www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Otologic
and
audiologic
characteristics
of
type
2
diabetics
in
a
tertiary
health
institution
in
Nigeria
夽
Stephen
Oluwatosin
Adebola
a,∗,
Micheal
A.
Olamoyegun
b,
Olusola
A.
Sogebi
c,
Sandra
O.
Iwuala
d,
John
A.
Babarinde
a,
Abayomi
O.
Oyelakin
aaLadokeAkintolaUniversityofTechnology(LAUTECH)TeachingHospital,DepartmentofOtorhinolaryngology,Ogbomoso,Nigeria bLadokeAkintolaUniversityofTechnology,Endocrinology,DiabetesandMetabolismUnit,CollegeofHealthSciences,LAUTECH
TeachingHospital,Ogbomoso,Nigeria
cOlabisiOnabanjoUniversity,CollegeofHealthSciences,ENTUnit,DepartmentofSurgery,Sagamu,Nigeria
dUniversityofLagos,LagosUniversityTeachingHospital,andCollegeofMedicine,DepartmentofMedicine,Endocrinology,
DiabetesandMetabolismUnit,Lagos,Nigeria
Received26August2015;accepted26October2015 Availableonline10February2016
KEYWORDS
Diabetesmellitus; Eardisease;
Hearingimpairment; Puretone
audiometry; Nigeria
Abstract
Introduction:Thiscross-sectionalcomparativestudywascarriedoutattheDiabetesoutpatient clinicofLAUTECHTeachingHospital(LTH)Ogbomoso,Nigeria.
Objective: Thisstudyassessedpatternsofotologicdiseasesandauditoryacuityamongtype2 diabeticsanddeterminantsofthesefindingsamongdiabetics.
Methods:Ninety-seven consentingpatients withclinical diagnosis ofdiabetes mellitus (194 ears)werematchedforageandsexwithninetynon-diabeticpatients(180ears).Thesepatients werescreenedusingotoscopyandpuretoneaudiometryovera6-monthperiod.
Results:Thestudyreportedacrudeprevalencerateof21.6%hearinglossinT2DMpatients.The mostcommontypeofotologicdiseasethatshowedsignificantassociationwithT2DMpatients was otitis mediawith effusion(p=0.027).T2DMwas significantly associatedwith abnormal audiometricfindings(p=0.022),particularlysensorineuralhearingloss(p=0.022),ofthe mod-erategrade(p=0.057).Therewerenodifferencesoftheaudilogicalfindingsforanyparticular ear,andnodifferentialaffectationoffrequencyrangewasobserved.Coexistinghypertension andpoorglycaemiccontrolweresignificantlyassociatedwithaggravationofthehearingofthe T2DMpatients(p < 0.001,andp=0.009respectively).
夽 Pleasecitethisarticleas:AdebolaSO,OlamoyegunMA,SogebiOA,IwualaSO,BabarindeJA,OyelakinAO.Otologicand audiologic characteristicsoftype2diabeticsinatertiaryhealthinstitutioninNigeria.BrazJOtorhinolaryngol.2016;82:567---73.
∗Correspondingauthor.
E-mail:[email protected](S.O.Adebola). http://dx.doi.org/10.1016/j.bjorl.2015.10.016
Conclusion:T2DMhadappreciableeffectsonhearingacuity.T2DMwassignificantlyassociated withthetypeandthedegreeofthehearingloss.Theneedforscreeningofhearingacuityof T2DMpatients,inordertodetectearlychanges,andpromptlyofferanadequatemanagement andremedialmeasureswasemphasizedinthisstudy.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http://
creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Diabetesmelito; Doenc¸aotológica; Deficiênciaauditiva; Audiometriatonal; Nigéria
Característicasaudiológicaseotológicasdediabéticostipo2emumainstituic¸ão
desaúdeterciárianaNigéria
Resumo
Introduc¸ão:Esteestudodecaso-controlefoirealizadonoAmbulatóriodeDiabetesdoLAUTECH TeachingHospital(LTH),emOgbomoso,Nigéria.
Objetivo:Esteestudoavaliouospadrõesdedoenc¸asotológicaseacuidadeauditivaentreos diabéticostipo2eosfatoresdeterminantesdessesachadosentreosdiabéticos.
Método: Aotodo,97pacientescomdiagnósticoclínicodediabetesmelito(194orelhas)deram seu consentimento e foram pareados por idade e sexo, com 90 pacientes não diabéticos (180orelhas).Elesforamavaliadosporotoscopiaeaudiometriatonalliminarporumperíodo deseismeses.
Resultados: Oestudorelatouumataxadeprevalênciabrutade21,6%deperdaauditivaem pacientes comDM2. Otipo mais comum de doenc¸a otológica, afetando significativamente pacientescomDM2,foiotitemédiacomefusão(p=0,027).ADM2foiassociadacomachados audiométricosalterados(p=0,022),principalmenteperdaauditivaneurossensorial(p=0,012), degraumoderado(p=0,057).Nãohouvepredilec¸ãodosefeitosdaDM2paraumadasorelhas emparticular,etambémnãohouveefeitodiferencialdafaixadefrequência.Acoexistênciade hipertensãoecontroleglicêmicoinadequadoassociou-sesignificativamenteàpioradaaudic¸ão dospacientescomDM2(p<0,001ep=0,009,respectivamente).
Conclusão:ADM2mostrouapresentarefeitossignificantesnaacuidadeauditivaafetando sig-nificativamenteotipoeograudadisacusia.Esteestudomostrouanecessidadedeavaliac¸ão daacuidadeauditivadepacientescomDM2,afimdedetectarasalterac¸õesiniciais,epoder rapidamenteoferecermedidascorretivasadequadas.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http://
creativecommons.org/licenses/by/4.0/).
Introduction
Diabetesmellitusisachronicmetabolicdisorder character-izedbyhyperglycemiaduetoinadequateinsulinsecretion, ineffectiveaction or a combination of these. Worldwide, theprevalenceof diabetesis increasingalthoughtherate variesfromcountries,racesandreligion.Ithasbeen esti-mated thatthe prevalence of diabeteswill increase from present382millionto592millionby2035.1Thevast
major-ity of diabetes cases fall into 2 major etiopathogenetic categories, Type 1 diabetes which occurs as a result of absolute deficiency of insulin secretion and Type 2 dia-beteswhichiscausedbyacombinationofinsulinresistance and a faulty compensatory insulin secretory response.2
Other categories include; Other specific types (caused by specific genetic defects, surgery, drugs); Gestational Dia-betesMellitus(GDM);ImpairedGlucoseTolerance(IGT)and Impaired FastingGlucose (IFG).2 Type 2 diabetes mellitus
(T2DM)accountsfor80%---90%ofallcasesofdiabetesandis closelyrelatedtoobesityamongother riskfactors.It isa
multisystem disorder with a propensity to affect the cardiovascular system, and produces varying chronic microvascular and macrovascular complications. Amongst the complications, hearing loss remains one of its most-distressing and least understood phenomenon. Thus researchers have proposed various hypotheses includ-ing micro-angiopathy and neuropathy to explain the complication.3---5 Infact, studies have demonstrated that
the micro-angiopathy in Type 2 Diabetes Mellitus (T2DM) involvesmostlythecochlear withassociateddegeneration ofthestriavascularisandcochlearouterhaircells.6,7
Thepatternofhearinglossindiabeteshasbeenshown in many studies8---14 to be moderately severe in
magni-tude, progressive in nature, and bilateral in occurrence and may be irreversible. The prevalence of hearing loss in diabetics in Nigerian population has not been studied extensively.9,15 This study wasundertaken todescribethe
importantbecausetype2diabetesmellitusisapublichealth problem,whichsignificantlyandnegativelyaffectthe qual-ityoflifewhencomplicatedwithhearingloss.15
Methods
Studydesign
Thiscross-sectionalandcomparativestudywascarriedout onpatients attendingthe Endocrinologyand General out-patientclinicsinLadokeAkintola UniversityofTechnology Teaching Hospital (LTH) Ogbomoso, Nigeria. One hundred and87patientsweredividedintotwogroupsbasedontheir diabetesstatus;GroupIconsistedof97patientsdiagnosed with type 2 diabetes (T2DM), attending the endocrinol-ogyclinic andthe grouptwoconsisted of90 non-diabetic patientsattendingthegeneraloutpatientclinic,whichwere matchedforageandsexwiththestudygroup.Thestudywas carriedoutover a6month periodfromDecember2013to May2014.
ThestudywasapprovedbytheinstitutionalEthics com-mittee of the Ladoke Akintola University of Technology Teaching Hospital (LTH) Ogbomoso, Nigeria. Appropriate samplesizewasdeterminedaccordingtothemethodology ofotherpublishedandrelevantstudies.14
Samplingtechnique:Consecutiveadultpatients attend-ing each of these clinics were approached as potential subjects.Thepurpose,nature,significanceofthestudywas explained to each of the subjects; those that consented wererecruitedassubjects.The maininclusioncriteriafor grouponewere:knowndiabeticpatientswhohadattended at least 2 visits at outpatientdiabetic clinics, aged≥ 30 years witha confirmed diagnosis of T2DM based onWHO criteria of Fasting Plasma Glucose (FPG) of ≥ 126mg/dL (7mmoL/L),regardedasthetestsubjects.Forthepatients ofthegrouptwo,normalbloodglucoselevel(takenasFPG <110mg/dL(6.1mmoL/L)servedascontrols.Adiagnosisof hypertensionwasmadeinpatientswithsystolicblood pres-sure>140mmHganddiastolicbloodpressure>90mmHg.
Patients withhistory of consumption of ototoxicdrugs within three months, previous history of ear surgeries, recent infectionsin theear, noseand throat, history sug-gestive of exposure to noise induced hearing loss were excluded. Data were generated from the information extracted from the participant by the researchers using aninterviewer-administeredquestionnaire.Theinformation obtained included socio-demographic parameters like the agelastbirthday,sex,socialclasses16andoccupationofeach
participant.
The weight measured inkilograms (kg) of the subjects weretakenbyusingOmronHN-283digitalbodyweightscale, and the height measurements in metres (m) were taken bySecaLeicesterstandiometer.TheBodyMassIndex(BMI) was calculated as weight in kg/(height in metres)2. The
rangesoftheBMIwere;underweight(<18.0),normalweight (18.1---24.9),overweight(25.0---29.9),Obese(>30.0),Types 1to3(30.0---34.5,35.0---39.9and>40respectively).
Plasma glucose levelswere measured for each partici-pant, afterwithdrawing 2 mlsof venous blood fromeach individual after an overnight fast of at least eighthours. Thevaluesobtainedwasusinginclassifyingthepatientsinto
eitherofthegroups.Theotherlaboratorydatadetermined indiabeticpatientswasglycatedhaemoglobin(HbA1c)using Pointof Caremachine (In 2 ItR).HbA1c < 7% was
consid-eredasgoodglycaemiccontroland>7%aspoorglycaemic
control.
Otoscopicandaudiologicscreening
Otoscopic examination wasperformed on both ears by a Consultant Otolaryngologist using a pneumatic otoscope. Thefindings ofthe outer ear,externalauditory canaland thestatusofthetympanicmembranewererecorded.Only one major diagnosis made from each ear was recorded. Pneumaticotoscopywascarriedouttotestmobilityofthe tympanicmembraneusingtheWelchAllyn3.5vpneumatic otoscope(Model20200).
Diagnostic pure tone audiometry was performed in a sound-proofboothwithambientnoiseof<45dBusinga cali-brated2channelaudiometer(MA53,MaicoInc.)bythesame audiologist on all the subjects. Air conduction thresholds measuredatfrequencies250,500,1000,2000,4000,6000, 8000Hertz,whiletheboneconductionthresholdswere mea-suredatthefrequencies250,500,1000,2000,4000Hzfor each ear separately. The method usedwas based on the AmericanSpeechHearingAssociation(ASHA)guidelinesfor manualpuretoneaudiometry.15
Statisticalanalysis
All statistical analysis were done using SPSS statistical packagefor Windows,version18 (SPSS Inc.,Chicago, IL). The results were presented in simple charts and tables asappropriate descriptiveanalyses.Comparative analyses of the different variables were performed between the T2DMpatientsandcontrols.Differencesbetween categori-calvariableswereexploredusingtheChi-squaretest,while thosebetweencontinuousvariableswereexploredusing stu-dentt-test.Factorsassociatedwithhearingimpairmentin thediabetics were alsoexplored. All analyses were done withstatisticalsignificantlevelsetatp < 0.05.
Results
Therewereonehundredandeightysevenpatients compris-ingof97test-subjectswithtype2diabetes(T2DM)and90 controlsubjectswithoutdiabetes whoparticipatedinthis study.ThegenderdistributionamongT2DM(44malesand53 females)andthecontrols (40malesand50females)were similar(p=0.899).Thelowsocioeconomicclass(groupsIV andV) constituted 62.9% and 52.1% for the test subjects and controls respectively, with no statistically significant difference (p=0.693). The body-mass index (BMI) of the participants showed that 80.4% of diabetics had BMI ≥
Table1 Socio-demographicandclinicalcharacteristicsoftheparticipants. Diabetics Controls
Parameter n=97(%) n=90(%) 2 p-value
Genderofparticipants
Male 44(45.4) 40(44.4)
Female 53(54.6) 50(55.9) 0.016 0.889
Agerange(years)
30---39 10(10.3) 10(11.1)
40---49 18(18.6) 16(17.8)
50---59 11(11.3) 12(13.3)
60---69 35(36.1) 30(33.3)
70---79 12(12.1) 12(13.3)
≥80 11(11.3) 10(11.1)
Mean±SD 58.9±14.95 58.8±14.71 0.997
Socio-economicclass
I 8(8.2) 9(10.0)
II 11(11.3) 14(15.6)
III 17(17.6) 20(22.2)
IV 28(28.9) 21(23.3)
V 33(34.0) 26(28.9) 2.234 0.693
BodyMassIndex(BMI)
Healthyweight 19(19.6) 39(43.3)
Overweight 27(27.8) 31(34.4)
Obesitytype1 15(15.5) 11(12.3)
Obesitytype2 36(37.1) 9(10.0) 23.759 <0.001a
Otoscopicfindings n=194(%) n=180(%)
Normal 99(51.0) 116(64.4) 1.344 0.246
ImpactedCerumenauris 27(13.9) 25(13.9) 0.077 0.781
OtitisMediawithEffusion 38(19.6) 21(11.7) 4.898 0.027a
PerforatedTympanicmembrane 30(15.5) 18(10.0) 3.000 0.083
aStatisticallysignificant.
while diagnosis < 1 year period wasthe most prevalent, 27.8%,thedetailsofthedistributionisinFig.1.
Abnormal pure tone audiometry (PTA) findings were presentin21.5%(21)and8.9%(8)oftheT2DMandcontrols respectively,which wasstatisticallysignificant(p=0.016). The affectation of the ears of participants with abnor-mal PTA findings wasunilateral in fiveof thetwenty-one T2DM patients (5/21, 23.8%) and six of the ten controls (6/10,75.0%). The numberof participants with abnormal
27 30
Duration of diabetes (Years)
25
20
15
10
5
Frequency (Numbers)
0
< 1 1 to 5 6 to 10 11 to 15 16 to 20 > 20 13
15
17
21
4
Figure1 Showingtheduratiomofdiabetes mellitusin sub-jects.
PTA,withbilateralearinvolvementfoundinT2DMpatients wassignificantlyhigherthanincontrols(p=< 0.001).The mostprevalenttypeofhearinglossrecordedamongT2DM patients(in61.9%)wassensorineuralhearinglosswhichwas significantly different(p=0.012) fromthe 37.5% recorded amongthecontrols. Thedegreeofhearinglossmost com-monamongstT2DMpatientsandcontrolsinthestudywas moderatehearingloss,38.0%(8/21)andmildhearingloss, 37.5%(3/8)respectively,whichwerenotstatistically signif-icant(Table2).
Thereweresomedifferences notedbetweentheT2DM groupandthecontrolgroupinthetwopuretoneaverage (PTAv)groupscomputed:PTAv-1(0.5,1,2kHz)andPTAv-2 (4, 6, 8kHz). Diabetics needed more sound intensity for the detectionofPTA thresholdascomparedwithcontrols (Fig.2).Theaveragethresholddifferencesrangedfrom8.5 to12.2decibels(dB)intherightear,andfrom6.4to9.4dB intheleftear.Thesedifferenceswerenotstatistically sig-nificant.
Table2 Audiologiccharacteristicsoftheparticipants.
Diabeticpatients Controls
Parameter n=97(%) n=90(%) 2 p-value
AbnormalPTAfindings
No 76(78.4) 82(91.1)
Yes 21(21.5) 8(8.9) 5.828 0.016*
Levelofinvolvement
Unilateral 5(23.8) 6(75.0) 0.091 0.763
Bilateral 16(76.2) 2(25.0) 10.889 <0.001*
Typeofhearingloss
ConductiveHL 3(14.2) 2(25.0) 0.250 0.650
Sensori-neuralHL 13(61.9) 3(37.5) 6.250 0.012a
MixedHL 5(23.9) 3(37.5) 0.500 0.480
Degreeofthehearingloss
Mild(26---40db) 4(19.0) 3(37.5) 0.143 0.705
Moderate(41---60db) 8(38.0) 2(25.0) 3.600 0.057
Severe(61---80db) 5(24.0) 2(25.0) 1.286 0.257
Profound(>80db) 4(19.0) 1(12.5) 1.800 0.180
PTA,PureToneAudiometry;HL,HearingLoss.
a Statisticallysignificant.
70
60
F
requency (Numbers)
50
40
30
20
10
0
37.6
PTA 1, Right ear PTA 1, Left ear
Type 2 diabetics Controls
PTA 2, Right ear PTA 2, Left ear 25.4
34.5
25.1
61.7
53.2 52.9
59.3
Figure2 Puretoneaudiometricaveragesatdiferentefrequencyrangesaccordingtosubjectcategory.
(p < 0.001).Comparing theaudiogramsbetweenpatients withgoodandpoorglycaemiccontrol,revealedsignificant differencesinbetweenthetwogroupsofpatients(p=0.009) inTable3.
Discussion
Thestudyfoundthatthemainotologicaldiseaseassociated withT2DMpatientsinourenvironmentwasotitismediawith
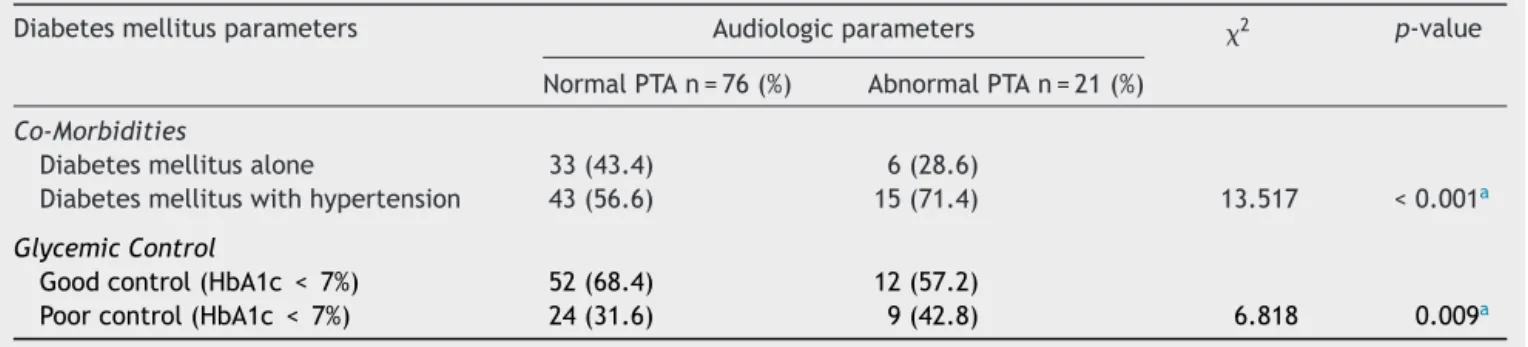
Table3 Showingtherelationshipbetweendiabeticparametersandhearingimpairmentofparticipants.
Diabetesmellitusparameters Audiologicparameters 2 p-value
NormalPTAn=76(%) AbnormalPTAn=21(%)
Co-Morbidities
Diabetesmellitusalone 33(43.4) 6(28.6)
Diabetesmellituswithhypertension 43(56.6) 15(71.4) 13.517 <0.001a
GlycemicControl
Goodcontrol(HbA1c <7%) 52(68.4) 12(57.2)
Poorcontrol(HbA1c < 7%) 24(31.6) 9(42.8) 6.818 0.009a
effusion. There were significant impacts of T2DM on the audiological characteristics namely abnormal audiometric shapes,sensorineuraltypeofhearingloss,involvingthetwo ears.T2DMdidnotdifferentiallyaffectanyfrequencyrange andhad noeffecton thedegree of hearingloss. Hearing impairmentinT2DMpatientswereaggravatedbyco-existing hypertensionandpoorglycaemiccontrol.
Whilethesocio-demographiccharacteristicsof thetwo categoriesof patients were generallysimilar,significantly moreof the diabeticpatients were obeseor at leasthad unhealthyweightssimilartoprevious studies.4,17 The
pre-ponderance of the low socio-economic class, 62.9% and 52.1%inbothT2DMpatientsandcontrolsinthestudy sug-gestthepeculiaritiesofthisclassofindividuals.Thelevel ofeducationinthisclasstendtobelowascomparedwith thehigher classes and addedto thisfact is the tendency totakediets that maynotbebalanced nutritionally, pre-disposingtoobesity. Obesity hadbeen established asone oftheriskfactorsforT2DM,18 andmaintenanceofhealthy
weighthasbeenmentionedamongthewaysforpreventing developmentof T2DM.17,19 Furthermore,weightreduction
remainsoneofthekeylifestylemodificationstrategiesthat hasbeendeployedinthemanagementofT2DM.20,21
While the spectrum of otologic diseases found in this studywasvaried,itwasonlyotitismediawitheffusion(OME) that was found to be significantly associated with T2DM. Thisfindingiscorroboratedbypreviousstudiesin develop-ingcountries,22whereimmune-compromisedstatehasbeen
implicatedasapredisposingfactortodevelopingchronicear diseaseespeciallywithanaerobicbacteriologyinmiddleear isolates.Nasalmucociliaryactiontendstobedecreasedin diabetics, whichmight predispose to OME.23 The study of
Lee, Sun Kyu24 which examined the relationship between
paediatric obesity and OME,noted that obesity results in altered cytokine expression, gastroesophageal reflux dis-easeandfataccumulation,whichmayeventuallyresultin OME.Theremaybeneedforfurtherresearchonthe rela-tionship between T2DM and OME, to explore and fill the obviousgapinknowledgeconcerningthesephenomena.
Twootologicaldiseases,namelyotomycosisand necrotiz-ing(malignant)otitisexterna (NOE)have been reportedly associated with diabetes were not found in this study. Otomycosis is a fungal infection which thrives in the ear whenthesystemicimmunityisgenerallycompromised espe-ciallyin poor glycaemic control.The common practiceof manyof ourpatients instillingoff-the-shelfanti-microbial andantifungal ear dropsinto the earcanals which might inadvertedlytreatotomycosis,andmayberesponsiblefor itsabsencein this population. It is also possible thatour patients’diabeticcontrolwasnotbad,especiallywhenthe simplemajority(27.8%)amongthemwerediagnosedwithin oneyearofnoticingthesymptoms.Thismayalsobe respon-sible for the absenceof NOE in this study. However,it is possiblethatsomeofthesepathologiesweremissedor mis-diagnosedasthespecialtestsrequiredfortheirdiagnoses likenewer moleculardetection methodsavailable as pre-packaged kits (yeast star, auxocoloretic),25 immunoassay
withmonoclonalantibodies,andpolymerasechainreaction (PCR)werenotcarriedoutinthestudy.
Significantly more of the T2DM patients in this study were found to have abnormal audiologic characteristics, particularlyofthesensorineuraltypethataffectedthetwo
ears.Thesystemicnatureofthediseasewilltendtoaffect the two ears, and there might not be a lateralization to aparticularear.Thisisintandemwithfindingsfromother researchers.26Inpatientswithdiabetes,twopossible
mech-anisms had been muted which includes microangiopathic changesinvolvingallthemajorbloodvesselsincludingthat ofthe innerearinT2DMpatients7,11 Secondlytherecould
be primary neuropathy of the cochlear nerve leading to retro-cochlearhearingloss.12Thehearingimpairmentinthis
study significantly affected both ears. Ciorba et al.8 in a
largecohortstudythatevaluatedinnerearchanges result-ingfrommicro-vasculardiseaseinT2DMpatients,however reportedthat the association ofSNHL withT2DMwasnot conclusive.
Someprevious studieshavenotidentifiedany relation-ship between duration of diabetes, presence and degree of hearing loss.12---14 Similarlyin this study,we found that
T2DMdidnotdifferentiallyaffectanyfrequencyrangeand hadnoeffectonthedegree ofhearingloss.Systemic dis-easeslikepresbycusis,andnoiseinducedhearinglosshave been reported todifferentially affect the high frequency tones,27 while Frisina etal.,in a study inUSA, found the
greatest hearing deficits at the lower frequencies among patients with T2DM.28 Mozaffari et al.29 in the study
car-ried outin Iran amongst the non-elderlypopulation (< 60 yearsold),however notedthatage at onsetandduration ofdiabetesmellituswerepredisposingfactorstoacquiring hearinglossindiabetics.ItisobviousinthisstudythatT2DM significantlyaffectedhearingofthesubjects.Thuscertain actionsmaybenecessaryespeciallyashearingimpairment itself can constitute a majormorbidity. The management ofT2DMwillrequireamultidisciplinaryapproachinvolving the diabetologist, the dietitian, the otologist, audiologist andpossiblytheneurologist.Weproposethatscreeningof hearing acuities withdiagnostic pure tone audiometry be performed at diagnosis of T2DM,and at least six-monthly intervalsonthe initialresultsof thetests.This willallow early detectionofauditory anomalies,permit promptand adequatemanagementtobeofferedandremedialmeasures institutedasappropriate.
HearingimpairmentinT2DMpatientsareaggravatedby co-existing hypertension andpoor glycaemic control.This is in keeping with findings of Duck et al.,30 whose study
supported the hypothesis that the presence of end-organ damage in diabetics, tends to be exacerbated in the co-existinghypertension.Howevertheimpactofhypertension in T2DM patients in this study must be made cautiously, as other known and reported confounders like hypercho-lesterolemia, heavy smoking, and geneticpredisposition18
werenotcontrolledfor.Furthermore,asreportedinsome other studies9,12,31 we found that hearing impairment in
T2DMpatientswerealsoaggravatedbypoorglycaemic con-trol. Prolonged accumulation of products of glycation in the inner ear, especially the outer hair cell function has been attributed tobe responsible for the hearing impair-mentassociatedwithpoorglycaemiccontrol amongT2DM patients.However,thisexplanationisnotdefinitive, espe-cially as some other studies had not found a significant association between these two phenomena,32 The exact
Thestudywaslimitedbyitshospital-basednature,and thefactthatotherconfoundersandco-morbiditieswerenot subjectedtocontrol.Alargerpopulation-based epidemio-logical study might benecessary for betterelucidation of thisimportantsubject.
Conclusion
Inconclusion,thisstudyfound thatT2DMhadappreciable effectsonhearingacuity,showingasignificantassociation between the disease andthe type andthe degree of the hearingloss.Thereisaneedforscreeningofhearingacuity ofT2DMpatients,inordertodetectthechangesearly, offer-ingapromptadequatemanagementandremedialmeasures asappropriate.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.InternationalDiabetesFederationIDFDiabetesAtlas,6th edi-tion. 2013. DK Publishing, Brussels, Belgium: International DiabetesFederation.
2.AmericanDiabetesAssociation(ADA)P.Diagnosisand classifica-tionofdiabetesmellitus.diabetescare.2004;27:S5-S10. 3.Toth F, Varkonyi TT, Rovo L, Lengye C, Legrady P, Jori J,
etal.Investigationofauditorybrainstemfunctionindiabetic patients.IntTinnitusJ.2003;9:84---6.
4.HelznerEP,PatelAS,PrattS,Sutton-TyrellK,CauleyJA, Tal-bottE,etal.Hearingsensitivityinolderadults:associations withcardiovascularriskfactorsinthehealth,aging,andbody compositionstudy.JAmGeriatrSoc.2011;59:972---9.
5.LinJ, OghalaibJS. Towards anetiologic diagnosis:assessing thepatientwithhearingloss.AdvOtorhinolaryngol.2011;70: 28---36.
6.Zahnert T. The differential diagnosis of hearing loss. Dtsch ArzteblInt.2011;108:433---44.
7.FukushimaH,CureogluS,SchachernPA,PaparellaMM,Harada T,Oktay MF.Effects oftype2 diabetesmellituson cochlear structure in humans. Arch Otolaryngol Head Neck Surg. 2006;132:934---8.
8.CiorbaA, AimoniC,Bovo R. Hearing lossand diabetes mel-litus: evidences of cochlear microangiopathy. Audiol Med. 2012;10:105---8.
9.Lasisi OA, Nwaorgu OG, Bella AF. Cochleovestibular complications of diabetes mellitus in Ibadan, Nigeria. Int CongrSeries.2003;1240:1325---8.
10.TaylorIG,IrwinJ.Someaudiologicalaspectsofdiabetes melli-tus.JLaryngolOtol.1978;92:99---113.
11.KakarlapudiV,SawyerR,StaeckerH.Theeffectofdiabeteson sensorineuralhearingloss.OtolNeurotol.2003;24:382---6.
12.KurienM,ThomasK,BhanuTS.Hearingthresholdsinpatients withdiabetesmellitus.JLaryngolOtol.1989;103:164---8. 13.DaltonSD,CruickshanksKJ,KleinR,KleinBE,WileyTL.
Associa-tionofNIDDMandhearingloss.DiabetesCare.1998;21:1540---4. 14.SalvenelliF,MieleA,CasaleM,GrecoF,D’AscanioL,FirrisiL, etal.Hearingthresholdsinpatientswithdiabetes.IntJ Otorhi-nolaryngol.2004:3.
15.OlogeFE,OkoroEO.Type2diabetesandhearinglossinblack Africans.DiabetMed.2005;22:664---5.
16.OyedejiGA.Socio-economicandculturalbackgroundof hospi-talizedchildreninIlesha.NigJPaediatrics.1985;12:111---7. 17.MokdadAH,FordES,BowmanBA,DietzWH, VinicorF,Bales
VS,etal.Prevalenceofobesity,diabetesandobesity-related healthriskfactors,2001.JAMA.2003;289:76---9.
18.WildSH,ByrneCD.Riskfactorsfordiabetesandcoronaryheart disease.BMJ.2006;333:1009---11.
19.ChanJM,RimmEB,ColditzGA,StampferMJ,WillettWC. Obe-sity,fatdistributionandweightgainasriskfactorsforclinical diabetesinMen.DiabetesCare.1994;17:961---9.
20.GoldsteinDJ.Beneficialhealtheffectsofmodestweightloss. IntJObesRelatMetabDisord.1992;16:397---415.
21.VidalJ.Updatedreviewonthebenefitsofweightloss.IntJ ObesRelatMetabDisord.2002;26Suppl4:S25---8.
22.AdebolaSO,OlogeFE,AlabiBS,NwabuisiC,FowotadeA.Profile ofanaerobicbacteriologyofmiddleearaspiratesina develop-ingcountry:does immunocompromiseplaya role.Anaerobe. 2014;26:31---5.
23.YueWL.Nasalmucociliaryclearanceinpatientswithdiabetes mellitus.JLaryngolOtol.1989;103:853---5.
24.Lee SK, Yeo SG. Relationship between pediatric obesity and otitis media with effusion. Curr Allergy Asthma Rep. 2009;9:465---72.
25.ForbesBA,SahmDF,WeissfeldAS.Laboratorymethodsinbasic mycology.In: Baileyand Scottsdiagnostic microbiology.12th editionMosby-Elsevier;2007.p.629---712.Chapter50. 26.AgrawalY,PlatzEA,NiparkoJK.Prevalenceofhearinglossand
differences bydemographiccharacteristicsamong USadults. ArchInternMed.2008;168:1522---30.
27.KirchnerDB,EvensonE,DobieRA,RabinowitzP,CrawfordJ, KopkeR,etal.OccupationalNoise-Inducedhearingloss,ACOEM taskforceonOccupationalhearingloss.JOccupEnvironMed. 2012;54:106---8.
28.Frisina ST, Mapes F,Kim H, Frisina DR, Frisina RD. Charac-terizationofhearinglossinagedtypeIIdiabetics.HearRes. 2006;211:103---13.
29.MozaffariM,TajikA,AriaeiN,Ali-EhyaiiF,BehnamH.Diabetes mellitusandsensorineuralhearinglossamongnon-elderly peo-ple.EastMediterrHealthJ.2010;16:947---52.
30.Duck SW, Prazma J, Bennett PS, Pillsbury HC. Interac-tion between Hypertension and Diabetes mellitus in the pathogenesis of Sensorineural hearing loss. Laryngoscope. 1997;107:1596---605.
31.PanchuP.Auditoryacuityintype2diabetesmellitus.IntJ Dia-betesDevCtries.2008;28:114---20.