www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Refractory
episodic
vertigo:
role
of
intratympanic
gentamicin
and
vestibular
evoked
myogenic
potentials
夽
,
夽夽
Erika
Celis-Aguilar
a,∗,
Ramon
Hinojosa-González
b,
Olivia
Vales-Hidalgo
b,
Heloisa
Coutinho-Toledo
caUniversidadAutónomadeSinaloa,CentrodeInvestigaciónyDocenciaenCienciasdelaSalud(CIDOCS),Departamentode
Otorrinolaringología,Culiacán,Sinaloa,Mexico
bInstitutoNacionaldeNeurologíayNeurocirugíaManuelVelascoSuárez,DepartmentofNeurotology,CiudaddeMéxico,Mexico cHospitalMédicaSur,CiudaddeMéxico,Mexico
Received16August2015;accepted29November2015 Availableonline28March2016
KEYWORDS
Vestibularevoked myogenicpotentials; Refractoryvertigo; Intratympanic gentamicin; Menieredisease
Abstract
Introduction:Eventoday,thetreatmentofintractablevertigoremainsachallenge.Vestibular ablationwithintratympanicgentamicin standsasa goodalternativeinthe managementof refractoryvertigopatients.
Objective:Tocontrolintractablevertigothroughcompletesaccularandhorizontalcanal ves-tibularablationwithintratympanicgentamicintreatment.
Methods:Patientswithrefractoryepisodicvertigowereincluded.Theinclusioncriteriawere: unilateraleardisease,moderatetoprofoundsensorineuralhearingloss,andfailuretoother treatments.Includedpatientsunderwent0.5---0.8mLofgentamicinintratympanicapplication ata30mg/mLconcentration.Vestibularablationwasconfirmedbytheabsenceofresponse oncervicalvestibularevokedmyogenicpotentialsandnoresponseoncalorictests. Audiome-try,electronystagmographywithicedwater,andvestibularevokedmyogenicpotentialswere performedinallpatients.
Results:Tenpatientswereincluded;ninepatientswithMeniere’sdiseaseandonepatientwith (lateonset)delayedhydrops.Ninepatientsshowedanabsentresponseonvestibularevoked myogenicpotentials andnoresponseoncaloric tests.The onlypatient withlowamplitude oncervicalvestibularevokedmyogenicpotentialshadvertigorecurrence.Vertigocontrolwas achievedin90%ofthepatients.Onepatientdevelopedhearingloss>30dB.
夽 Pleasecitethisarticleas:Celis-AguilarE,GonzálezRH, HidalgoOV,ToledoHC. Refractoryepisodicvertigo:role ofintratympanic
gentamicinandvestibularevokedmyogenicpotentials.BrazJOtorhinolaryngol.2016;82:668---73.
夽夽ThisstudywaspresentedattheAmericanAcademyofOtolaryngology,2014,Orlando,Florida.
∗Correspondingauthor.
E-mail:[email protected](E.Celis-Aguilar).
http://dx.doi.org/10.1016/j.bjorl.2015.11.019
1808-8694/©2016Associac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.PublishedbyElsevierEditoraLtda.Thisisanopen
Conclusions: Cervicalvestibularevoked myogenicpotentialsconfirmedvestibularablationin patientstreatedwithintratympanicgentamicin.High-gradevertigocontrolwasduetocomplete saccularandhorizontalcanalablation(noresponsetoicedwaterinelectronystagmographyand noresponseoncervicalvestibularevokedmyogenicpotentials).
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Potencialevocado miogênicovestibular; Vertigemrefratária; Gentamicina intratimpânica; Doenc¸adeMénière
Vertigemrefratáriaepisódica:papeldagentamicinaintratimpânicaepotencial evocadomiogênicovestibular
Resumo
Introduc¸ão: Aindahoje,ocontroledavertigemintratávelpermaneceum desafio.Aablac¸ão vestibularcomgentamicinaintratimpânicapermanececomoumaboaalternativanotratamento depacientescomvertigemrefratária.
Objetivo: Controlaravertigemintratávelpormeiodeablac¸ãovestibularcompletadoscanais sacularehorizontalcomgentamicinaintratimpânicacomotratamento.
Método: Pacientescomvertigemrefratáriaepisódicaforamincluídos.Oscritériosdeinclusão foramdoenc¸a unilateraldaorelha,perdaauditiva neurossensorialdemoderadaaprofunda e fracasso com outros tratamentos. Os pacientes incluídos receberam uma aplicac¸ão de 0,5---0,8mL de gentamicinaintratimpânica comconcentrac¸ão de 30mg/mL. A ablac¸ão ves-tibular foi confirmada pela ausência de resposta no teste de potencial evocadomiogênico vestibular cervical(PEMVc)e nenhumarespostanasprovascalóricas. Audiometria, eletron-istagmografiacomáguageladaepotencialevocadomiogênicovestibularforamrealizadosem todosospacientes.
Resultados: Aotodo,dezpacientesforamincluídos:novecomdoenc¸adeMénièreeumcom hidropisiatardia. Novepacientes apresentaram ausência deresposta noteste depotencial evocadomiogênico vestibularenenhuma respostanaprovacalórica.Oúnicopaciente com baixa amplitudeno PEMVcapresentou recorrência davertigem. Ocontroledavertigemfoi obtidoem90%dospacientes.Umpacientedesenvolveuperdaauditiva>30dB.
Conclusões: OPEMVcconfirmouablac¸ãovestibular nos pacientestratados comgentamicina intratimpânica.Oaltograudecontroledavertigemfoidevidoàablac¸ãocompletadosáculo ecanalhorizontal(semrespostaàáguageladanaeletronistagmografiaeausênciaderesposta noPEMVc).
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Vertigo control is the main outcome in the treatment of Meniere’s disease; nevertheless, many patients do not respondtoconservativemeasures.Moreinvasiveprocedures are preserved for those patients with intractable vertigo andnoresponsetomedicaltreatment.Surgicaltreatments, particularly vestibularnerve section, have a high success rate.Nonetheless,asasurgicalprocedure,sideeffectssuch as headache, bleeding, cerebrospinal fluid (CSF) leak, or facialparalysis,amongothers,arepossible.Forthisreason, intratympanicgentamycintreatmentisgraduallyreplacing thesesurgicalprocedures.
In 1957 Schuknecht1,2 wasthefirst todescribetheuse
ofaminoglucosides inthe treatment ofMeniere’s disease. He described the instillation of streptomycin in the mid-dleearoffivepatients,withgoodvertigocontrol,although withadversecochlearsideeffects,asprofoundhearingloss developedinallpatients.
Sincethen,numerousstudiesofintratympanic gentami-cinhavedemonstrateda76---96%vertigocontrolrate,with ariskofhearinglossaround20---30%.1,2
Interestingly,gentamicininstillations arecurrently still controversial. Dose, number of applications, and period between each application has not reach a consensus between otologists. In 2004, a meta-analysis2 described
fivedifferenttechniques ofgentamicinapplications:daily (three daily applications for at least four days), weekly dose (oneeach week for atotal of fourdoses), low dose (one or two applications, with new treatment if vertigo recurrence),continuousapplicationwithmicrocatheter,and titrationtherapy (weekly or daily dose untilvestibular or cochlearsymptomsoccur).Chiaetal.2concluded,according
Ontheotherhand,cervicalvestibularevokedmyogenic potentials (cVEMPs) were first described by Colebatch in 19943;sincethen,cVEMPshavebeenaknowntestfor
saccu-larfunctionandinferiorvestibularnerve.Inhumans,intense auditory clicks and tone bursts stimulate afferent saccu-larpathwaysthatinhibitsternocleidomastoidmuscletone, whichisrecordedonthistest.Theresultisapositivewave p1,followedbyanegativewaven1.
Furthermore,saccular functionhas been found altered inpatientwithrecentlydiagnosisofMeniere’sdisease.4Itis
believedthatcompletevestibularfunction,including saccu-larfunction,shouldbemeasuredingentamicintreatment. Moreover, the rehabilitation of a patient who undergoes gentamicintreatmentdependsontheamountofvestibular damagepresent.5
Disadvantages of intratympanic gentamicin are mainly hearingloss6andchronicsubjectivedizziness.
Evaluationof thesaccular functionis paramountifthe goalofvestibularablationwithintratympanicgentamicinis completeablation,andcVEMPscouldaddtothediagnostic work-upandfollow-upofthesepatients.Thistestcouldalso showvestibularresidualfunctioninapatientwithrecurrent vertigopost-gentamicintreatment.
Complete vestibular ablation vs. partial ablation is a subjectof controversy.Unfortunately,reports onhowthis vestibular ablation is obtained are varied. To determine completevestibularablation,studiesshouldinclude evalua-tionofsemicircularcanals,aswellasutricularandsaccular function.
Vestibular ablation in this study was defined as zero response on the caloric tests with ice water and absent responseoncVEMPs,i.e.,completeablationofsaccularand horizontalsemicircularcanalfunction.
The objectiveof this study was toassess vertigo con-trolin patientswithintractablerefractoryvertigotreated withintratympanicgentamicinandvestibularablation, con-firmedbyanabsentresponseoncVEMPsandzeroresponse intheicewatertestonelectronystagmography(ENG).
Methods
Studydesign
Retrospective,clinicalchartreview.
Setting
Tertiarycarecenter.
Patients
Thisstudyincludedpatientswithintractablerecurrent ver-tigo,unilateralvestibulardisease,andcompletevestibular tests,fromJanuary 2002 toDecember 2010.Weekly gen-tamicin application was conducted in all patients. The applicationconsistedof0.5mlto0.8mlofgentamicin,with a concentration of 30mg/mL. This solution was buffered withbicarbonate.Inclusioncriteria:Allpatientsfulfilledthe criteriaforMeniere’sdiseaseaccordingtothe1995AAO-HNS committeeonhearingandequilibrium,hadage>18years,
moderate to profound hearing loss, and failure to other medicaltreatmentsincludingdexamethasoneintratympanic application.
Measurements
All patients underwent pure tone audiometryand speech audiometrywithanInteracousticAD29audiometer.ENGwas performedwithmicromedicalequipment.Oculomotortests (saccades,gazetesting,optokinetic,smoothpursuit track-ing),positionaltests,and calorictestswereperformed in allpatients.Vestibularasymmetrywasdefinedthroughthe calorictests, withan asymmetry of 30%compared tothe otherear.Zeroresponsewasdefinedasabsenceof nystag-muswithicedwater.
cVEMPs were performed with Nicolet Viking Select consistedofelectrodesplacedonthesternocleidomastoid, sternum,andipsilateralmastoid(groundelectrode). Stern-ocleidomastoidtonewasobtainedbyeffortelicitedbythe patient by means of a pole system with a weight of 2kg andaheadband.Thepatientthrustsforwardhis/her fore-head,maintainingmuscletone.Auditorystimuliconsistedof clicks,threepersecondat105dB(withacontralateralwhite noise of 45dB, and a filter of 10Hz---1.5kHz). Recordings wereconductedfor100ms(milliseconds).
Informed consent wasobtained fromall patients. This studywasapprovedbytheinstitutionalethicscommittee.
Intervention
Protocol of intratympanic gentamicin application: patient lays flat with 45◦ of head rotation,tetracaine solution is appliedtoearcanal,undermicroscopicviewtheanesthetic issuctioned,andwitha1mLsyringewith30mggentamicin, buffered with 1/3 NaHCO3; 0.4ml to 0.6ml is applied to themiddleear,intheinferiorquadrants.Thepatientsrests inthatpositionforoveronehour,andisinstructedtonot speakorswallow.Weeklyapplicationswereperformeduntil therewas an absentresponse both toice waterENG and cVEMPs.
Follow-up
Patientswerefollowedupwithevaluationsat30days,and three, six,and 12months.Posteriortotheseevaluations, followupwasdoneannually.Allpatientsunderwenta vesti-bularrehabilitationprogram,whichconsistedofenhancing the vestibulo-ocular reflex,sensorysubstitution, and pos-turalcontrol;each protocolwasindividualized.Duringthe patients’subsequentvisits,audiometrywasperformed,as wellasENGwithicewaterandmeasurementof the func-tionalscaleofMeniere’sdisease.
Statisticalanalysis
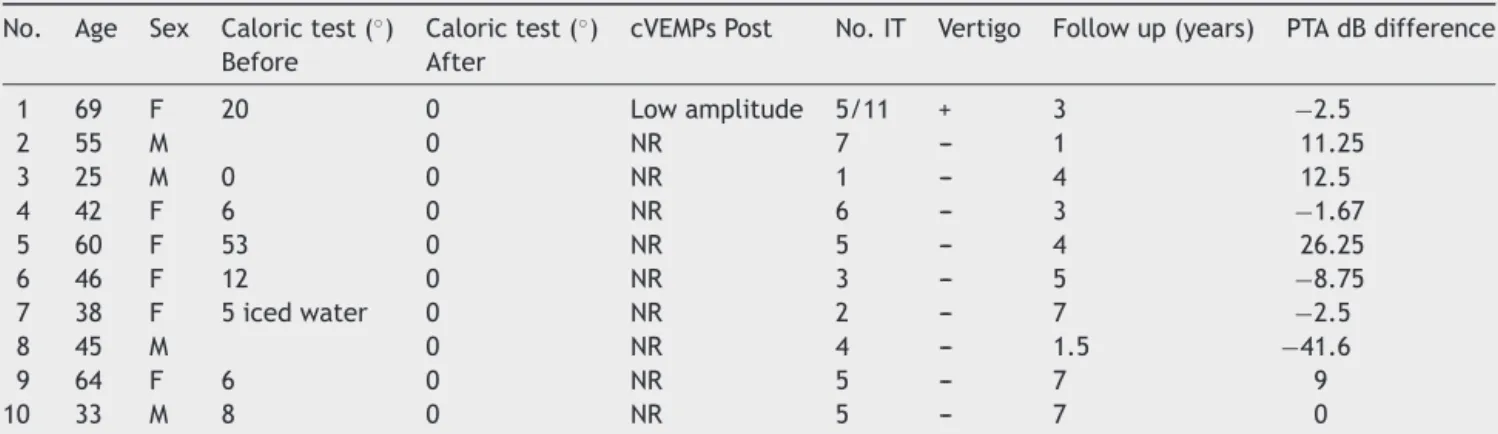
Table1 Patients’clinicalcharacteristics,intervention,andfollowup.
No. Age Sex Calorictest(◦) Calorictest(◦) cVEMPsPost No.IT Vertigo Followup(years) PTAdBdifference
Before After
1 69 F 20 0 Lowamplitude 5/11 + 3 −2.5
2 55 M 0 NR 7 --- 1 11.25
3 25 M 0 0 NR 1 --- 4 12.5
4 42 F 6 0 NR 6 --- 3 −1.67
5 60 F 53 0 NR 5 --- 4 26.25
6 46 F 12 0 NR 3 --- 5 −8.75
7 38 F 5icedwater 0 NR 2 --- 7 −2.5
8 45 M 0 NR 4 --- 1.5 −41.6
9 64 F 6 0 NR 5 --- 7 9
10 33 M 8 0 NR 5 --- 7 0
PTAdifference,puretoneaveragedifference(differenceofdBinaudiometrypre-andpost-intervention);negativevaluesrepresent hearinglossandpositivevalueshearinggainindB.
No.IT,numberofintratympanicgentamicinapplications;NR,noresponse;cVEMPs,cervicalvestibularevokedmyogenicpotentials.
Results
Tenpatientswereincludedwithcompletevestibulartests, bothENGandcVEMPs.NinepatientshadMeniere’sdisease andonepatienthaddelayedendolymphatichydrops.
Allpatientsunderwentintratympanicgentamicin appli-cation. The mean number of applications was 4.3 (range 1---7).Follow-upwasfromonetosevenyears,withamean of4.25years.
Vertigocontrolwas90%.Onepatientdevelopedhearing loss>30dB.SeeTable1forresults.
After gentamicin treatment, nine patients had absent response on cVEMPs and only one patient had persistent cVEMPsresponse.The latterpatient(patientNo.1onthe table)hadlowamplitudecVEMPswithsymptomatic recur-rentvertigo. This patientrequired twosetsofgentamicin applications;fiveand11applications,respectively.
AllpatientshadzeroresponseonicewaterENGposterior togentamicinapplication. ENGoculomotorand positional testswerenegativeinallpatients.
Twopatients(patientsNo.2and8)hadENGwith vesti-bularasymmetrypre-treatment(>25%),althoughnogrades of responseweredocumented;therefore, this datais not includedonTable1.
Previoustreatment
All patients had no response to medicaltreatment (diet, diuretics,steroids,vasodilators,calciumantagonists). Inter-estingly, two patients had dexamethasone intratympanic applicationwithoutgoodresults,aswellasonepatientwith endolymphaticsacdecompressionandonepatientwith pos-sibleincompletevestibularnervesection.
cVEMPSprevioustogentamicinapplication
Eventhoughallpatientshaddocumentedvestibularparesis (horizontalsemicircularcanalparesis)previousto gentami-cintreatment, onlytwo(patients No.3and 4)hadinitial pre-treatment cVEMPs. Both patients had low amplitude responsecVEMPs withposterior ablation of this response.
ThesepatientshadMeniere’s disease,witha meanageof 33.5years.
cVEMPsandvertigocontrol
Ninetypercentofthepatientshadgoodvertigocontrol.The onlypatientwithrecurrentvertigoattackswaspositiveon cVEMPsposteriortothesecondcourseofgentamicin appli-cation. This patient rejected surgical treatment and was subsequentlypartiallycontrolledwithmedicaltreatment.
Hearingloss
Onlyonepatienthadhearinglossmorethan30dB.Therest ofpatientshadameanhearinglossof5.70dB.
FunctionalclassofMeniere’sdisease
Fivepatientshad intermittentdizziness; theycontinue to work,drive,andengageinanyactivity.Thiscorrespondsto functionalclasslevels2and3.
TechnicaldifficultiesofcVEMPs
Four patients had to be eliminated from the database becauseofbilateralabsentresponseoncVEMPs.These tech-nicaldifficultieswereduetomorphologicalneckvariations (thickneck)orduetolackofcooperationfromthepatient (nosternocleidomastoidcontraction).
Discussion
(saccularandhorizontalsemicircularcanalfunction)could beachieved.
Inthisseries,absentresponseoncVEMPstestafter genta-micintreatmentwaspresentinallpatientswithgoodvertigo control.
Additionally, anabnormalresponsetocVEMPscouldbe anearlysymptomofMeniere’sdisease.Inpre-symptomatic ears,itcouldbeasignofdiseaseinthecontralateralear.4,7
In the present study, twopatients (patients No.3 and 4) had positive cVEMPs pre-treatment, and interestingly, bothhad low amplituderesponse.This corroborates what haspreviouslybeendescribedintheliterature,that saccu-lardamageispresentinMeniere’sdisease.4,5Otherauthors
havedescribedaninitialdamagetosemicircularcanalswith posteriorsaccularinjury.5
Patient No. 3 was a controversial case, since there waszero responseonicewaterENGbut cVEMPsresponse was present; gentamicin treatment was chosen due to persistentsaccularfunction.Aftergentamicinapplication, cVEMPswere negativeand icewater ENGpersisted nega-tiveafter twoyearsposterior tointervention. Duringthis timeposturographywasnormal, verifyingcomplete vesti-bularrehabilitation.Thispatientisfreeofvertigoattacks. cVEMPscouldbeofgreatdiagnosticvaluewhenapatient presentswithvertigo spellsandnoresponseonicewater ENG,sinceanothervestibularepithelium,e.g.thesaccule, couldberesponsibleforthevertigoattacks.
AnimalstudieshaveprovedthatcervicalVEMPsoriginate fromtypeIcellsinthesacculeofguineapigs.8Vestibularcell
regenerationafter gentamicinhasbeen described in both semicircularcanals8andthesaccule.7Thisvestibular
regen-erationis probablythe causeof recurrent vertigo attacks post-gentamicin.9However,otherauthorsexplainthatthis
isduetothenaturalhistoryofMeniere’sdisease,sincethe absenceofvertigoattacksinsomestudiesisduetoan insuf-ficientfollow-up,givingafalseideaoftherapysuccess.Long termfollow-upisstronglyadvised.7
Inthepresentseries,patientNo.1,afterthefirsttherapy ofgentamicin,hadgrade11vestibularresponseonicewater ENGandalsopresentedwithlowamplitudecVEMPs.After the second application of gentamicin, she persisted with vertigoattackswithpositivecVEMPs,supporting the asso-ciationofvestibulartestsandsymptoms,alreadydescribed bynumerousauthors.5,7,9,10
Helling etal.5 included in theirstudy 19 patients with
Meniere’s disease. After the first gentamicin application cVEMPswerenegative,theyconcludedthatcVEMPswerenot areliableindicatoroftherapysuccess.Thisdiffersfromthe presentresultssincetheonlypatientwithpositivecVEMPS wasthepatientwhohadrecurrentvertigo.Additionally, Pic-ciotti etal.11 emphasized the usedof cVEMPs to monitor
therapyefficacy.
PresenceofcVEMPsafterintratympanicgentamicincould bean indicatorof therapyfailure,at least inthe present study.Moreresearchismandatoryinordertoconfirmthese results.
Additionally,intratympanicgentamicindeliverymethods arehighlyvariable.AccordingtoChiaetal.,2thetitration
methoddemonstratedvertigo controlof81.7%vs. 75%for weeklydelivery.Theauthors’standarddeliverymethod,as previouslystated,isweeklyapplicationsuntilnoresponse on ice water ENG. Comparing these results with those
previously published, this study’s rate of vertigo control couldbesuperiortoothermethodsofgentamicindelivery.
Completevestibularablationisstillcontroversial,more sosincethe meta-analysisbyChia etal.2 didnotconfirm
astatisticaldifferencebetweenpartialandcomplete ves-tibular ablation (p=0.179). The datashow that complete vestibularablationinthismeta-analysisproduced92.1% ver-tigocontrolvs.74.8%forpartialablation.
Otherauthors5havepreferredpartialablation,
explain-ingthatpreservedcanalicularfunctioncouldachievevertigo control,becauseitproducedamorespecificdamagetothe darkcellsandthusprovidesendolymphproduction homeo-stasis. Nevertheless, the present study demonstrates that vestibularablation(asmeasuredbysaccularandhorizontal semicircularcanalablation)iseffectiveforvertigocontrol. Chia et al.2 described a 13.1% hearing loss with the
weeklygentamicindeliverymethod.Inthepresentseries, only onepatienthad hearingloss greaterthan 30dB, 10% ofthestudypopulation.Noneofthepatientshadprofound hearinglosssecondarytotheprocedure,vs.6.6%reported inotherliterature.2Themeanhearinglosswas5.7dB.This
rate of hearing loss is corroborated by other studies.5 Of
relevance,thereareothercentersthatapplyintratympanic gentamicin in normalhearing subjects,12 emphasizing the
lowrateofexpectedhearingloss.
Interestingly,inthisseries,fourpatientshadpure tone average(PTA)improvement.Thiscouldbeduetothe nat-uralcourseofMeniere’sdisease,whichincludesfluctuating hearingloss.
Utricular function has been described tobe preserved in 30%---40% of patients with intratympanic gentamicin treatment5; this differs from the saccule and
semicircu-larcanals, whichareinvariableinjuredbythistreatment. Unfortunately, this study did not evaluate utricular func-tion. Posturography hasalso been usedin these patients. Onestudydescribedanimprovementinthevestibular com-ponentsixmonthsaftergentamicinmiddleearapplication. Thereareseveralvenuesofresearchthathavebeen incom-pletelyexploredregardingthistreatment thatcouldbeof usebyfutureresearchers.
Thelimitationsofthisstudyareitsretrospectivenature, thelimitednumberofpatientsincluded,andthelackof pre-treatmentcVEMPsinsomepatients.However,onestrength ofthisstudyisthelong-termfollow-up,insomepatientsup tosevenyears.
Anotherlimitationis thefactthatthe ENGcalorictest representsonlyalowfrequencytestofvestibularfunction. The calorictestmeasures exclusivelythehorizontal semi-circular canalfunction; therefore, itcan beinferred that inthisstudy,onlypartialvestibularablationwasmeasured. Nevertheless, the ENG also measures a dynamic range of othertests,suchaspositionaltestingandoculomotortests (saccades, optokinetic,smooth pursuit,etc.),which were notalteredinanyofourpatients.
canalsobeevaluatedbytheheadimpulsetest,withor with-outFrenzelgoggles;calorictestscouldalsobeperformed if necessary, with only Frenzel goggles at the emergency department.
Moreover, the authors are aware of the lack of other vestibulartests,suchasocularVEMPs,videoheadimpulse test,andutricularfunction.Inthisstudy,althougha com-plete absence of the saccule and horizontal semicircular canalfunctionwasachieved,completevestibularfunction cannotbeassumedbecausenotallvestibularorganswere measured.
Nevertheless, this study adds evidence on the use of intratympanicgentamicinforcompleteablationofsaccule andhorizontalsemicircularcanalfunction.ENGcalorictests andcVEMPsshouldbeusetocorroboratevestibularablation.
Conclusions
cVEMPs confirmed vestibular ablation in patients treated withintratympanicgentamicin.High-gradevertigo control wasdue tocomplete saccular andhorizontal semicircular canal ablation (no response toiced water in ENG and no responseoncVEMPs).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.LalwaniA,McGuireJF.Pharmacologicandmoleculartherapies ofthecochlearandvestibularlabyrinth.In:FlintP,HaugheyB, LundV,NiparkoJ,RichardsonM,RobbinsK,etal.,editors. Cum-mingsotolaryngology--- headand necksurgery. Philadelphia: Mosby;2010.p.2179---93.
2.ChiaS,GamstA,AndersonJ,HarrisJ.Intratympanicgentamicin therapy forMénièredisease: ameta-analysis.OtolNeurotol. 2004;25:544---52.
3.Nguyen K, Welgampola M, Carey J. Test---retest reliability and age related characteristics of the ocular and cervical vestibular evoked myogenic potential tests. Otol Neurotol. 2010;31:793---802.
4.Waele C, Tran Ba Huy P, Diard JP, Freys G, Vidal PP. Sac-cular dysfunction in Meniere’s disease. Am J Otol. 1999;20: 223---32.
5.Helling K, Schönfeld U, Clarke A. Treatment of Meniere disease bylow dose dosage intratympanicgentamicin appli-cation: effect on otolith function. Laryngoscope. 2007;117: 2244---50.
6.YoussefTF,PoeDS.Intratympanicgentamicininjectionforthe treatmentofMeniere’sdisease.AmJOtol.1998;19:435---42.
7.Ozluoglu L, Akkuzu G, Ozgirgin N, Tarhan E. Reliability of the vestibular evoked myogenic potential test in assessing intratympanic gentamicintherapy in Meniere’sdisease. Acta Otolaryngol.2008;128:422---6.
8.LueJH,DayAS,ChengPW,YoungYH.Vestibularevoked myo-genic potentials are heavily dependent on type I hair cell activityofthesaccularmaculainguineapigs.AudiolNeurotol. 2009;14:59---66.
9.WaelwC,MeguenniR,FreyssG,ZamithF,BellalimatN,Vidal PP, et al. Intratympanic gentamicin injections for Meniere’s disease.Vestibularhaircellimpairmentandregeneration. Neu-rology.2002;59:1442---4.
10.WelgampoalaM,ColebatchJ.Characteristicsandclinical appli-cations ofvestibularevokedmyogenicpotentials. Neurology. 2005;64:1682---8.
11.Picciotti PM, Fiorita A, Nardo W, Quaranta N, Paludetti G, MauriziM.VEMPSand dynamicposturographyafter intratym-panic gentamicin inMeniere disease. J Vestib Res. 2005;15: 161---8.