDevDisabil.2014;35:733---40.
14.Hwang JL, Davies PL, Taylor WJ, Gavin WJ. Validation of schoolfunctionassessmentwithprimaryschoolchildren.OTJR. 2002;22:48---58.
15.D’Ávila-BacarjiKM,MarturanoEM,EliasLC.Recursose adver-sidades no ambiente familiar de crianc¸as com desempenho escolarpobre.Paideia.2005;15:43---55.
16.HalpernR,BarrosFC,HortaBL,VictoraCG.Estadode desen-volvimentoaos12mesesdeidadedeacordocompesoaonascer erendafamiliar:umacomparac¸ãodeduascoortesde nascimen-tosnoBrasil.CadSaúdePública.2008;24:444---50.
17.Moura DR, Costa JC, Santos IS, Barros AJ, Matijasevich A, HalpernR,etal.Naturalhistoryofsuspecteddevelopmental delaybetween 12and24monthsofageinthe2004 Pelotas birthcohort.JPaediatrChildHealth.2010;46:329---36. 18.Mc Donald L, RennieA, Tolmie J, GallowayP, McWulliam R.
Investigationofglobaldevelopmentaldelay.ArchDisabilChild. 2006;91:701---5.
19.MarturanoEM,FerreiraMC,D’Avila-BacarjiKM.Anevaluation scaleoffamilyenvironmentfortheidentificationofchildrenat riskofschoolfailure.PsycholRep.2005;96:307---21.
20.Srour M, Mazer B, Shevell MI. Analysis of clinical features predictingetiologicyieldintheassessmentofglobal develop-mentaldelay.Pediatrics.2006;118:118---39.
21.Williams J, Lee KJ, Anderson PJ. Prevalence of motor-skill impairment in preterm children who do not develop cere-bral palsy: a systematic review. Dev Med Child Neurol. 2010;52:232---7.
22.Goyen TA, Lui K. Developmental coordination disorder in ‘‘apparentlynormal’’schoolchildrenbornextremelypreterm. ArchDisChild.2009;94:298---302.