w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Health
related
quality
of
life
in
Turkish
polio
survivors:
impact
of
post-polio
on
the
health
related
quality
of
life
in
terms
of
functional
status,
severity
of
pain,
fatigue,
and
social,
and
emotional
functioning
夽
Yesim
Garip
a,∗,
Filiz
Eser
b,
Hatice
Bodur
b,
Bedriye
Baskan
b,
Filiz
Sivas
b,
Ozlem
Yilmaz
baAnkaraBasakMedicalCenter,DepartmentofPhysicalMedicineandRehabilitation,Ankara,Turkey
bAnkaraNumuneTrainingandResearchHospital,DepartmentofPhysicalMedicineandRehabilitation,Ankara,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14February2014 Accepted1December2014 Availableonline10March2015
Keywords:
Postpolio-syndrome(PPS) Qualityoflife
Fatigue Rehabilitation
a
b
s
t
r
a
c
t
Objective:Todeterminetheimpactofpostpolio-syndromeonqualityoflifeinpolio sur-vivors.
Methods:Fortypoliosurvivorswereincludedinthestudy.Twenty-onepatientsfulfilling theHalstead’spostpolio-syndromecriteriaparticipatedinpostpolio-syndromegroup.The remainingnineteenpatientsformednon-postpolio-syndrome group.Controlgroupwas composedoffortyhealthysubjects.QualityoflifewasevaluatedbyNottinghamHealth Profile, depressionbyBeckDepressionScaleandfatiguebyFatigueSymptomInventory. Isometricmusclestrengthwasmeasuredbymanualmuscletesting.
Results:Total manual muscletesting scorewas 26.19±13.24 (median:29) in postpolio-syndrome group and 30.08±8.9 (median: 32) in non-postpolio-syndrome group. Total manualmuscletestingscoresofnon-postpolio-syndromegroupweresignificantlyhigher thanthatofpostpolio-syndromegroup.Patientswithpostpolio-syndromereported signifi-cantlyhigherlevelsoffatigueandreducedqualityoflifeintermsofphysicalmobility,pain andenergywhencomparedwithpatientswithoutpostpolio-syndromeandcontrolgroup. Itwasnotreportedastatisticallysignificantdifferenceinsocialandemotional function-ingandsleepqualitybetweenpostpolio-syndrome,non-postpolio-syndromeandcontrol groups.AlsoitwasnotfoundanystatisticallysignificantdifferenceinBeckDepression Scalescoresamongthegroups.
夽
ThisstudyoriginatedfromtheDepartmentofPhysicalMedicineandRehabilitation,AnkaraNumuneTrainingandResearchHospital, Ankara,Turkey.
∗ Correspondingauthor.
E-mail:[email protected](Y.Garip).
http://dx.doi.org/10.1016/j.rbre.2014.12.006
2255-5021/©2015ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
2
rev bras reumatol.2017;57(1):1–7Conclusions: Postpolio-syndrome hasa negativeimpact on quality of life in terms of functionalstatus,severityofpainandenergy.Theidentification,earlyrecognitionand reha-bilitationofpostpolio-syndromepatientsmayresultinanimprovementintheirqualityof life.
©2015ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Qualidade
de
vida
relacionada
com
a
saúde
em
sobreviventes
turcos
da
pólio:
impacto
pós-pólio
na
saúde
relacionada
com
a
qualidade
de
vida
em
termos
de
estado
funcional,
gravidade
da
dor,
fadiga
e
funcionamento
social
e
emocional
Palavras-chave: Síndromepós-pólio Qualidadedevida Fadiga
Reabilitac¸ão
r
e
s
u
m
o
Objetivo: Determinaroimpactoda síndromepós-pólionaqualidadedevidanos sobre-viventesdapólio.
Métodos:Quarentasobreviventesdapólioforamincluídosnoestudo.Participaramdogrupo desíndromepós-pólio21pacientesqueatenderamaoscritériosdesíndromepós-póliode Halstead.Os19restantesformaramogruponãosíndromepós-pólio.Ogrupocontrolefoi compostopor40indivíduossaudáveis.AqualidadedevidafoiavaliadapeloNottingham HealthProfile,adepressãopelaEscaladeDepressãodeBeckeafadigapeloInventáriode SintomasdeFadiga.Aforc¸amuscularisométricafoimedidaportestemuscularmanual. Resultados: Oescoretotaldotestemuscularmanualfoi26,19±13,24(mediana:29)nogrupo desíndromepós-pólioe30,08±8,9(mediana:32)nogruponãosíndromepós-pólio.Escores totaisdetestemuscularmanualdegruponãosíndromepós-pólioforamsignificativamente maioresdoqueosdogrupodesíndromepós-pólio.Ospacientescomsíndromepós-pólio relataramníveissignificativamentemaioresdefadigaequalidadedevidareduzidaem ter-mosdemobilidadefísica,doreenergiaquandocomparadoscompacientessemsíndrome pós-pólio egrupocontrole. Nãoserelatouumadiferenc¸aestatisticamentesignificativa nofuncionamentosocialeemocionalenaqualidadedosonoentregruposdesíndrome pós-pólio,nãosíndromepós-pólioecontrole.Alémdisso,nãoseencontroudiferenc¸a esta-tisticamentesignificativanosescoresdaEscaladeDepressãodeBeckentreosgrupos. Conclusões:Asíndromepós-póliotemumimpactonegativonaqualidadedevidaemtermos deestadofuncional,gravidadedadoreenergia.Aidentificac¸ão,oreconhecimentoprecoce eareabilitac¸ãodospacientescomsíndromepós-póliopodemresultaremumamelhoriada qualidadedevida.
©2015ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Postpolio-syndrome(PPS)isaneurologicdisorder character-ized bya collection oflatemanifestations occurringmany yearsaftertheinitialpoliomyelitisinfection.Neworincreased muscleweaknessisthehallmark.Theotherclinicalfeatures are fatigue, pain in joints, bones and muscles, cold intol-erance and bulbar symptoms (swallow,speech, respiratory symptoms).Fatiguehasbeendescribedasthemostcommon symptom. PPS symptoms affect the abilityto perform the activitiesofdailyliving,mobility,upperlimbfunction,and respiratorycapacity.PPShasanegativeeffectonqualityof life(QoL).1–3
ThepresentstudyaimedtoinvestigateQoLinpolio sur-vivorsinTurkey,toassesstheimpactofPPSonvariousQoL domainsintermsoffunctionalstatus,severityofpain,social andemotionalfunctioning.
Material
and
methods
The study included a total of 40 polio survivors (21 men, 19 women) who were followed at the outpatient clinic of physicalmedicineandrehabilitationdepartmentofa train-ing and research Hospital whichis amajor referral center under MinistryofHealth,locatedinAnkara,capitalcityof Turkey,betweenDecember2012andSeptember2013.Study wasconductedinaccordancewiththeprinciplessetforthin theHelsinkiDeclaration2008.
67.5% of polio survivors (21 patients) fulfilling the Hal-stead’s PPS criteria4 participated in PPS group, and the
painand/orjointpain,newmuscleweaknessinthemuscles previouslyaffectedorunaffected)afterastableperiodofat least15years;(4)exclusionofothermedicalconditionsthat mayexplainthesesymptoms.4
Isometricmusclestrengthwasmeasuredbymanual mus-cletesting(MMT)accordingtoMedicalResearchCouncil(MRC) Scale.5 Hipflexors,knee extensors,kneeflexors,ankle
dor-salflexorandankleplantarflexorswereevaluatedbilaterally, thentotalscorewasobtained(maximumscore:50).
Controlgroupconsistedof40ageandsexmatchedhealthy subjects(20men,20women)whosetotalMMTscoreswere 50. Inclusion criteria for all subjects were no other disor-dersincludingfibromyalgia,hypertension,diabetesmellitus, hepaticandrenaldiseases,inflammatoryarthritis,other neu-rologicalorpsychiatricdisordersthatmaycausefatigue.
Symptomsincludingmusclepain,fatigue,jointpain,sleep disorders,respiratorydisordersanddysphagiawereanalyzed inPPSandnon-PPSgroups.QoLwasassessedbyNottingham HealthProfile(NHP)6anddepressionbyusingBeckDepression
Scale(BDS).7
FatiguewasevaluatedbyusingTurkishversionofFatigue SymptomInventory(FSI).8FSI,firstpublishedin1998,isa
14-itemself-reportmeasuredesignedtoassessfatigueintensity (fouritems),duration(twoitems),itsinterferencewithquality oflife(7items),andthedailypatternoffatigue.Intensityis measuredonseparate11-pointscales(0=notatallfatigued; 10=extremefatigue)thatassessmost,least,currentfatigue and averagefatigueinthe previous week.Eachofthese is scoredasanindividualitem.Theinterferenceitemsassessthe extenttowhichfatigueinterferedwitharespondent’sgeneral activitylevel,abilitytobatheanddress,workactivity,ability toconcentrate,relationswithothers,enjoymentoflifeand moodduringthepreviousweekusingan11pointratingscale (0=no interferenceand 10=extremeinterference). These 7 itemsareaveragedtoobtainaninterferencescalescore. Dura-tionitems(numberofdaysfatigued,amountoftimefatigued) assessfatiguefrequency.Itismeasuredasthenumberofthe days(from0to7days)inthepastweekthatrespondentsfelt fatiguedandtheamountofeachdayonaveragerespondents felt fatigued (0=noneofthe day, 10=the entireday). Each oftheseisscoredasanindividualitem.Thefinalitemasks respondentstoindicatetheirdailypatternoffatigueandso providesdescriptiveinformationaboutpossiblediurnal vari-ationinthedailyexperienceoffatigue(0=notatallfatigued, 1=worseinthemorning,2=worseintheafternoon,3=worse intheevening,4=noconsistentdailypatternoffatigue).Final
itemprovidesinformationonlyandisnotintendedtobeused asaquantitativescale.9–11 TheitemsincludedintheFSIare
showninAppendix1.
Statisticalanalyses
Data were presentedby descriptiveanalysis withmeans±
standard deviation (SD) and median scores. Because vari-ables were not normally distributed, Kruskal–Wallis and Mann–WhitneyUtestswereperformedtoassessstatistically significant differencesinMMT, BDS,FSIandNHPscoresof thegroups.CategoricalvariableswereevaluatedbyChi-square test.Avalueofp<0.05wasconsideredstatisticallysignificant. AllanalyseswereperformedusingStatisticalPackageforthe SocialSciences–13.0(SPSS-13.0)software.
Results
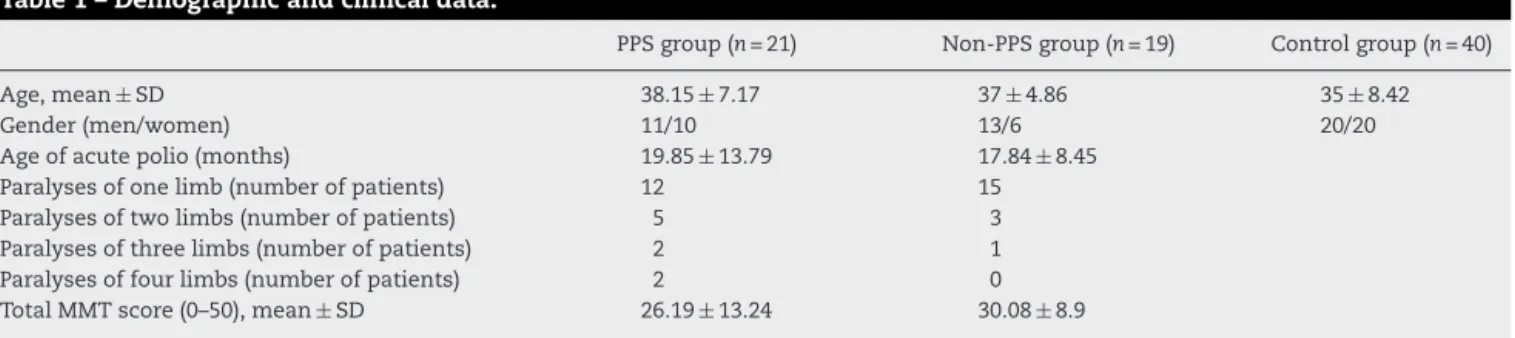
Demographicandclinicalcharacteristicsofthepatientsand controlsubjects are summarizedinTable1.Meanage was 38.15±7.17 in PPS group, 37±4.86 in non-PPS group and 35±8.42inthecontrolgroup.Atthetimeofacutepolio,polio survivorswere19.2±12.23monthsoldonaverage(3months to4years,median:18months).
OfthepatientsinPPSgroup,12hadparalysesofonelimb, 5hadparalysesoftwolimbs,2hadparalysesofthreelimbs, and2hadparalysesoffourlimbs.Oneofthemreportedthat thediseaseaffectedtherespiratorysystem.Ofthepatientsin non-PPSgroup,15hadparalysesofonelimb,3hadparalyses oftwolimbs,and1hadparalysesofthreelimbs.Noneofthem hadparalysesoffourlimbs.Alsononeofthemreportedthat therespiratorysystemwasaffected(Table1).
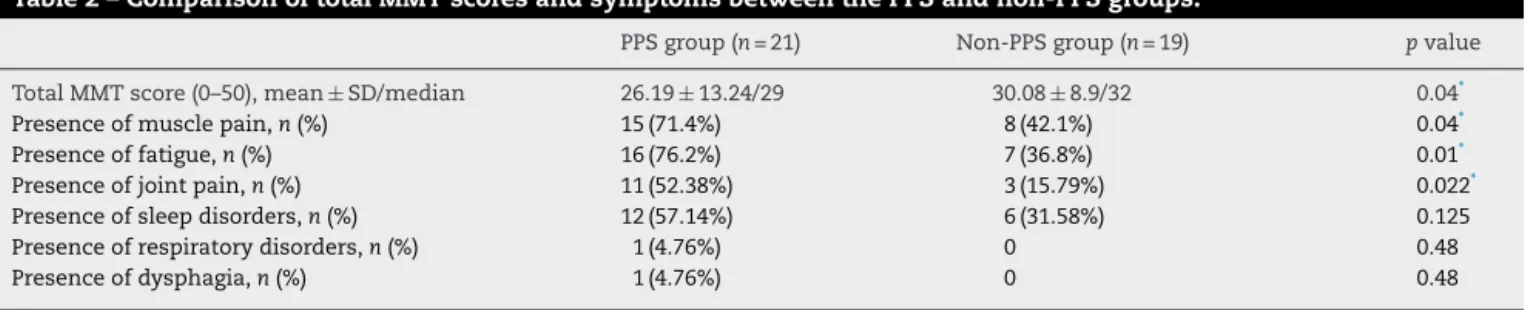
Themostcommonsymptoms werefatigue(16 patients, 76.2%), and muscle pain (15 patients, 71.4%) inPPS group. Thesewerefollowedbysleepdisorders(12patients,57.14%) andjoint pain(11patients, 52.38%),respectively.Dysphagia andrespiratorydisorderswerenotedinonepatient(4.76%). Innon-PPSgroup,the mostfrequentsymptomswere mus-clepain,fatigue,sleepdisordersandjointpain,whichwere reported in 42.1%, 36.8%, 31.58%, 15.79% of the patients, respectively.Fatigue,jointpainandmusclepainwere signif-icantly higherinPPS group(p<0.05).Total MMTscore was 26.19±13.24(median:29)inPPSgroupand30.08±8.9(median: 32)innon-PPSgroup.AccordingtotheMann–WhitneyUtest,
Table1–Demographicandclinicaldata.
PPSgroup(n=21) Non-PPSgroup(n=19) Controlgroup(n=40)
Age,mean±SD 38.15±7.17 37±4.86 35±8.42
Gender(men/women) 11/10 13/6 20/20
Ageofacutepolio(months) 19.85±13.79 17.84±8.45 Paralysesofonelimb(numberofpatients) 12 15 Paralysesoftwolimbs(numberofpatients) 5 3 Paralysesofthreelimbs(numberofpatients) 2 1 Paralysesoffourlimbs(numberofpatients) 2 0 TotalMMTscore(0–50),mean±SD 26.19±13.24 30.08±8.9
4
rev bras reumatol.2017;57(1):1–7Table2–ComparisonoftotalMMTscoresandsymptomsbetweenthePPSandnon-PPSgroups.
PPSgroup(n=21) Non-PPSgroup(n=19) pvalue
TotalMMTscore(0–50),mean±SD/median 26.19±13.24/29 30.08±8.9/32 0.04*
Presenceofmusclepain,n(%) 15(71.4%) 8(42.1%) 0.04*
Presenceoffatigue,n(%) 16(76.2%) 7(36.8%) 0.01*
Presenceofjointpain,n(%) 11(52.38%) 3(15.79%) 0.022*
Presenceofsleepdisorders,n(%) 12(57.14%) 6(31.58%) 0.125
Presenceofrespiratorydisorders,n(%) 1(4.76%) 0 0.48
Presenceofdysphagia,n(%) 1(4.76%) 0 0.48
MMT,manualmuscletesting.
∗ p<0.05(significant).
totalMMTscoresofnon-PPSgroupweresignificantlyhigher thanthatofPPSgroup(p<0.05)(Table2).
Kruskal–Wallistestrevealedthatdifferencesamonggroups weresignificantinallFSIsubgroups(p<0.05).Accordingtothe Mann–WhitneyUtest,FSIscoresofPPSgroupwere signifi-cantlyhigherthanthatofbothnon-PPSgroupandthecontrol group(p<0.05)(Table3).Itwasnotfoundanystatistically sig-nificantdifferenceinBDSscoresbetweenPPS,non-PPSand control groups (p>0.05). Median values of BDS and FSI in patientsandthecontrolgrouparegiveninTable3.
Kruskal–Wallistestshowedthatdifferencesamonggroups were significant in all NHP subgroups except social isola-tion, emotional reaction and sleep (p<0.05). According to the Mann–Whitney U test, PPS group scored significantly higher in pain, physicalmobility and energysubgroups of NHP than non-PPS and the control group (p<0.05). Itwas not reported a statistically significant difference in social isolation,emotionalreactionandsleepsubgroups.Also non-PPSgroup reported poorer levels in all NHPgroups except social isolation, emotional reaction and sleep subgroups, whencomparedtothecontrolgroup(Table4).Median val-uesofNHPscoresinpatientsandthecontrolgrouparegiven
inTable4.
Discussion
TheaimofthisstudywastoinvestigateQoLinpoliosurvivors inTurkeyinordertoassesstheimpactofPPSonQoLinterms offunctional status, severityofpain, social and emotional functioning.
TheresultsshowedthatPPSimpairedQoLincluding physi-calmobility,painandenergy,butdidnotaffectemotionaland socialhealth.Furthermoreitwasnotfoundanystatistically significantdifferenceinBDSscoresbetweenPPS,non-PPSand controlgroups.ThisfindingconfirmedthatPPSdidnothave anegativeimpactonemotionalstatus.Ourresultssupport thepreviousstudiesintheliterature.Itwasreportedlower scoresinphysicalfunctioningin38post-poliopatientsinthe studyofMcNaughtonetal.whereQoLwasmeasuredbyusing ShortForm-36(SF-36).12 Similarly,JacobinvestigatedQoLin
101poliosurvivorsfromtwopost-polioclinicsinIsraeland reportedlowphysicalscoresandnormalmentalscores includ-ingemotionalandsocialfunctioninginpost-poliopatients.13
Tateetal.confirmedthatpoliosurvivorsdidnotdifferfrom thegeneralpopulationinlevelsofdepression.14Bycontrast,
Schanke,15 Conrady16 and Hazendonk17 reported that PPS
patientshadhigherlevelsofdepressivesymptomsas com-paredtocontrolgroups.AlsoOnetal.foundlowerphysical, socialandemotionalscoresinPPSgroupwhereQoLwas eval-uatedbyusingNHP.18
PatientswithPPSexperiencedsignificantlyhigherlevelsof fatiguewhencomparedtonon-PPSandcontrolgroup.This findingsupportsthepreviousstudies.18–20Toourknowledge,
this isthe first study toevaluatefatigueinpolio survivors byusingFSI.Fatigueisacomplexsymptomanditmustbe assessedbyamultidimensionalquestionnairewhich identi-fiesdifferentaspectsoffatigueindetail.FSIdealswithvarious characteristicsoffatigueanditsperceivedinterferencewith quality oflifeinterms ofgeneralwork activities,abilityto concentrate,andenjoymentoflifeandmood.Furthermore,it statesdailypatternsofFatigue.10,11Itwassuggestedasa
use-fulinstrumentinassessmentoffatiguebythereviewers.21In
previousstudies,nosignificantdifferenceswerefoundintotal MMTscoresbetweenPPSandnon-PPSgroups.18,22Contrarily,
inourstudy,totalMMTscoresofPPSgroupweresignificantly lowerthanthatofnon-PPSgroup.
Inthepresentstudy,themostcommonsymptomswere fatigue(76.2%), andmuscle pain(71.4%)inPPSgroup.This resultisinaccordancewithotherclinicalstudies.Inastudy byNolletondisabilityandfunctionalstatusinDutchpatients withPPS,78%ofthepatientsselectedfatigueastheirmajor problem.22 InConde’sstudy,the mostfrequentcomplaints
were fatigue (87.1%), muscle pain (82.4%), and joint pain (72%).23 Wefoundthatprevalenceoffatigue,jointpainand
musclepainwassignificantlyhigherinPPSgroupthan non-PPSgroup.Prevalenceofsleepdisorderswassimilarinboth of the groups. 57% ofPPS patients had sleep disorders. In the study of van Kralingen, prevalence of sleep disorders wasfoundas50%.24Östlundreportedthatpostpoliorelated
fatiguehadanegativeeffectonsleepquality.25Contrarily,in
ourstudy,fatiguedidnotinfluenceNHPsleepscores. Thesmallsamplesizedeemedourmainlimitation.Itis duetotheexclusionofconcomitantmedicalandpsychiatric diseasesthatmaycausefatigue.
r
e
v
b
r
a
s
r
e
u
m
a
t
o
l
.
2
0
1
7;
5
7(1)
:1–7
5
PPSgroup(n=21) Medianvalues
Non-PPSgroup (n=19) Medianvalues
Controlgroup (n=40) Medianvalues
Chi-square (Kruskal–Wallis)
pvalueX (Mann–WhitneyU)
pvalueY (Mann–WhitneyU)
pvalueZ (Mann–WhitneyU)
BeckDepressionScale 16 13 12 5.43 0.125 0.06 0.83
Mostfatigue 9 5 3 53.29* 0.00* 0.00* 0.001*
Leastfatigue 7 2 0 62.58* 0.00* 0.00* 0.00*
Currentfatigue 7 4 2 53.68* 0.00* 0.00* 0.00*
Averagefatigue 7 4 2 53.88* 0.00* 0.00* 0.00*
Interferencescale 7 3 1 52.29* 0.00* 0.00* 0.002*
Numberofdaysfatigued 7 3 2 52.46* 0.00* 0.00* 0.002*
Amountoftimefatigued 8 4 2 57.23* 0.00* 0.00* 0.00*
pvalueX:pvaluebetweenPPSandnon-PPSgroup. pvalueY:pvaluebetweenPPSandcontrolgroup. pvalueZ:pvaluebetweennon-PPSandcontrolgroup.
∗ p<0.05(significant).
Table4–ComparisonofQoLbetweenthegroups.
PPSgroup(n=21) Medianvalues
Non-PPSgroup (n=19) Medianvalues
Controlgroup (n=40) Medianvalues
Chi-square (Kruskal–Wallis)
pvalueX pvalueY pvalueZ
NHPphysicalmobility 87.5 50 0.0 54.04* 0.00* 0.00* 0.00*
NHPpain 85.71 42.86 0.0 61.20* 0.00* 0.00* 0.00*
NHPenergy 100 50 0.0 31.66* 0.00* 0.00* 0.00*
NHPsocialisolation 25 25 25 0.55 0.56 0.72 0.55
NHPemotionalreaction 37.5 25 25 2.38 0.79 0.10 0.43
NHPsleep 20 20 20 3.03 0.27 0.08 0.76
NHP,NottinghamHealthProfile.
pvalueX:pvaluebetweenPPSandnon-PPSgroup. pvalueY:pvaluebetweenPPSandcontrolgroup. pvalueZ:pvaluebetweennon-PPSandcontrolgroup.
6
rev bras reumatol.2017;57(1):1–7Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Appendix
1.
The
Fatigue
Symptom
Inventory
(FSI)
1-Rate your level of fatigue on the day you felt most fatigued during the past week.
0 1 2 3 4 5 6 7 8 9 10 Not at all fatigued Extreme fatigue
2-Rate your level of fatigue on the day you felt least fatigued during the past week.
0 1 2 3 4 5 6 7 8 9 10 Not at all fatigued Extreme fatigue
3- Rate your level of fatigue on the average during the last week.
0 1 2 3 4 5 6 7 8 9 10
Not at all fatigued Extreme fatigue
4- Rate your level of fatigue right now.
0 1 2 3 4 5 6 7 8 9 10
Not at all fatigued Extreme fatigue
5-Rate how much in the past week, fatigue interfered with your level of activity.
0 1 2 3 4 5 6 7 8 9 10
No interference Extreme interference
6-Rate how much, in the past week fatigue interfered with your ability to bathe and dress yourself.
0 1 2 3 4 5 6 7 8 9 10
No interference Extreme interference
7- Rate how much, in the past week fatigue interfered with your normal activity (includes both work outside the home and housework).
0 1 2 3 4 5 6 7 8 9 10
No interference Extreme interference
8-Rate how much, in the past week fatigue interfered with your ability to concentrate.
0 1 2 3 4 5 6 7 8 9 10
No interference Extreme interference
9- Rate how much, in the past week fatigue interfered with your relations with other people.
0 1 2 3 4 5 6 7 8 9 10
No interference Extreme interference
10- Rate how much, in the past week fatigue interfered with your enjoyment of life.
0 1 2 3 4 5 6 7 8 9 10
No interference Extreme interference
11- Rate how much, in the past week fatigue interfered with your mood.
0 1 2 3 4 5 6 7 8 9 10
No interference Extreme interference
12-Indicate how many days, in the past week, you felt fatigued for any part of the day.
0 1 2 3 4 5 6 7 days
13- Rate how much of the day, on average, you felt fatigued in the past week.
0 1 2 3 4 5 6 7 8 9 10
None of the day The entire day
14-Indicate which of the following best describes the daily pattern of your fatigue in the past week
0 1 2 3 4
0=notatallfatigued,1=worseinthemorning,2=worseintheafternoon,
3=worseintheevening,4=noconsistentdailypatternoffatigue.
r
e
f
e
r
e
n
c
e
s
1. KhanF.Rehabilitationforpostpoliosequelae.AustFam
Physician.2004;33:621–4.
2. SilverJK,AielloDD.Whatinternistsneedtoknowabout
postpoliosyndrome.CleveClinJMed.2002;69:704–6,
709–12.
3. ÖstlundG,WahlinÅ,SunnerhagenKS,BorgK.Postpolio
syndrome:fatiguedpatientsaspecificsubgroup?JRehabil
Med.2011;43:39–45.
4. HalsteadLS,RossiCD.Newproblemsinoldpoliopatients:
resultsofasurveyof539poliosurvivors.Orthopedics.
1985;8:845–50.
5. MedicalResearchCouncil.Aidstotheexaminationofthe
peripheralnervoussystem.London:HMSO;1981.p.1.
6.KucukdeveciAA,McKennaSP,KutlayS,GurselY,WhalleyD,
ArasilT.Thedevelopmentandpsychometricassessmentof
TurkishversionofNottinghamHealthProfile.IntJRehabil
Res.2000;23:31–8.
7.BeckAT,WardCH,MendelsonM,MockJ,ErbaughJ.An
inventoryformeasuringdepression.ArchGenPsychiatry.
1961;4:561–71.
8.OksuzE,MalhanS,TulunayFC.Reliabilityandvalidityofthe
FatigueSymptomInventory.Movingandimprovingconcepts
andevidenceforhealthcaredecisions.Ispor11thAnnual
EuropeanCongress2008Nov8–11;Athens,Greece.Value
Health.2008;11:A426.
9.DonovanKA,JacobsenPB.TheFatigueSymptomInventory:a
systematicreviewofitspsychometricproperties.Support
10.HannDM,DennistonMM,BakerF.Measurementoffatiguein
cancerpatients:furthervalidationoftheFatigueSymptom
Inventory.QualLifeRes.2000;9:847–54.
11.HannDM,JacobsenPB,AzzarelloLM,MartinSC,CurranSL,
FieldsKK,etal.Measurementoffatigueincancerpatients:
developmentandvalidationoftheFatigueSymptom
Inventory.QualLifeRes.1998;7:301–10.
12.McNaughtonH,McPhersonK,FalknerE,TaylorW.
Impairment,disability,handicap,andparticipationin
post-poliomyelitissubjects.IntJRehabilRes.2001;24:133–6.
13.JacobT,ShapiraA.Qualityoflifeandhealthconditions
reportedfromtwopost-polioclinicsinIsrael.JRehabilMed.
2010;42:377–9.
14.TateDG,ForchheimerM,KirschN,MaynardF,RollerA.
Prevalenceandassociatedfeaturesofdepressionand
psychologicaldistressinpoliosurvivors.ArchPhysMed
Rehabil.1993;74:1056–60.
15.SchankeAK,StanghelleJK.Fatigueinpoliosurvivors.Spinal
Cord.2000;39:243–51.
16.ConradyLJ,WishJR,AgreJC,RodriquezAA,SperlingKB.
Psychologiccharacteristicsofpoliosurvivors:apreliminary
report.ArchPhysMedRehabil.1989;70:458–63.
17.HazendonkKM,CroweSF.Aneuropsychologicalstudyofthe
postpoliosyndrome:supportfordepressionwithout
neuropsychologicalimpairment.Neuropsychiatry
NeuropsycholBehavNeurol.2000;13:112–8.
18.OnAY,OncuJ,AtamazF,DurmazB.Impactof
post-polio-relatedfatigueonqualityoflife.JRehabilMed.
2006;38:329–32.
19.BerrylMH,StrauserWW,HallKM.Fatigueinpostpolio
syndrome.ArchPhysMedRehabil.1991;72:115–8.
20.PackerTL,SauriolA,BrouwerB.Fatiguesecondarytochronic
illness:postpoliosyndrome,chronicfatiguesyndrome,and
multiplesclerosis.ArchPhysMedRehabil.1994;75:
1122–6.
21.DittnerAJ,WesselySC,BrownRG.Theassessmentoffatigue:
apracticalguideforcliniciansandresearchers.JPsychosom
Res.2004;56:157–70.
22.NolletF,BeelenA,PrinsMH,DeVisserM,SargeantAJ,
LankhorstGJ,etal.Disabilityandfunctionalassessmentin
formerpoliopatientswithandwithoutpostpoliosyndrome.
ArchPhysMedRehabil.1999;80:136–43.
23.CondeMT,OliveiraAS,QuadrosAA,MoreiraGA,SilvaHC,
PereiraRD,etal.Post-poliosyndrome:epidemiologicand
prognosticaspectsinBrazil.ActaNeurolScand.
2009;120:191–7.
24.VanKralingenKW,IvanyiB,VanKeimpemaAR,VenmansBJ,
DeVisserM,PostmusPE.Sleepcomplaintsinpostpolio
syndrome.ArchPhysMedRehabil.1996;77:609–11.
25.ÖstlundG,WahlinA,SunnerhagenKS,BorgK.Vitalityamong
Swedishpatientswithpolio:aphysiologicalphenomenon.J