w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Analysis
of
conditions
for
the
diagnosis
of
rheumatic
diseases
in
primary
health
care
in
the
city
of
Sorocaba-SP
Adriano
Chiereghin
a,∗,
José
Eduardo
Martinez
b aPontifíciaUniversidadeCatólicadeSãoPaulo,Sorocaba,SP,BrazilbDisciplineofRheumatology,PontifíciaUniversidadeCatólicadeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received25October2013 Accepted28April2014
Availableonline28November2014
Keywords:
Rheumaticdiseases Primaryhealthcare
Continuingmedicaleducation
a
b
s
t
r
a
c
t
Objectives: Thestudyhadasmaingoaltodefinetheprofileoftheattendingprofessional workingattheprimaryhealthcaresectorinthecityofSorocaba,andtoanalyzethe envi-ronmentinwhichthisprofessionalisinserted,tryingtoidentifyifthereareconditionsfor thecareoflow-complexityrheumaticdiseasesandpossiblereasonsthatwouldleadtoa highdegreeofreferraltospecialists.
Methods:Aquantitativestudywasperformedinwhichphysiciansofprimaryhealthcare wereinvitedtoansweraquestionnairethataddressedpersonalaspects,besidesthe techni-calaspectsoffourrheumaticdiseases:osteoarthritis,gout,fibromyalgiaandosteoporosis, whichservedasthebasisforevaluatingthecareforlow-complexitydiseasesinUBSs.
Results:Itwasobservedthattheprofessionalispartintegralofanorganizationalsystem thathindershis/herperformance;moreover,certainpersonaldifficultytechniqueswere realized.Together,theseconditionsturnedouttobethefactorsthatdetermineaqualityof carethatfallsshortofthatexpected.
Conclusion: Theremustbeareviewofhowmedicaleducationisoffered,inordertoseek amorequalifiedtraining,focusedonthebasicneedsofthehealthsystem,aswellasa restructuringoftheentirehealthsystemintermsofitsorganizationandmanagement,in ordertoattainasuitableconditionforthedevelopmentofagoodmedicalpractice,and thus,forprovidingagoodservicetothecommunity.
©2014ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](A.Chiereghin).
http://dx.doi.org/10.1016/j.rbre.2014.04.008
Análise
das
condic¸ões
para
diagnóstico
de
doenc¸as
reumáticas
na
atenc¸ão
básica
de
saúde
na
cidade
de
Sorocaba-SP
Palavras-chave:
Doenc¸asreumáticas Atenc¸ãoprimáriadesaúde Educac¸ãomédicacontinuada
r
e
s
u
m
o
Objetivos: Definiroperfildoprofissionalqueatendenosetorprimáriodesaúdenacidade deSorocaba,analisaromeioemqueestáinseridoetentaridentificarsehácondic¸õespara oatendimentodedoenc¸asreumáticasdebaixacomplexidadeeospossíveismotivosque levariamaumaltograudeencaminhamentoaosespecialistas.
Métodos: Fizemosumestudoquantitativonoqualmédicosdaatenc¸ãobásicadesaúde foramconvidadosaresponderumquestionárioqueabordavaaspectospessoaisdo profis-sional,alémdetécnicosdequatrodoenc¸asreumáticas:osteoartrite,gota,fibromialgiae osteoporose, asquaisserviramdebaseparaavaliaroatendimentoa doenc¸asdebaixa complexidadenasunidadesbásicasdesaúde(UBS).
Resultados: Observou-se queoprofissionalencontra-seinseridonumsistema organiza-cionalquedificultasuaatuac¸ão;alémdisso,perceberam-secertasdificuldadespessoais técnicas.Essascondic¸õessomadasacabamporserfatoresquedeterminamumaqualidade deatendimentoaquémdaesperada.
Conclusão: Énecessárioquehajaumarevisãodecomoaeducac¸ãomédicasedá,afim debuscarumaformac¸ãomaisqualificadaevoltadaparaasnecessidadesbásicasdo sis-temadesaúde,alémdeumareestruturac¸ãodetodosistemadesaúdedopontodevista deorganizac¸ãoegestão,paraquehajaumacondic¸ãoadequadaparaodesenvolvimentode umaboapráticamédicae,consequentemente,umaboaprestac¸ãodeservic¸oàpopulac¸ão. ©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Theprioritizationofhealthcareservicesbasedonthe com-plexityofthecasesandproceduresisaprincipleoftheUnified HealthSystem(SistemaÚnicodeSaúde[SUS])inBrazil,that standsoutamongtherest.1,2
Theresolutioncapacityoftheprimarycaresector, repre-sentedbytheBasicHealthUnits(UnidadesBásicasdeSaúde [UBSs]) involves the use of secondary and tertiary sectors; furthermore, it can determine the presence of overloaded urgencyand emergencyunits.Thus,it isexpectedthatthe solutioninmostcasesbeachievedintheUBSsbyreducing referralsandstimulatingthecounter-referrals.1,2
Amongthemedicalareaswherethishierarchicalscheme seemstobepoor,itcallsattentionthoseareascaringfor mus-culoskeletaldiseases.Afailuretoresolvesuchcasesbythe generalpractitionerattheUBSsgeneratesanexpectationof attendanceatotherlevelsofassistanceforthespecialtiesof Rheumatology,OrthopedicsandPhysiatry.
DatacollectedbytheMunicipalityofSorocabathroughits DepartmentofHealthinAugustandSeptember2011showed anunmetdemandforserviceswithrheumatologists amount-ingto300medicalappointments,whileatthat sametime, anunmetdemandfororthopedistsofaround10,000 appoint-mentswasnoted.
Basedondataandobservationsofcarepracticeprovided, itwasnotedthatthemostprevalentdiseases,responsiblefor thelargestnumberofconsultationsandreferralsto special-ties,arealsothoseoflesscomplexityandthatandrequireless technicalandstructuralfollow-upresources.
Amongthesediseases,therearefourofthem,whichwill servetoillustratetheideathatthereisanoverloadinlooking forthesespecialties:osteoarthritis(OA),popularlyknownas
arthritis, primary osteoporosis (PO), fibromyalgia (FM) and gout(microcrystallinearthritissecondarytouratecrystals).
A reviewof the international literaturehas shown that there are difficulties in monitoring these diseases by gen-eral practitioners. Studies showthat thereisinconsistency in referrals, as it relates to clinical suspicion and pre-sentation complaint; in addition, it is noted in several descriptionstheoccurrenceoflow-qualityreferralsand mis-takentreatments.3–6
The aim of this study is to determine the main fac-tors that hinder the diagnosis of the most prevalent and low-complexityrheumaticdiseasesbyphysiciansworkingat UBSs, and, thus,leading to low efficiency insolving these cases.
Materials
and
methods
Studysites
UBSsofthemunicipalityofSorocaba.
Inclusioncriteria
1. InternistphysiciansworkinginUBSs.
2. Acceptanceofparticipationbysigningafreeandinformed consentform.
Exclusioncriteria
Researchtools
Thequestionnairewasdividedinto:
A. Socio-demographicandprofessionaltrainingissues. B. Questions to assess the degree of technical knowledge
regarding the four chosen diseases for the study: OA, PO, FM and Gout based on their clinical, radiological and laboratory aspects. These technical questions have beenpreparedbasedonclinicalcriteriaandina consen-susestablishedbythemedicalliterature,and havebeen applied, prior to the distribution to the participants of thisstudy,tosixrheumatologistsholdingaspecialisttitle grantedbytheBrazilianSocietyofRheumatology,inorder tovalidatetheanswerstobeconsideredascorrect.After theparticipantsinthestudycompletedthequestionnaire, theresultswerecomparedbetweentwogroups:physicians withupto15yearsandover15yearsofgraduation. C. Levelofperceptionwithrespecttopersonalabilityfor
tak-ingcareofrheumaticdiseases.
The questionnaires were sent through the Municipal Health Department, after due approval by the local Ethics Committee(CEP-PUC/SP),toallmedicalprofessionals belong-ingtotheprimarycarenetwork,withatotalof136physicians. DataweretabulatedandanalyzedusinganExcelplatform andthenstatisticallyanalyzedusingSPSSsoftwareversion 13.0.
For descriptive analyses, mean, standard deviation, median,minimumandmaximumwereconsidered.Forthe analysisoftheresultsofdiseases’scores,ananalysisof vari-ancewasused;andtocheckwhethertherewasarelationship betweenthetotalpointsobtainedinthesediseasesand train-ingtime,aStudent’sttestwasusedforobtainingthemeans.
Results
Ofthe136questionnairessent,49returnedfullyansweredand withaninformedconsentformsigned,bringingthetotalrate ofadhesionto36.02%.
Asfortheprofessionalprofile,themeanagewas42.5±11.8 years,and24(48.9%)weremaleand25(51.1%)female.
Twenty-twophysicians(44.9%)wereover15yearsof grad-uation. About 75% of all respondents completed or were attending residency or specialization programs, and only 36.7%oftheseprogramswererelatedtotheclinicalareaand theirspecialties.
Itwasalsoobservedthat55.1%oftheprofessionals ded-icated3–6periodsper weekforpublic service(each period shouldbeunderstoodas:morning,afternoonorevening).The workingtimeinpublicservicerangedfrom3monthsto29 years,withamedianof5years,and75%hadupto13yearsof publicservice.
About90%oftherespondentsreportedthattheyfelt rec-ognizedbytheirpatients,regardingthecareprovidedbythem asageneralpractitioner.
Inrelationtotheupdatingprocess,75.5%respondedthat theytookpartin2–6scientificeventsinthelasttwoyears.
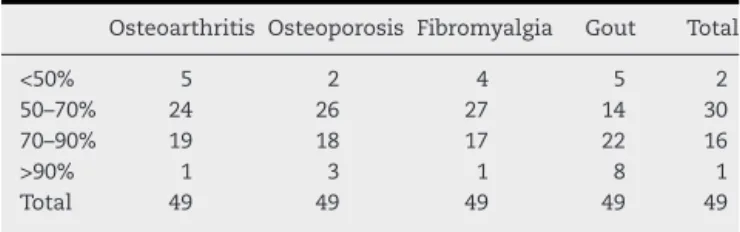
Table1–Stratificationbypercentageofcorrectanswers.
Osteoarthritis Osteoporosis Fibromyalgia Gout Total
<50% 5 2 4 5 2
50–70% 24 26 27 14 30
70–90% 19 18 17 22 16
>90% 1 3 1 8 1
Total 49 49 49 49 49
44.9%oftheseprofessionalssearchedforweeklyupdateson theInternet,and36.7%readprofessionaljournalsmonthly.
Inassessingtheprofileofmedicalcare,89.8%sawbetween 3and5patientsperhour.Accordingto79.6%ofrespondents, thisvolumeofconsultationgeneratedashortervisittimethan whatwouldbenecessaryforanassessmentrelatedto mus-culoskeletalcomplaints.ThepressureforproductivityinUBSs wasreportedasthemainfactorfortheshortconsultationtime (75.5%).
Thereasons forreferral ofthesecasestothe secondary units were:casecomplexity (55.1%)and lackofknowledge aboutthedisease(57.1%).About6.1%oftherespondents jus-tifiedthe referralasaresultoflackofinterest infollowing these cases.Most ofthe respondents reportedthat not all casesshouldbetreatedbyspecialists(87.8%).
Inthesecondpartofthequestionnaire,relatedtospecific technical knowledge,weassigned the correct answers and dividedthemintopercentiles,asshowninTable1.
Ahighernumberofcorrectresponsesbetweenpercentiles 50and70%wasobservedinalldiseases,exceptforgout,which stayedbetween70and90%.
Table2showsthedistributionofcorrectanswers
accord-ingtothetimeofgraduationofprofessionals.Astatistically significant difference was observed onlyin relation to the knowledgeaboutosteoarthritis.
Inthequestionsaboutpersonalperception,itwasasked about thepreparationforcaringrheumaticdiseases(in the opinionoftheinterviewee),andwhichdiseaseswouldpresent greatereaseordifficulty,inadditiontothosestructuralissues imposinglimitationsforthepatient’scare.
Whentheparticipantswereaskedabouttheperceptionof anadequate preparationtoconductsuchcases,only10.2% thoughttheywereunpreparedtofollowthecaseswith mus-culoskeletalcomplaints.
Thediseases mentionedas ofgreater ease ofcarewere gout, osteoarthritis and soft tissuerheumatism. Regarding themostdifficultdiseases,therespondentscitedvasculitis, progressivesystemicsclerosis,systemiclupuserythematosus andSjögren’ssyndrome.
Table2–Percentageofcorrectanswersbydisease, accordingtotimeelapsedsincegraduation.
Upto15years old,n=27
≥16years, n=22
p
Osteoarthritis 66.92 58.11 0.024
Gout 66.29 70.45 0.184
Fibromyalgia 66.64 66.75 0.487
Asforthedifficultiesimposedbytheworkingstructurefor thediagnosisofthesediseases,thefollowingwerementioned:
1. Workingoverload.
2. Lackofaccesstoimagingstudies. 3. Lackofamultidisciplinaryapproach.
Astotheitemregardingtheaccesstoimagingstudies,it hasbeenmentionedthat,forrequestingbonedensitometry (whichisessentialforthediagnosisofPO)thepatienthadtobe referenced.Ontheotherhand,regardingcommonradiological imaging,adelayinobtainingthesestudieswasmentioned.
Discussion
Thedatastemmingfromthisstudyshowthatthephysician whoworksatUBSsisarelativelyyoungprofessional, with-outgenderpredominanceandmostlywithagraduationtime below15years(55.1%).
National guidelines for the teaching ofmedical courses recommendthatthegraduatemustbeabletosolvemostof thecasescoveredintheprimarysector.Thus,thelow spe-cializationinclinicalareasobservedinthisstudyshouldnot influencetheperformanceoftheseprofessionals(34%).7
Itcan be seen that, in mostcases, the medical profes-sional working at UBSs has a personal perception of the importanceofhis/herroleasprimarycareclinician.Thisis evidentbecausethevastmajorityfeltrecognizedbytheuser, regardingtheir medicalpractice(87.9%). Thisperception is important,becausethephysicianmustbecommittedtothe citizenshipandaspromoterofintegralhealthpractice,trying toanalyzeandsolvethesocialproblemsthatarise,7notbeing justatechnicalperformer.
Thephysiciansfeel thattheyare immersedinaprocess ofexcessiveworkload;thiswasarecurringcomplaint.They alsoreportthattheydonothaveenoughtimeforpropercare, regardingthisissueasapriority.
Anothercomplaintfrequentlyreportedbytherespondents referstoadeficiencyinthestructureofhealthcare.Inthis aspect,thedifficultyofaccesstoancillarytestsstandsout. Thissituationinvariablygeneratesadelayintheirdiagnosis andtreatment.Itiscriticaltorediscusswhattestsshouldbe availabletocliniciansintheUBSs.Thisdiscussionshould con-sidertheindicationofeachexamanditspotentialtoexpedite theservice.InthecaseofPO,itisknownthatdensitometry isanessentialstudytoitsdiagnosisandthatthereare guide-linestodetermineitsindication.Thus,anexcess oforders canbeavoidedbythesimplerequirementthattheestablished indicationsbefollowedbytheclinician.Theexclusionofthe practitionerintheprocessofrequestingsuchatestdoesnot seemtobeagoodsolution.
Intheanalysisoftheperceptionofeaseordifficultyinthe consultationforspecificdiseases,thereisafeelingof com-fortonthepartofthephysiciansstudied,whenexamining patientswithOA,gout,FMandPO.Itshouldbeemphasized thattheexistenceofthisperceptionofeaseordifficulty,when the doctor isfaced with a certain disease,not necessarily isapreconditionforagoodorbadclinical conduct.Itonly expressesthepersonalopinionofthedoctor.
Whencomparingtheseviewswiththecountingofcorrect answersinthequestionnairethatassessestechnical knowl-edge,thisperceptionisconfirmed,sincethesediseaseshave generatedarate ofcorrectanswers greater than50%,with anemphasistothecorrectanswerstoquestionsaboutgout (70–90%).Aquestionarises:shouldweconsiderthishitrate asacceptable, whenitcomestogeneralpractitioners?One limitationofthisworkisthatitsimplycannotbebasedona definitionofwhatwouldbeanexpectedhitrate.
Regardingthegraduationtime,itwasnotedthattherewas nobig differenceinthepattern ofresponses;this occurred onlyinosteoarthritis,withbetterrates forthe groupupto 15 years. It may be possible to assign the balance to the experienceandlearningcurveacquiredbyolderphysicians, counteractingthelargesteducational“freshness”ofthoseless experienced.
One question that seems relevant is the fact that all researchthataimstomeasuretheknowledgecollideswith theoppositionofsurveyedsubjects.Thisdifficultyhasbeen describedintheliterature.8
Onecanassumethatonlythosewhoconsiderthemselves bettertrainedfeelcomfortableinparticipatinginthisstudy. Thismayhavegeneratedabiasthatcaninfluencethepattern ofanswersprovidedtosomethingbasedontheopiniononlyof thebestprofessionals,andnotontheopinionoftheabsolute majority.
Theissueofmedicalqualificationisrelevant,andthisis probablyoneofthekeysinthequalityofprovidedcare equa-tion.Morethanthequalification,itisimportanttoanalyzethe skillsrequiredforthisprofessional.Theeducationaltrendin manycountries,suchasUK,CanadaandtheUnitedStates,9 isbasedonthisaspect,becauseitisunderstoodthatthe def-inition ofcompetencesisa prerequisitefortheoccurrence ofacquisitionofknowledgeinamoreconsistentand solid form.10
Kenedy11showedthatthereisagapbetweenknowledge and behavior,i.e.,clinicalpractice,andtherearenumerous individualissuesthatdefinetheattitudeanddecisionsthat professionalsmusttake,whenfacingnewproblems.
Theliteraturedescribingtechniquessuccessfullyusedfor training and skills development isextensive.12,13 Here, the important pointis thateach situation requires an individ-ualized approach, and there isno lack oftools todevelop educationprojects.
Thefocusofchangeshouldfallprimarilyongraduation.In thistimeofprofessionaltrainingliesthecriticalpointofthe mainproblemstobeovercome.Astudyof28institutionsof medicaleducationinBrazilhasshownthatthemaindifficulty indevelopingneweducationalandcurricularconceptsliesin theacceptance,byteachers,ofnewmethodologies.The fac-ultygenerallysteersclearofneweducationaldemands,thus perpetuatingthegapbetweenscholarshipandpractice.14
Therefore, this study demonstrates the need for the promotion of a qualified continuing education for these professionals. This education should focus notonlyin the knowledge,butalsomustdevelopskillsthatencompass indi-vidualabilities.15
visionofhealthcarecanbeobtainedfromanamplifiedway, bringingtherealizationthatthemerecase-by-caseanalysisof theclinicalservicesimplifiesamuchmorecomplexproblem. Thisresearch, althoughdevelopedwithanemphasison specificrheumaticproblems,resultedinrelevantinformation withregardtoorganizationalmattersofthehealthsystem. Basedonthat,aviewofhealthcareinanamplifiedmanner, implyingtheperceptionthatamerecase-by-caseanalysisof theclinicalservicesimplifiesamuchmorecomplexproblem, ismadepossible.
Theimpressionobtainedinthestudyisthatprofessionals arewillingtoperformtheirworkinthemostcompleteand accurateway.However,theyrunintostructuralissuesthat arerelatedtotheorganizationofthehealthsystem.
Arevisioninthewaymedicaltrainingisdevelopedisalso consideredassomethingnecessary.Theeffectivenessof tra-ditionalteachingapproachesprovesincreasinglyinsufficient toeffectchangeortoacquireskills.16,17Intheseareas, educa-tionpoliciesmustwalkalongsidehealthpolicies.Oneshould thinkofthehealthprofessionalaspartofthesystemandits potentialtransformingagentfromthestartofhis/her grad-uation,sohe/sheshouldbetaken earlytobecomefamiliar withclinicalpractice.18Thisprofessionalmustbeformedand trainedsothathe/sheisabletounderstandandquestionthe existingfailures;andthusbeactiveinthedevelopmentand improvementofthehealthsystem.
Theadvancesaregettingfaster,andconstantupdatingis necessary.Butconditionsshouldbecreatedforthisto hap-pen.Newwaysofteachingandnewcurriculaarebeingput intopracticeinordertomeettheseneeds.Thereisstillsome resistancetoacceptneweducationaltrendsandformsof edu-cation,buttheoutlookisgood.
Inadditiontothisinvestmentinthehumanpartofthe pro-cess,it seemsclearthatthemanagerialorganizationofthe publichealthsystemshouldberevised.Thepublicsystemis stilllackingabetterstructureandneedstobeabletooffer ade-quateworkingconditions,sothatallprofessionalscanengage initeffectivelyandconcretely.
Weconcludethat:1–theprofessionalsevaluatedfeel com-fortableinaddressingthemostprevalentandlowcomplexity rheumaticdiseases;2–Theknowledgeofclinicalphysicians workingatUBSsissituatedintheaveragelevelwithrespect tothebasicissuesonthesediseases;3–thereisnodifference ofknowledgeregardingthetimeelapsedsincegraduation;4 –themaindifficultiesforthediagnosisofthesediseasesare theshorttimewiththepatientandlittleaccesstoancillary exams.
Conflict
of
interests
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. SUS:oquevocêprecisasabersobreoSistemaÚnicode
Saúde.Associac¸ãoPaulistadeMedicina.2000;1:20.Legislac¸ão
enormaspertinentesaoSUS.
2.Brasil.MinistériodaSaúde.Regionalizac¸ãodaassistênciaà
saúde:aprofundandoadescentralizac¸ãocomequidadede
acesso.2a
ed.rev.atualBrasília:MinistériodaSaúde;2011
[SérieA,NormaseManuaisTécnicos,116].
3.GlazierRH,DalbyDM,BadleyEM,HawkerGA,BellMJ,
BuchbinderR.Determinantsofphysicianconfidenceinthe
primarycaremanagementofmusculoskeletaldisorders.J
Rheumatol.1996;23:351–6.
4.GranJT,NordvagBY.Referralsfromgeneralpracticetoan
outpatientrheumatologyclinic;diseasespectrumand
analysisofreferralletters.ClinRheumatol.2000;19:
450–4.
5.Games-NavaJI,Gonzalez-LopezL,DavisP,Suarez-Almazor
ME.Referralanddiagnosisofcommonrheumaticdiseasesby
primarycarephysicians.BrJRheumatol.1998;37:
1215–9.
6.StainkeyLA,SeidlLA,JohnsonAJ,TullochGE,PainT.The
challengeoflongwaitinglist:howweimplementedaGP
referralsystemfornon-urgentspecialist’appointmentsatan
Australianpublichospital.HealthServRes.2010;10:
303.
7.Brasil.ConselhoNacionaldeEducac¸ão.Resoluc¸ãoCNE/CNS n◦4,de7denovembrode2001.DiárioOficialdaUnião,
Brasília,2001;1,p.38.
8.LauwMN,HoekstraJBJ,LimthorstGE.Thesuccessofaweekly
medicalquiz.Test-basedmedicaleducation.JMed.
2011;69:205–6.
9.CateOT,ScheeleF.Competence-basedpostgraduatetraining.
Canwebridgethegapbetweentheoryandclinicalpractice.
AcadMed.2007;82:542–7.
10.MylopoulosM,RegehrG,GisburgS.Exploringresident’s
perceptionofexpertiseandexpertdevelopment.AcadMed.
2011;86:546–9.
11.KenedyT,RegehrG,RosenfieldJ,RobertsSW,LingardL.
Exploringthegapbetweenknowledgeandbehavior:a
qualitativestudyofclinicianactionfollowinganeducational
intervention.AcadMed.2004;79:386–93.
12.KowacsPA,TwardowschyCA,PiovesanEJ,WilkinsAL,BellMJ.
Generalpracticephysicianknowledgeaboutheadache
evaluationofthemunicipalcontinualmedicaleducation
program.ArqNeuropsiquiatr.2009;67:595–9.
13.WeinerSJ,JacksonJL,GartenS.Measuringcontinuingmedical
educationoutcomes:apilotstudyofeffectsizeofthreeCME
interventionatanSGIMannualmeeting.JGenInternMed.
2009;24:626–9.
14.PerinGL,AbdallaIG,SilvaRHA,LampertJD,StellaRCR,Costa
NMSC.Desenvolvimentodocenteeformac¸ãodemédicos.Rev
BrasEducMéd.2009;33:70–82.
15.LongDM.Competency-basedresidencytraining:thenext
advanceingraduatemedicaleducation.AcadMed.
2000;75:1178–83.
16.LunaFilhoB.Avaliac¸ãodacompetênciamédica–Reflexão
crítica.RevSocCardiolEstadoSãoPaulo.2005;15:
301–5.
17.KlassD.Aperformace-basedconceptionofcompetenceis
changingtheregulationofphysicians’professionalbehavior.
AcadMed.2007;82:529–35.
18.CamposFE,FerreiraJR,FeuerwerkerL,SenaRR,CamposJJB,
CordeiroH,etal.Caminhosparaaproximaraformac¸ãode
profissionaisdesaúdedasnecessidadesdaatenc¸ãobásica.