w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
The
importance
of
lactic
acid
in
migraines
and
fibromyalgia
夽
Guido
Assis
Cachuba
de
Sá
Ribeiro
a,
Rosana
Hermínia
Scola
a,b,
Elcio
Juliato
Piovesan
a,c,
Darley
Rugeri
Wollmann
Junior
d,
Eduardo
dos
Santos
Paiva
e,
Claudio
Leinig
Pereira
da
Cunha
a,d,
Lineu
Cesar
Werneck
a,b,∗aInternalMedicineandHealthSciencesPost-GraduationProgram,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil bNeuromuscular/Neurology,HospitaldeClínicas,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
cHeadacheUnit/Neurology,HospitaldeClínicas,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil dCardiology/InternalMedicine,HospitaldeClínicas,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil eRheumatology/InternalMedicine,HospitaldeClínicas,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20February2014 Accepted17February2015 Availableonline8September2015
Keywords:
Chronicmigraine Episodicmigraine Lacticacid Fibromyalgia
a
b
s
t
r
a
c
t
Background:Lacticacidisabyproductofbothmusclemetabolismandthecentralnervous system.Changesinmetabolismarerelatedtovariousphysiologicalandpathological con-ditions.Theaimofthisstudywastodeterminetherelationshipbetweenmigraineand fibromyalgiawiththelevelsoflacticacidintheblood.
Methods:Westudy93patientsdividedintofivegroups:(1)patientswithfibromyalgia(n=20); (2) episodic migraine(n=20);(3) chronicmigraine (n=20); (4)fibromyalgiaand episodic migraine(n=13);and(5)fibromyalgiaandchronicmigraine(n=20),and20 healthy sub-jects(controlgroup).Bloodlevelsoflacticacidweremeasuredatfourdifferenttimepoints: atrest,duringaerobicexercise,duringanaerobicphysicalactivityandwhilerestingafter anaerobicexercise.
Results:Lacticacidincreasedinallgroupsduringanaerobicphysicalactivitywithout pre-dominanceforeithergroup.Duringaerobicphysicalactivity,allgroupsincreasedlacticacid levels,buttheincreasewasmoreexpressiveinthechronicmigrainegroupandthechronic migrainewithfibromyalgiagroupwithoutstatisticalsignificance.
Conclusions: We didnot foundabnormalitiesinvolvingthe metabolism oflactic acidin episodicandchronicmigrainewithorwithoutfibromyalgia.
©2015ElsevierEditoraLtda.Allrightsreserved.
夽
ThestudywasconductedattheNeurology,CardiologyandRheumatologyServices,HospitaldeClínicas,UniversidadeFederaldo Paraná(UFPR),Curitiba,PR,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](L.C.Werneck).
http://dx.doi.org/10.1016/j.rbre.2015.08.012
A
importância
de
ácido
láctico
na
enxaqueca
e
na
fibromialgia
Palavras-chave:
Enxaquecacrônica Enxaquecaepisódica Ácidoláctico Fibromialgia
r
e
s
u
m
o
Introduc¸ão: Oácidolácticoéumsubprodutodometabolismomuscularedosistemanervoso central.Asalterac¸õesnometabolismoestãorelacionadascomdiversascondic¸ões fisiológ-icasepatológicas.Oobjetivodesteestudofoideterminararelac¸ãoentreaenxaquecaea fibromialgiacomosníveisdeácidolácticonosangue.
Métodos: Foramestudados93pacientes,divididosemcincogrupos:1)fibromialgia(n=20); 2)enxaquecaepisódica(n=20);3)enxaquecacrônica(n=20);4)fibromialgiaeenxaqueca episódica(n=13);e 5)fibromialgiae enxaquecacrônica (n=20), além de20 indivíduos saudáveis(grupocontrole).Osníveissanguíneosdeácidolácticoforammedidosemquatro momentos:emrepouso,duranteoexercícioaeróbico,duranteaatividadefísicaanaeróbica eduranteodescansodepoisdoexercícioanaeróbico.
Resultados: O ácido láctico aumentou em todos os grupos durante a atividade física anaeróbica,sempredominânciaemqualquergrupo.Duranteaatividadefísicaaeróbica, todososgruposapresentaramumaumentonosníveisdeácidoláctico,masesseaumento foimaisexpressivonosgruposdeenxaquecacrônicaeenxaquecacrônicacomfibromialgia, semsignificânciaestatística.
Conclusões: Nãoforamencontradasanormalidadesqueenvolvessemometabolismodo ácidolácticonaenxaquecaepisódicaecrônica,napresenc¸aounãodefibromialgia.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Migraineisachronicneurologicaldisorderwithhigh preva-lenceand severe impacton apatient’s quality oflife.This disorderhasgeneticcharacteristicsthatmodulatea dysfunc-tioninbrainelectricalactivity.Thisneurologicalconditionis characterizedbyrecurrentepisodesofheadachewith unilat-eralthrobbingcharacteristicsofmoderatetostrongseverity thatworsenswithphysicalactivity.Thisworseningis associ-atedwithvomiting,nausea,phonophobiaandphotophobia.1,2
Many biochemical changes can beobserved duringand
betweenmigraineattacks.Lacticacidlevels,forexample,may be altered, exhibiting an increase compared with patients
with tension-type headache and healthy controls.3 These
datasuggest thatmigrainepatientshaveanabnormalityin mitochondrialmetabolism.Itwasdemonstratedthatlactate levelswithinthevisualoccipitalcortexiselevatedinmigraine patientsduringtheinter-ictalperiodand couldsuggestthe presenceofanaerobicglycolysisincorticalregions.4However,
other studies have notconfirmed these changes and,as a
result,donotsupportthishypothesis.5
Lacticacidusuallyincreasesduringhigh-intensityphysical activityandisrelatedtoadeclineinmusclestrengthandpain generationduringexercise.6–8Additionally,theincreasein lac-ticacidobservedduringexercisehasbeenshowntotrigger migraineattackswithaura.9,10 Despitethis causal relation-ship,lacticacidisnotconsideredanalgogenicsubstance.11
Fibromyalgia is a chronic pain condition of unknown
etiology characterized by widespread spontaneous muscle
pain and tenderness to palpation. The diagnostic criteria
usedforfibromyalgia comesfrom the American Collegeof
Rheumatology2009and2010.12,13Fibromyalgiacanalso dis-playco-morbidities,suchaspsychiatricdisordersandother
pain syndromes. Thecorrelationbetweenfibromyalgia and
migraine variesfrom22 to50% ofcases.14 Thisassociation contributes to a decreased quality of life forpatients and enhances thepresenceofco-morbidities.The pathophysio-logicalrelationshipbetweenthesetwodisordershasnotyet beenestablishedinthemedicalliterature.
Patientswithfibromyalgiamayexperiencehigh levelsof lactic acid atrest15,16 or during aerobicphysical activity.17 However,otherstudiesshowthatchangesinglycolysisand lactic acid at rest or during physical activity were slight increasedamongfibromyalgiapatients.18,19
Theratiooflacticacidproductioninpatientswithmigraine andfibromyalgia,aswellastheinfluenceofthismetabolite inthepathophysiologyofthesediseases,iscontroversialor nonexistent.Thegoalofthisstudyistodeterminewhether themetabolismoflacticacidchangedinepisodicmigraineor chronicmigraine,withorwithoutassociatedfibromyalgia.
Patients
and
methods
We selected from out-patient headache clinic cases with
chronicandepisodicmigrainewhowerealsosufferingfrom fibromyalgia and from the out-patient rheumatology clinic forpatientswithonlyfibromyalgia.Allpatientswithchronic
and episodic migraine met the criteria proposed by the
Medications
Aportionofpatientscontinuouslyusedoneormoreofthe fol-lowingmedications:selectiveinhibitorsofserotoninuptake (n=23), tricyclic antidepressants (n=20), selective
recep-tor of serotonin inhibitors, norepinephrine and dopamine
(n=5), antipsychotics/dopamine blockers (n=6), benzodi-azepines (n=14), sleep inducers (n=1), muscle relaxants (n=19),anti-inflammatorydrugs(n=9),antimalarials(n=2), antihistaminesforallergy(n=4),statins(n=3),protonpump blockers(n=6),anticonvulsants(n=10),angiotensin convert-ing enzyme inhibitors (n=10), diuretics (n=10), oral anti-coagulants(n=1), alendronate (n=1), levothyroxine (n=15), metformin,insulinandorlistat(n=4).
Symptomsduringtesting
Thetestswereperformeddespitethepainfulmuscle symp-tomsinpatientswithfibromyalgia.Thepatientswithepisodic
migraine underwent the test only if they were free of a
headachecrisisforatleastfivedays.Patientswithchronic migraineweretestedduringperiodsoflowerheadache inten-sity.
Exercisestresstesting
Thepatientsunderwentexercisestresstestingusinga tread-millwith progressiveincrementsofeffort and whileusing thesoftwareMicromedErgoPC13.Initially,thepatientshadan electrocardiogramatrest(baselinecontrolphase)followedby exerciseswithameandurationof30min.Thetreadmillwas inaflatposition,startedatspeedsof2.0mphandincreased
by 1.0mph every minute until reaching 9.0mph. The test
wasdividedintodifferentstages:aerobic,anaerobicexercise andrestpostexercise.Todifferentiatebetweenaerobicand anaerobicexercise,weusedtheKarvonenformula(220minus subjectage=maximumheartratefortheage).Weconsidered aerobicmetabolicactivitywhentheheartratewasbetween 50and69%ofthepredictedvaluefoundintheKarvonen for-mulafortheageandanaerobicexercisewhentheheartrate wasfrom70%to85%ofthepredictedmaximum.Allsubjects sustainedtheexerciseatthenecessaryheartrateforatleast 3min.19Allsubjectswereconsideredtobesedentary.
Lacticaciddetermination
Lacticacidwasdeterminedbycapillarybloodsamplesviaa transdermalskinpunchoftheleftindexfingeratfourtime points: (1) restingbaseline beforeexercise; (2) after10min ofaerobicactivity;(3)after3minofanaerobicactivity;and (4)after6minofrestfollowinganaerobicexercise.Adropof bloodwasplacedonaspecificpapertape(RocheDiagnostics Brazil)andintroducedintoadeviceforreflectancephotometry (AccutrendLactate,Roche Diagnostica, Brazil),which auto-maticallydeterminedthelevelsoflacticacid.
Ethicsstudy
All patients signed an informed consent form.The
proce-duresinthis studywereapprovedbythe ethicscommittee
forhumanresearchattheHospitaldeClinicas,Universidade FederaldoParaná.
Statisticalanalysis
Inadditiontodescriptivestatisticaltests,weusedthet-test forindependentsamples(homogenizationofcases)andthe
Mann–WhitneyUtestformakingcomparisonsbetweenthe
levelsoflacticacidinthevariousstagesofthestudy(p<0.05 forstatisticalsignificance).Toconfirmtheresultsweapplied theBonferronicorrection.Statisticalanalysisandplotswere doneusingtheSPSSsoftwareversion11.0(Chicago,IL).
Results
Studysubjects
Thestudysubjectsweregroupedbyage,weight,heightand bodymassindex(BMI).Allsubjectsandcontrolswerefemales. Patientsweredividedintosixgroups:GroupI–thehealthy subjects using no medication (n=20); Group II – patients withonlyfibromyalgia(n=20);GroupIII–patientswithonly episodic migraine (n=20); Group IV – patients with only chronicmigraine(n=20);GroupV–patientswith fibromyal-giaplusepisodicmigraine(n=13);andGroupVI–patientswith fibromyalgiapluschronicmigraine(n=20)(Table1).Allgroups weresimilar,andtherewasnostatisticallysignificant differ-encebetweenthemwithrespecttoage,weight,heightorbody massindex(BMI)(Table1).
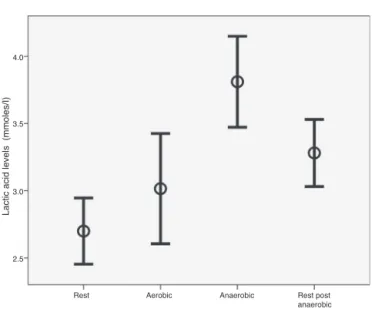
Lacticacidbloodlevels
Thelacticacidwasmeasuredin113casesinfouroccasions (452 analyses): the baseline phase, aerobic phase, anaero-bic phase and rest after physical activity. The lactic acid
average of all groups underwent elevation during
anaer-obic activity and remained high during the rest period.
Comparison of all subjects lactic acid level at the
base-line phase (2.70±1.32mmol/L) with the anaerobic phase
(3.81±1.81mmol/L)showedasignificantincrease(p=0.0001). The lactic acid level at the baseline phasecompared with the post-exercise rest (3.28±1.34mmol/L)was also signifi-cant(p=0.001).Theaerobicphaselacticacidalsoincreased (3.01±2.20mmol/L)but wasnotsignificantlydifferentfrom thebaseline(p=0.125)(Fig.1).
No significant difference was found between aerobic
exercises when compared with the baseline phase in all
groups.Anaerobicexerciseincreasedthelacticacidcompared with baselineinthe controlgroup(p=0.0001),fibromyalgia group (p=0.0001) and chronic migraine group (p=0.008). In the post-exercise rest group, the lactic acid remained ele-vated in the control group (p=0.008) and the fibromyalgia group(p=0.003).Inthegroupsofepisodicmigraine,chronic migraine, fibromyalgia plus episodic migraine and chronic migraineplusfibromyalgia,thelevelsoflacticacidremained slightlyelevatedornearthebasalcontrolwithoutstatistical significance(Table2).
Table1–Subjectscharacteristicsofthecontrols,fibromyalgiaandmigrainecases.
Group Numberofcasesa Age(years-old)
Mean±SD Min–max
Weight(kg) Mean±SD
Min–max
Height(m) Mean±SD Min–max
Bodyindex mass Mean±SD
Min–max
Controls 20 42.60±9.36
(22–56)
66.75±9.15 (53–84)
1.64±0.76 (1.53–1.80)
24.95±3.90 (18.59–34.17) Fibromyalgia 20 47.35±6.33
(32–57)
65.75±12.38 (46–90)
1.60±0.54 (1.49–1.70)
25.65±4.98 (18.81–34.07) Episodicmigraine 20 37.75±10.54
(21–59)
65.95±12.68 (46–90)
1.62±0.67 (1.50–1.76)
25.24±5.21 (17.85–35.15) Chronicmigraine 20 39.15±12.13
(26–67)
65.15±11.88 (45–100)
1.60±0.78 (1.47–1.79)
25.71±5.34 (20.00–42.16) Episodicmigraine
plusfibromyalgia
13 46.92±8.64 (30–62)
71.08±4.70 (65–80)
1.61±0.55 (1.53–1.72)
27.33±2.35 (23.87–30.86) Chronicmigraine
plusFibromyalgia
20 44.30±6.45 (31–57)
66.45±12.39 (44–92)
1.61±0.73 (1.50–1.76)
25.56±4.16 (19.04–31.59)
SD,standarddeviation;min,minimal;max,maximal.
a Allcaseswerefemales.
Table2–Lacticacidlevelsatrestandthetypeofexercisesphases.
Group Numberofcases Rest(mmol/L)
Mean±SD
Aerobic (mmol/L) Mean±SD
Anaerobic (mmol/L) Mean±SD
Restpost exercise (mmol/L) Mean±SD
Controls 20 2.39±0.88 2.82±2.41 3.64±1.31 3.34±1.24
Fibromyalgia 20 2.33±1.08 2.38±1.71 4.32±1.96 3.37±1.56
Episodicmigraine 20 2.93±1.38 3.22±2.70 3.22+0.96 3.25±1.39
Chronicmigraine 20 2.79±1.25 3.40±1.91
p=0.048a
4.21±1.56 3.44±1.19
Episodicmigraineplusfibromyalgia 13 2.40±0.83 2.05±0.81 4.15±3.40 3.05±1.60 Chronicmigraineplusfibromyalgia 20 3.23±1.95 3.87±2.53
p=0.042a
3.43±1.48 3.16±1.27
SD,standarddeviation.
a StatisticalsignificanceinrelationtothecontrolgroupbeforeBonferroniCorrection(Mann–WhitneyUtest).
thephasesofanaerobicexerciseandrestafterexercisephase. Intheaerobicphasewefoundthatthelevelsoflacticacid increasedinthechronicmigrainegroup(p=0.048)andchronic migraineplusfibromyalgiagroup(p=0.042)whencompared withtheothergroups.However,ifweappliedtheBonferroni correction,thisstatisticalsignificancedisappears(Table2).
Nopatientswithfibromyalgiareportedincreasedofmuscle paininallphasesoftheexercise.Allpatientswithmigraine andcontrolshadnonewcomplaintsrelatedtestsduringthe study.
Discussion
Thelactic acid blood level increasedduring exercise, with theskeletalmusclebeingthelargest productionsite.20 The increase inlactic acid production occurs after anincrease
of glycogenolysis and glycolysis. These changes promote
a reversal ofsystemic genesis of energy, increasing circu-lating levels of catecholamines and altering the systemic glucose metabolism.21,22 The energy source in the central
nervous system (CNS) originates from glucose and lactic
acid.Thelatterservesasenergysourceafterovercomingthe
blood–brainbarrierorwhenbeingproduceddirectlyinglial cells.23IntheCNS,lacticacidisessentialformaintainingthe metabolicinteractionsbetweenastrocytesandneurons,and itsincreasesinlacticacidinfluenceneuronalactivityinthe hypothalamusandthesolitarytract.24,25
Thediffusionoflactic acid isknowntobemediatedby transporters,suchasmonocarboxylatetransporters1(MCT1) and 2(MCT2), allowinggreater ATPsynthesis, closure ofK channels and neuronal depolarization.26 The sub-forms of
MCT1 and MCT2 are expressed in the sites of lactic acid
production (muscle and glialcells) and local of utilization (astrocytes,bloodvessels,hippocampus,cerebellum,cerebral cortexandhypothalamus).27Inhumans,theamountof intra-cellular lactate is determined by the balance between the amountproducedinthecellfromincreasedglycolysis (physi-calactivity)andthequantitytransportedoutofthecellorinto themitochondria(influencedbyMCT1).Acutephysical activ-ityalterstheexpressionofMCT1inthefirstminutes,andthis changeismaintainedwithin24hoursafterexercise.28
A central mechanism that may alter lactate removalis
4.0
3.5
3.0
2.5
Rest Aerobic Anaerobic
Lactic acid levels (mmoles/I)
Rest post anaerobic
Fig.1–Lacticacidlevelsandresponsetothetypeof exercisesin113femalecases(controls20;fibromyalgia20; episodicmigraine20;chronicmigraine20;episodic migraineplusfibromyalgia13;andchronicmigraineplus fibromyalgia20).
function, peripheral blood flow and the elevation of
cat-echolamine levels (norepinephrine and epinephrine).29
However,themainremovalcapacityoflactateduring exer-ciseisdetermined bytheactionofcellularMCT1, whichis expressedinlargeamountsinthefirstminutesfollowingthe onsetofphysicalactivity.Thisrelationshipoccurssuchthat theincreasedamountofcirculatingMCT1isdirectlyrelated tothereductionofthelevelsofmusclelacticacid.30,31
Conclusion
In conclusion our groups ofchronic migraine and chronic
migraineplusfibromyalgiashowedsignificantincreased lev-elsoflacticacidduringaerobicphysicalactivityinrelationto thecontrols.However,theydidnotreachastatistical signifi-cancelevelafterBonferronicorrection.Theincreasedlevels
seems to be more dependent on the presence of chronic
migrainethanfibromyalgiaandmaybeduetotheincreased production,bythedecreasedmetabolismoflacticacidorto theseveralmedicationsusedbythepatients.Ourfindings can-notsupportthesuggestionofabnormalmetabolismoflactic acidinpatientswithepisodicandchronicmigraineassociated withfibromyalgia.Nocausalrelationshipbetweenmigraine, fibromyalgiaandlacticacidproductionwasfound.
Funding
ThisworkwassupportedbygrantsfromFundac¸ãoAraucária,
CNPq,CAPES.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.Sanchez-Del-RioM,ReuterU,MoskowitzMA.Newinsights intomigrainepathophysiology.CurrOpinNeurol.
2006;19:294–8.
2.HeadacheClassificationSubcommitteeoftheInternational HeadacheSociety:TheInternationalClassificationof HeadacheDisorders.Cephalalgia.2004;24:9–160.
3.OkadaH,AragaS,TakeshimaT,NakashimaK.Plasmalactic acidandpyruvicacidlevelsinmigraineandtension–type headache.Headache.1998;38:39–42.
4.WatanabeH,KuwabaraT,OhkuboM,TsujiS,YuasaT. Elevationofcerebrallactatedetectedbylocalized 1H-magneticresonancespectroscopymigraineduringthe interictalperiod.Neurology.1996;47:1093–5.
5.ReyngoudtH,PaemeleireK,DierickxA,DescampsB, VandemaeleP,DeDeeneY,etal.Doesvisualcortexlactate increasefollowingphoticstimulationinmigrainewithout aurapatients?Afunctional(1)H-MRSstudy.JHeadachePain. 2011;12:295–302.
6.JeremyMB,TymoczkoJL,StryerL.Glicoseegliconeogênese. In:JeremyMB,TymoczkoJL,StryerL,editors.Bioquímica.Rio deJaneiro:GuanabaraKoogan;2008.p.437–77.
7.MariebE,HoehnK.Músculoetecidomuscular.In:MariebE, HoehnK,editors.Anatomiaefisiologia.PortoAlegre:Artmed; 2009.p.246–83.
8.GibsonH,EdwardsRH.Muscularexerciseandfatigue.Sports Med.1985;2:120–32.
9.HafenG,Laux-EndR,TruttmannAC,SchiblerA,McGuiganJA, PeheimE,etal.Plasmaionizedmagnesiumduringacute hyperventilationhumans.ClinSci(Lond).1996;91: 347–51.
10.RamadanNM,HalvorsonH,Vande-LindeA,LevineSR, HelpernJA,WelchKM.Lowbrainmagnesiuminmigraine. Headache.1989;29:590–3.
11.TeixeiraMJ.Fisiologia.In:TeixeiraMJ,editor.Dor:Conceitos Gerais.SãoPaulo:LimayEditoraLtda;1994.p.8–20.
12.WolfeF,SmytheHA,YunusMB,BennettRM,BombardierC, GoldenbergDL,etal.TheAmericanCollegeofRheumatology 1990.CriteriafortheClassificationofFibromyalgiaReportof theMulticenterCriteriaCommittee.ArthritisRheum. 1990;33:160–72.
13.WolfeF,ClauwDJ,FitzcharlesMA,GoldenbergDL,KaztRS, MeaseP,etal.TheAmericanCollegeofRheumatology. Preliminarydiagnosticcriteriaforfibromyalgiaand measurementofsymptomseverity.ArthritisCareRes. 2010;62:600–10.
14.IferganeG,BuskilaD,SimiseshvelyN,ZeevK,CohenH. Prevalenceoffibromyalgiasyndromeinmigrainepatients. Cephalalgia.2006;26:451–6.
15.GerdleB,SoderbergK,SalvadorPuigvertL,RosendalL, LarssonB.Increasedinterstitialconcentrationsofpyruvate andlactateinthetrapeziusmuscleofpatrientswith fibromyalgia:amicrodialysisstudy.JRehabilMed. 2010;42:679–87.
16.NorregaardJ,BulowPM,MehlsenJ,Danneskiold-SamsøeB. Biochemicalchangesinrelationtoamaximalexercisetestin patientswithfibromyalgia.ClinPhysiol.1994;14:
159–67.
17.MciverKL,EvansC,KrausRM,IspasL,SciottiVM,HicknerRC. NO-mediatedalterationsinskaletalmusclenutritiveblood flowandlactatemetabolisminfibromyalgia.Pain. 2005;120:161–9.
18.MengshoelAM,SaugenE,ForreO,VøllestadNK.Muscle fatigueinearlyfibromyalgia.JRheumatol.1995;22:143–50.
20.KarvonenJ,VuorimaaT.Heartandexerciseintensityduring sportsactivities:practicalapplication.SportsMed.
1988;5:303–12.
21.YamadaH,IwakiY,KitaokaR,FujitaniM,ShibakusaT, FujikawaT,etal.Bloodlactatefunctionsasasignalfor enhancingfattyacidmetabolismduringexerciseviaTGF-Bin thebrain.JNutrSciVitaminol(Tokyo).2012;58:88–95.
22.FattorJA,MillerBF,JacobsKA,BrooksGA.Catecholamine responseisattenuatedduringmoderate-intensityexercisein responsetothelactateclamp.AmJPhysiolEndocrinolMetab. 2005;288:E143–7.
23.LombardiAM,FabrisR,BassettoF,SerraR,LeturqueA, FederspilG,etal.Hyperlactatemiareducesmuscleglucose uptakeandGLUT-4mRNAwhileincreasing(E1alpha)PDH geneexpressioninrat.AmJPhysiol.1999;276:
E922–9.
24.vanHallG,StrømstadM,RasmussenP,JansO,ZaarM,GamC, etal.Bloodlactateisanimportantenergysourceforthe humanbrain.JCerebBloodFlowMetab.2009;29:1121–9.
25.PellerinL,MagisgtrettiPJ.Glutamateuptakeintoastrocytes stimutesaerobicglucolysisutilization.ProcNatlAcadSci USA.1994;22:10625–9.
26.BorgMA,TamborlaneWV,ShulmanGI,SherwinRS.Local Lactateperfusionoftheventromedialhypothalamus suppresseshypoglycemiccounterregulation.Diabetes. 2003;52:663–6.
27.HalestrapAP,PriceNT.Theproton-linkedmonocarboxylate transporter(MCT)family:structure,functionandregulation. BiochemJ.1999;343:281–99.
28.Cortés-CamposC,ElizondoR,LlanosP,UrangaRM,NualartF, GarcíaMA.MCTexpressionandlactateinflux/effluxin tanycytesinvolvedinglia-neuronmetabolicinteraction.PLoS. 2011;6:E16411.
29.ThomasC,BishopDJ,LambertK,MercierJ,BrooksGA.Effects ofacuteandchronicexerciseonsarcolemmalMCT1and MCT4contentsinhumanskeletalmuscles:currentstatus. AmJPhysiolRegulIntegrCompPhysiol.2012;302:R1–14.
30.GrantSM,GreenHJ,PhillipsSM,SuttonJR.Fluidand electrolyteresponsestoexerciseandacuteplasmavolume expansion.JApplPhysiol.1996;81:2386–92.