rev bras hematol hemoter. 2016;38(4):310–313
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Determination
of
reference
ranges
for
immature
platelet
and
reticulocyte
fractions
and
reticulocyte
hemoglobin
equivalent
Iuri
Vicente
Camargo
Morkis
∗,
Mariela
Granero
Farias,
Luciana
Scotti
HospitaldeClínicasdePortoAlegre(HCPA),PortoAlegre,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14April2016 Accepted6July2016
Availableonline6August2016
Keywords:
Referenceinterval Immatureplateletfraction Immaturereticulocytefraction
a
b
s
t
r
a
c
t
Introduction:Theimmatureplateletandimmaturereticulocytefractionsrepresenttheratios ofplateletsandreticulocytesrecentlyreleasedintothecirculationandthuswithhigherRNA content.Theyareconsideredearlyindicatorsofbonemarrowrecovery.
Objective:Theaimofthisstudywastodeterminethereferencerangesfortheimmature plateletandreticulocytefractionsofhematologicallynormalindividualsina university hospital.
Methods:VenousbloodsamplescollectedinethylenediaminetetraaceticacidK3were ana-lyzedusingaSysmexXE-5000TManalyzer.Individualswithplateletandreticulocytecounts
withinthereferenceranges,andabloodcountwithinthelaboratory’sscreeningcriteria wereincluded.Individualswithclinicalconditionsthatcouldaffecthematologicalresults wereexcluded.Theimmatureplateletfraction,high,mediumandlowfluorescence retic-ulocytefractionsandreticulocytehemoglobinequivalentwereevaluated.Thereference rangesweredeterminedaccordingtotherecommendationsoftheInternationalFederation ofClinicalChemistry.
Results:Onehundredandthirty-twooutpatientswereevaluated.The meanagewas44 years(range:13–80years),72(54.5%)werewomentreatedina universityhospital.The meanplateletcountwas250.8×109/Landthemeanreticulocytecountwas0.052×109/L.
Thefollowingreferencerangeswereobtained:immaturereticulocytefraction1.6–12.1%, thehigh,medium andlowfluorescence reticulocytefractionswere0.0–1.7%, 1.6–11.0% and87.9–98.4%,respectively,thereticulocytehemoglobinequivalentwas30.0–37.6%and immatureplateletfractionwas0.8–5.6%.Therewasastatisticallysignificantdifference(p -value=0.006)betweengendersinrespecttotheimmatureplateletfractionwith0.8–4.7%for femalesand0.7–6.1%formales.Theimmaturereticulocytefractionwasdirectlycorrelated withthereticulocytecount.
∗ Correspondingauthorat:HospitaldeClínicasdePortoAlegre(HCPA),RuaRamiroBarcelos,2350,90035-903PortoAlegre,RS,Brazil. E-mailaddress:[email protected](I.V.Morkis).
http://dx.doi.org/10.1016/j.bjhh.2016.07.001
revbrashematolhemoter.2016;38(4):310–313
311
Conclusion: Determining the reference range is critical to the introduction of a new parameter. The reference rangesobtained hereincorroborate those reported in previ-ous publications and will contribute to the clinical and laboratory application of the indices.
©2016Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Recentadvancesinthefield ofhematology analyzersused inclinicallaboratoriesallowthedeterminationofadditional hematologicparameters,providingusefulinformationforthe diagnosisand/ortreatment ofvarious pathologies.1 Among
theseparametersaretheimmaturefractionsofplateletsand reticulocytes.1–3
Theimmatureplateletfraction(IPF)andimmature retic-ulocytefraction(IRF)areyoungcellsthathaverecentlybeen releasedinto thecirculation, andare consideredindicators of bone marrow recovery.1–3 They are important in
vari-ousclinical situations, suchas thrombocytopenia, anemia, bonemarrowregenerationfollowingthe transplantation of hematopoieticstemcellsandafterchemotherapy.2,4–13
The IPF and IRF are determined using hematology analyzers with fluorescence and light scatter technology. ImmaturefractionshavelargeramountsofRNAthanmature plateletsandreticulocytes.Thus,theuseoffluorescentprobes thatlabel the RNApermitthe differentiation and quantifi-cationoftheIRFandIPF.1–3,6 Automatedsystemsprovidea
graphicdisplayofthedifferentpopulationsaccordingtothe sizeandamountofRNA.Basedonthis,theindicesare calcu-latedasapercentageoftotalreticulocytesandplatelets.1–3,6
Differentpopulationsofreticulocytesareseparated accord-ingtothesizeandtheamountofRNAandclassifiedasbeing low(LFR),medium(MFR) orhigh(HFR) fluorescence reticu-locytefractions.Thecombinedcountsofthe HFRand MFR correspond to IRF. The reticulocyte hemoglobin equivalent (Ret-He)parametercorrespondstothehemoglobincontentof thereticulocytes,andisstudiedasanindicatorofthe incor-porationofironinreticulocytes.15–18
Advancesinautomationhaveprovidedadditionalblood count parameters that enable new interpretations of the examination. However, clinical application can only occur oncethereferencerangeshavebeendeterminedwith knowl-edgeofpre-analyticalvariables(time,temperature, anticoag-ulants)andstandardizationofthemethodology.1,2,16,17,19–21
Somereferencerangeshavebeencalculatedbythe man-ufacturer,whileothershavenotyetbeendetermined.Thus, itisrecommendedthateachlaboratorycalculatesthe refer-encerangeforitspopulation,takingintoaccounttheroutine andthemethodologyused.22–24Subjectsshouldbestratified
byageandgenderandmeetstrictcriteriaintheselectionof theindividualsinthepre-analyticalandanalyticalphasesand forstatisticalanalysis.22–24
Thisstudyaimstodeterminethereferencerangesforthe IPF,IRF,LFR,MFR,HFRandRet-HEinhematologicallynormal patientstreatedatauniversityhospital,inordertostudythe rolesoftheparametersaspredictorsofengraftmentinbone
marrow transplantation,oneoftheirmainclinical applica-tions.
Methods
Venousbloodsamplescollectedin ethylenediaminetetraace-ticacidK3(EDTA-K3)wereanalyzedinaSysmexXE-5000TM analyzer(SysmexCorporation,Japan).Tominimizevariations due to sampleage, all assays were performed within four hoursofcollection;thesampleswerekeptatroom temper-atureuntilthetimeofanalysis.Theanalyzerusesthesame reagenttomeasuretheIPFandIRFinthereticulocytechannel. The platelet detection method employs hydrodynamic focusanddirectcurrenttechnology.TheIPFandIRFare deter-mined by fluorescence and light scatter using fluorescent RNA markers.1–3 TheRet-He isobtainedbyflowcytometry
technologyusingapolymethinedye,specificforRNA/DNA. Theforwardlightscatterintensitycorrelatestothecellular hemoglobincontent.
Patients withnormalblood countswithinthescreening criteria established by the laboratory such as hemoglobin greaterthan12.0g/dLandplateletandreticulocytecount val-ues withinthe normal ranges (platelet count greater than 150.0×109/Landreticulocytes25–80×109/L)wereincluded. Patientswithdiabetes,humanimmunodeficiencyvirus(HIV), cardiovascular diseases,pregnant women,hematologic dis-eases, cancer,and thyroid disease were excluded, asthese conditionsmayaffectthehematologicalresults.19–21
TheIPF,IRF,thereticulocyteratios(HFR,MFRandLFR)and Ret-Hewere evaluated. Assayswereroutinely submittedto internalandexternalqualitycontrols.
Statisticalanalysis
ThereferencerangesweredeterminedusingoftheStatistical PackageforSocialSciencesversion18.0(SPSSInc.,Chicago, IL,USA).Symmetricvariablesareexpressedasthemeanand standarddeviation,whileasymmetricvariablesareexpressed asthemedian,2.5–97.5percentileswithina95%confidence interval,asrecommendedbytheInternationalFederationof ClinicalChemistry(IFCC).22–24Spearman’sandPearson’s
cor-relationtestswerealsoused.
Results
312
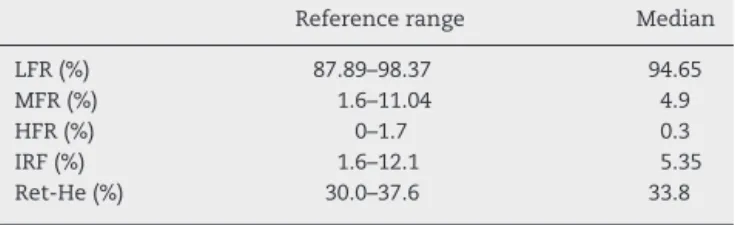
revbrashematolhemoter.2016;38(4):310–313Table1–Referenceintervalandmedianforreticulocyte index.
Referencerange Median
LFR(%) 87.89–98.37 94.65
MFR(%) 1.6–11.04 4.9
HFR(%) 0–1.7 0.3
IRF(%) 1.6–12.1 5.35
Ret-He(%) 30.0–37.6 33.8
LFR:lowfluorescenceratio;MFR:mediumfluorescenceratio;HFR: highfluorescenceratio;IRF:immaturereticulocytefraction;Ret-He: reticulocytehemoglobinequivalent.
Table2–Referencerangeandmedianforimmature plateletfraction.
Referencerange Median
Women(%) 0.7–4.7 2.0
Men(%) 0.6–6.1 2.6
Total(%) 0.8–5.5 2.2
concentration was 1.1% (range: 0.6–1.7%) with a count of 52×109/L(range:49–54×109/L).
Themedian valueof the IRF was 5.3% witha range of 1.6–12.1%.ThereferencerangesoftheHFR,MFRandLFRwere 0.0–1.7%, 1.6–11.0%and 87.9–98.4%, respectively. Themean Ret-Hewas33.8%witharangeof30.0–37.6%(Table1).
The median IPF was 2.2% with a range of 0.8–5.6%. A statistically significant difference (p-value=0.006) between genderswas onlyfound forthe IPF, with 2.0%forfemales (range:0.8–4.7%)and2.6%formales(range:0.7–6.1%).TheIRF presentedadirectcorrelation(SpearmanRank-order Coeffi-cient=0.40)withthereticulocytecount(Table2).
Discussion
Althoughnotdirectlyusedinclinicaldecisionmaking,the ref-erencerangeiscriticaltotheintroductionofnewparameters andtheinterpretationoflaboratoryresults.22–24Thereference
rangeshowsthevariationoflikelyvaluesin‘healthy’ individ-ualswhodonotpresentclinicalconditionsthatcanaffectthe studiedvariables.22–24
Immatureplatelets and immaturereticulocytesare pre-cursor cells recently released into the blood stream that containlarger amounts of RNA. Thus, they can be distin-guished from the mature platelets and reticulocytes and quantifiedusingRNAfluorescentlabeling.1–3 Severalstudies
havedemonstratedthevalueoftheseindicesinthecontext ofhematopoieticstem celltransplantation as indicatorsof hematopoiesis,intransfusionassessmentandthe anticipa-tionofsuccessfulengraftment.1–8TheRet-Heisusefulinthe
evaluationofhematopoiesis,withrespecttotheincorporation ofiron.14–17
ThereferencerangeobtainedfortheIPFwasinaccordance withthestudiesbyTakamietal.(mean2.0%;range:0.5–5.7%),9
Gonzaloetal.(median:2.3%;range:0.6–7.2%),4Yamaokaetal.
(meanof3.0±1%),8andBriggsetal.(range:1.1–6.1%).2 The
studybyKoetal.foundlowerIPFvalues(range:0.5–3.3%).18
ThereferencerangefortheIRFwassimilartothatof Gon-zaloetal.whoobtainedamedianof4.7%(range:1.1–11.4%).4
Althoughtheyusedthesamemethodology,thesestudieswere conducted with the use of a Sysmex XE-2100TM analyzer. Other authors employedother methodologiestodetermine thereferencerangesfortheIPFandIRFandsotheywerenot comparedwiththeresultsofthecurrentstudy.
Determining the reference range involves several steps, including selectionofsubjects, methodologyand statistical analysis.22–24Itisessentialthatitiscarriedoutfornew
param-etersthatarenotwidelyusedbylaboratoriesandclinics.The referencerangesfortheIRFandIPFreportedinthisstudyare consistentwiththeliteratureandwillcontributetotheclinical applicationoftheseindices.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgement
We would like tothank the staff atthe Hematology Unit, DepartmentofClinicalPathology,HospitaldeClínicasdePorto Alegre.
r
e
f
e
r
e
n
c
e
s
1.PivaE,BrugnaraC,ChiandettiL,PlebaniM.Automated reticulocytecounting:stateoftheartandclinical
applicationsintheevaluationoferythropoiesis.ClinChem LabMed.2010;48(10):1369–80.
2.BriggsC,KunkaS,HartD,OguniS,MachinSJ.Assessmentof animmatureplateletfraction(IPF)inperipheral
thrombocytopenia.BrJHaematol.2004;126(1):93–9. 3.BrugnaraC.Useofreticulocytecellularindicesinthe
diagnosisandtreatmentofhematologicaldisorders.IntJClin LabRes.1998;28(1):1–11.
4.Gonc¸aloAP,BarbosaIL,CampilhoF,CamposA,MendesC. Predictivevalueofimmaturereticulocyteandplatelet fractionsinhematopoieticrecoveryofallograftpatients. TransplantProc.2011;43(1):241–3.
5.MolinaJR,Sanchez-GarciaJ,TorresA,AlvarezMA,SerranoJ, Casa ˜noJ,etal.Reticulocytematurationparametersare reliableearlypredictorsofhematopoieticengraftmentafter allogeneicstemcelltransplantation.BiolBloodMarrow Transplant.2007;13(2):172–82.
6.BriggsC,HartD,KunkaS,OguniS,MachinSJ.Immature plateletfractionmeasurement:afutureguidetoplatelet transfusionrequirementafterhaematopoieticstemcell transplantation.TransfusMed.2006;16(2):101–9.
7.GrazziuttiML,DongL,MiceliMH,Cottler-FoxM,KrishnaSG, FassasA,etal.Recoveryfromneutropeniacanbepredicted bytheimmaturereticulocytefractionseveraldaysbefore neutrophilrecoveryinautologousstemcelltransplant recipients.BoneMarrowTransplant.2006;37(4):403–9. 8.YamaokaG,KubotaY,NomuraT,InageT,AraiT,KitanakaA,
etal.Theimmatureplateletfractionisausefulmarkerfor predictingthetimingofplateletrecoveryinpatientswith cancerafterchemotherapyandhematopoieticstemcell transplantation.IntJLabHematol.2010;326Pt1:e208–16. 9.TakamiA,ShibayamaM,OritoM,OmoteM,OkumuraH,
revbrashematolhemoter.2016;38(4):310–313
313
ofplateletengraftmentafterallogeneicstemcell
transplantation.BoneMarrowTransplant.2007;39(8):501–7. 10.HennelE,KentoucheK,BeckJ,KiehntopfM,BoeerK.
Immatureplateletfractionasmarkerforplateletrecovery afterstemcelltransplantationinchildren.ClinBiochem. 2012;45(10-11):749–52.
11.CremerM,WeimannA,SzekessyD,HammerH,BührerC, DameC.Lowimmatureplateletfractionsuggestsdecreased megakaryopoiesisinneonateswithsepsisornecrotizing enterocolitis.JPerinatol.2013;33(8):622–6.
12.BatT,LeitmanSF,CalvoKR,ChauvetD,DunbarCE. Measurementoftheabsoluteimmatureplateletnumber reflectsmarrowproductionandisnotimpactedbyplatelet transfusion.Transfusion.2013;53(6):1201–4.
13.StraussG,VollertC,vonStackelbergA,WeimannA,Gaedicke G,SchulzeH.Immatureplateletcount:asimpleparameter fordistinguishingthrombocytopeniainpediatricacute lymphocyticleukemiafromimmunethrombocytopenia. PediatrBloodCancer.2011;57(4):641–7.
14.RileyRS,Ben-EzraJM,TidwellA,RomagnoliG.Reticulocyte analysisbyflowcytometryandotherstechniques.Hematol OncolClinNorthAm.2002;16(2):373–420,vii.
15.BrugnaraC,SchillerB,MoranJ.Reticulocytehemoglobin equivalent(RetHe)andassessmentofiron-deficientstates. ClinLabHaematol.2006;28(5):303–8.
16.WatanabeK,KawaiY,TakeuchiK,ShimizuN,IriH,IkedaY, etal.Reticulocytematurityasanindicatorforestimating
qualitativeabnormalityoferythropoiesis.JClinPathol. 1994;47(8):736–9.
17.BrugnaraC.Irondeficiencyanderythropoiesis:new diagnosticapproaches.ClinChem.2003;49(10):1573–8. 18.KoYJ,KimH,HurM,ChoiSG,MoonHW,YunYM,etal.
Establishmentofreferenceintervalforimmatureplatelet fraction.IntJLabHematol.2013;35(5):528–33.
19.GiacominiA,LegoviniP,GessoniG,AnticoF,ValverdeS, SalvadegoMM,etal.Plateletcountandparameters
determinedbytheBayerADVIA120inreferencesubjectsand patients.ClinLabHaematol.2001;23(3):181–6.
20.ButkiewiczAM,KemonaH,Dymicka-PiekarskaV, Matowicka-KarnaJ,RadziwonP,LipskaA.Plateletcount, meanplateletvolumeandthrombocitopoieticindicesin healthywomenandmen.ThrombRes.2006;118(2):199–204. 21.ZandeckiM,GenevieveF,GerardJ,GodonA.Spuriouscount
andspuriousresultsonhaematologyanalysers:areview.Part I:platelets.IntJLabHematol.2007;29(1):4–20.
22.SiestG,HennyJ,GräsbeckR,WildingP,PetitclercC,Queraltó JM,etal.Thetheoryofreferencevalues:anunfinished symphony.ClinChemLabMed.2013;51(1):47–64. 23.SolbergHE.TheIFCCrecommendationonestimationof
referenceintervals.TheRefValProgram.ClinChemLabMed. 2004;42(7):710–4.