w w w . r b o . o r g . b r
Case
report
Parosteal
aneurysmal
bone
cyst
夽
Walter
Meohas,
Ana
Cristina
de
Sá
Lopes,
João
Victor
da
Silveira
Möller
∗,
Luma
Duarte
Barbosa,
Marcelo
Braganc¸a
dos
Reis
Oliveira
InstitutoNacionaldeTraumatologiaeOrtopedia(Into),RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received4June2014 Accepted23October2014 Availableonline1September2015
Keywords:
Aneurysmalbonecyst Calcitonin
Corticosteroids Infiltration
a
b
s
t
r
a
c
t
The incidenceofaneurysmalbonecystsis0.14casesper100,000individuals.Parosteal aneurysmalbonecystsaretheleastprevalentsubtypeandrepresent7%ofallaneurysmal bonecysts.We presentthecaseofa38-year-oldmale patientwithpain andbulgingin hisrightarm foreightmonths.Hehadpreviouslybeendiagnosedaspresenting giant-celltumor,buthisslideswerereviewedandhisconditionwasthendiagnosedasparosteal aneurysmalbonecyst.Thepatientwastreatedwithcorticosteroidandcalcitonininfiltration intothelesionandevolvedwithclinicalandradiologicalimprovementwithinthefirstfive weeksaftertheoperation.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Cisto
ósseo
aneurismático
parosteal
Palavras-chave:
Cistoósseoaneurismático Calcitonina
Corticosteroides Infiltrac¸ão
r
e
s
u
m
o
Ocistoósseoaneurismáticotemumaincidênciade0,14acada100milindivíduos.Osubtipo parostealéomenosprevalente,representa7%detodos.Apresentamosumpaciente mas-culino,38anos,comdoreabaulamentoembrac¸odireitohaviaoitomeses.Diagnosticado previamentecomotumordecélulasgigantes,tevesualâminarevisadaeentãofoifeitoo diagnósticodecistoósseoaneurismáticoparosteal.Opacientefoitratadocominfiltrac¸ão intralesionaldecorticosteroideecalcitoninaeevoluiucommelhoriaclínicaeradiológicajá nasprimeirascincosemanaspós-operatórias.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Todososdireitosreservados.
夽
WorkperformedattheInstitutoNacionaldeTraumatologiaeOrtopedia(INTO),RiodeJaneiro,RJ,Brazil. ∗ Correspondingauthor.
E-mails:[email protected],[email protected](J.V.daSilveiraMöller).
http://dx.doi.org/10.1016/j.rboe.2015.08.008
602
rev bras ortop.2015;50(5):601–606Introduction
AneurysmalbonecystswerefirstdescribedbyJaffeand Lich-tensteinin1942.1Theyaccountfor1–2%ofallprimarybone tumorsand affectthemetaphyseal regionoflong bonesin children,adolescentsandyoungadults.2,3
Thislesiontypicallydevelopsinsidebones.4Cystslocated inthe cortical boneare rare and account for7–9.3% ofall aneurysmalbonecysts.5,6
Few cases have been reported in the literature. The approachusedisindividualizedandvariesaccordingtothe experience ofeach service.We presenta caseofparosteal aneurysmalbonecystthatwastreatedinaccordancewithour experience.
Case
report
Thepatientwasa38-year-oldmanofmixedracewitha com-plaintofpainandbulginginhisrightarm.Itwasofprogressive natureand the patient had had the complaintforat least eightmonths.Hesaidthathehadnotsufferedanytrauma orundergoneprevioussurgery.
Thepatient,whohadbeenattendedpreviouslyatanother service,underwentabiopsyfromwhichthehistopathological diagnosiswascompatiblewithagiant-celltumor.Whenhe arrivedatourservice,becauseoftheclinicalandradiological characteristicsoftheslides(Figs.1–4),areviewofthemwas requested.
Fig.1–Radiographsoftherighthumerusinanteroposteriorandlateralview.
Thisreview showedthe presenceofalesion formedby cystmembranesthatsometimesshowedcompleteseptation constitutedbyfusiformandmultinucleatedgiantcells.Bone trabeculaedissociatedbyconnectivetissuewerenoted,along withneoformedbonetrabeculaeofreactivepattern,whichled tothediagnosisofparostealaneurysmalbonecyst.
Infiltration intothe lesionusingcalcitonin and corticos-teroidwasindicatedafterreachingagroupdecision.Inthe fifthpostoperativeweek,the lesionwasalready seentobe undergoinganossificationprocess(Fig.5).
Discussion
AneurysmalbonecystswerefirstdescribedbyJaffeand Lich-tensteinin1942.AccordingtotheWorldHealthOrganization, theyarecharacterizedasbenigncysticbonelesionscomposed ofbonevoidsthatarefilledwithbloodandseparatedbysepta ofconnectivetissuecontainingfibroblasts,osteoclasticgiant cellsandreactivebonetissue.1–3,7
Thesecystsaccountfor1–2%ofallprimarybonetumors and their incidence is 0.14 per 100,000 individuals.8 The lesions affect the metaphyseal regionofthe long bonesof children,adolescentsandyoungadults.2,3
Fig.2–Tomographicfeatures.
subperiostealgiantcells,hemangiomasand osteogenic sar-comas.
In1957,ShermanandSoong5classifiedaneurysmalbone cystsintothreetypes:eccentric,parostealand central.The parostealsubtypeistheleastfrequentsubtype,accounting for7–9.3%ofallaneurysmalbonecysts.5,6
604
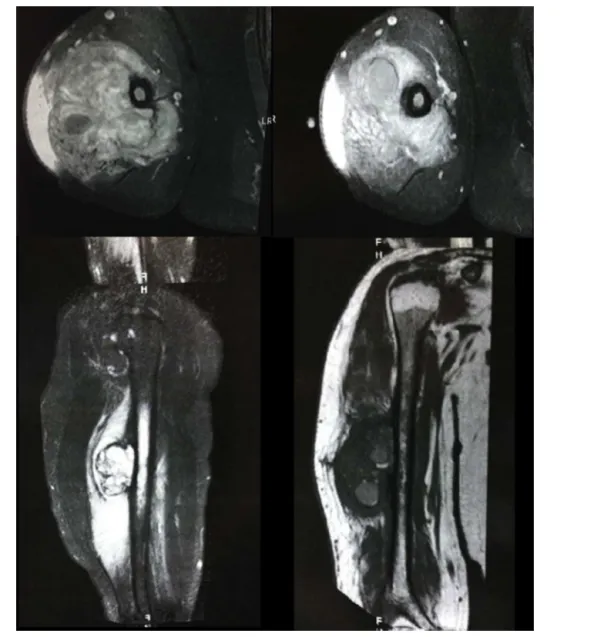
rev bras ortop.2015;50(5):601–606Fig.3–Magneticresonance.
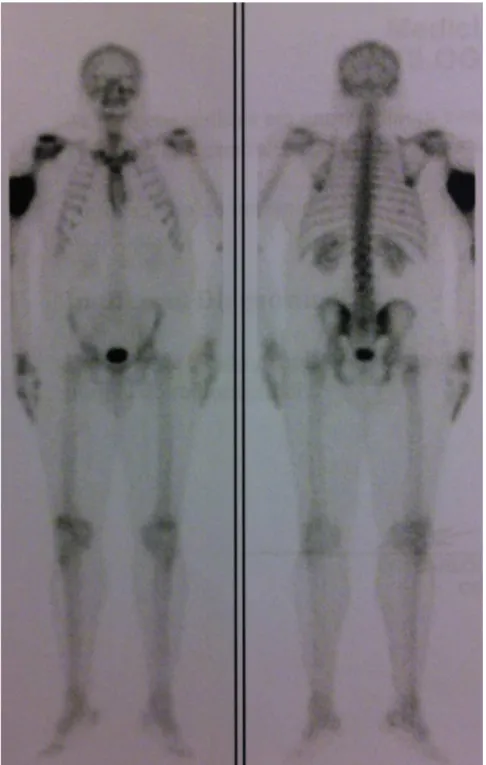
Tomography helps in making the differential diagnosis ofthese lesions.Theyshow liquiddensityand mayclearly demonstratetheliquidlevels.2,6Scintigraphyshowsthatthere isgreateruptakeattheperipheryofthelesion.2Inmagnetic resonanceimaging,thelesioniswelldefined,withlobulated outlinesandliquidlevels.2
The histology of aneurysmal bone cysts is character-ized by voids filled with blood. These voids are covered bya singlelayer ofundifferentiated cells.The solid tissue surrounding the lesion is composed ofrichly vascularized fibrosis.2Diagnosticdifferentiationbetweengiant-celltumors andosteosarcomawithtelangiectasiais anatomopathologi-callycomplex.2
Becausetheseareaggressivelesions,thetreatment con-sistsofcurettage,withorwithoutsubsequentadjuvantssuch
as bone grafts, bone marrow aspirate, cryotherapy, argon, phenol or calcitonin with corticosteroid injection into the lesion.7,10 In our service, use ofcorticosteroids in associa-tionwithcalcitonin,injectedintothelesion,isthepreferred methodfortreating thistypeoflesion.Casesofresolution oflesionsafteranepisodeoffracturingorafterabiopsy,or evenspontaneously,havebeendescribed.7,8Lesionrecurrence isassociatedwithyoungpatients,previousaneurysmalbone cysts,locationadjacenttoajointorgrowthplate,lowmitotic countandpresenceofotheropengrowthplates.8
606
rev bras ortop.2015;50(5):601–606Fig.5–Postoperativeradiographs.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. JaffeHL,LichtensteinL.Solitaryunicameralbonecyst:with emphasisontheroentgenpicture.Thepathologicappearance andthepathogenesis.ArchSurg.1942;44(6):1004–25.
2. Jesus-GarciaR.Diagnósticoetratamentodetumoresósseos. 2nded.RiodeJaneiro:Elsevier;2013.
3. PietschmannMF,OliveiraAM,ChouMM,IhrlerS,
NiederhagenM,Baur-MelnykA,etal.Aneurysmalbonecysts ofsofttissuerepresenttrueneoplasm.Areportoftwocases.J BoneJointSurgAm.2011;93(45):1–8.
4. KobayashiS,HayakawaK,TakenoK,BabaH,MeirA.Parosteal aneurysmalbonecystofthehumeruswithbirdcage-like
ossificationonthree-dimensionalCTscanning:acasereport. JointBoneSpine.2009;76(6):705–7.
5.ShermanRS,SoongKY.Aneurysmalbonecyst:itsroentgen diagnosis.Radiology.1957;68(1):54–64.
6.DeDiosAMV,BondJR,ShivesTC,McLeodRA,UnniKK. Aneurysmalbonecyst.Aclinicopathologicstudyof238cases. Cancer.1992;69(12):2921–31.
7.ReddyKIA,SinnaeveF,GastonCL,GrimerRJ,CarterSR. Aneurysmalbonecysts:dosimpletreatmentswork?Clin OrthopRelatRes.2014;472(6):1901–10.
8.SteffnerRJ,LiaoC,StacyG,AtandaA,AttarS,AvedianR,etal. Factorsassociatedwithrecurrenceofprimaryaneurysmal bonecysts:isargonbeamcoagulationaneffectiveadjuvant treatment?JBoneJointSurgAm.2011;93(21):e1221–9.
9.LichtensteinL.Aneurysmalbonecyst:apathologicalentity commonlymistakenforgiantcelltumorandoccasionallyfor hemangiomaandosteosarcoma.Cancer.1950;3(2):279–89.