www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Effects
of
vibrotactile
vestibular
substitution
on
vestibular
rehabilitation
---
preliminary
study
夽
,
夽夽
Cibele
Brugnera
a,∗,
Roseli
Saraiva
Moreira
Bittar
b,
Mário
Edvin
Greters
c,
Dietmar
Basta
daOtoneurologyOutpatientClinic,HospitaldasClínicas,FaculdadedeMedicina,UniversidadedeSãoPaulo(HCFMUSP),SãoPaulo, SP,Brazil
bHospitaldasClínicas,FaculdadedeMedicina,UniversidadedeSãoPaulo(HCFMUSP),SãoPaulo,SP,Brazil cHospitalCelsoPierro,PontifíciaUniversidadeCatólicadeCampinas(PUC-Campinas),Campinas,SP,Brazil dHospitalCharité,BerlinUniversity,Berlin,Germany
Received5May2014;accepted21October2014 Availableonline8September2015
KEYWORDS Dizziness;
Sensoryfeedback; Vestibulardiseases; Posturalbalance; Rehabilitation
Abstract
Introduction:Somepatientswithsevereimpairmentofbodybalancedonotobtainadequate improvementfromvestibularrehabilitation(VR).
Objective:ToevaluatetheeffectivenessofVertiguardTM biofeedbackequipmentasasensory
substitution(SS)ofthevestibularsysteminpatientswhodidnotobtainsufficientimprovement fromVR.
Methods:Thiswasarandomizedprospectiveclinicalstudy.Thirteenpatientswithout satisfac-toryresponseto conventionalVRwererandomizedinto astudygroup (SG),whichreceived thevibrotactilestimulusfromVertiguardTMfortendays,andacontrolgroup(CG),whichused
equipmentwithoutthestimulus.Forpre-andpost-treatmentassessment,theSensory Organi-zationTest(SOT)protocoloftheComputerizedDynamicPosturography(CDP)andtwoscalesof balanceself-perception,Activities-specific BalanceConfidence(ABC)andDizzinessHandicap Inventory(DHI),wereused.
Results:After treatment, only the SG showed statistically significant improvement in C5 (p=0.007)andC6(p=0.01).On theABCscale, therewasasignificantdifferenceintheSG (p=0.04).TheDHIshowed asignificantdifferenceinCG andSGwithregardtothephysical aspect,andonlyintheSGforthefunctionalaspect(p=0.04).
夽 Pleasecitethisarticleas:BrugneraC,BittarRSM,GretersME,BastaD.Effectsofvibrotactilevestibularsubstitutiononvestibular rehabilitation---preliminarystudy.BrazJOtorhinolaryngol.2015;81:616---21.
夽夽Institution:HospitaldasClínicas,MedicineSchool,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](C.Brugnera). http://dx.doi.org/10.1016/j.bjorl.2015.08.013
Conclusion: Thepresent findings showthat sensorysubstitution using thevibrotactile stim-ulus oftheVertiguardTM system helpedwiththe integrationofneural networksinvolvedin
maintainingposture,improvingthestrategiesusedintherecoveryofbodybalance.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE Vertigem;
Retroalimentac¸ão sensorial;
Doenc¸asvestibulares; Equilíbriopostural; Reabilitac¸ão
Efeitosdobiofeedbackvibrotátilnareabilitac¸ãodoequilíbriocorporal---estudo preliminar
Resumo
Introduc¸ão: Alguns pacientes com déficit severo do equilíbrio corporal submetidos à reabilitac¸ãovestibular(RV)podemnãoapresentarresultadossatisfatórios.
Objetivo: Verificar aeficáciado equipamentodebiofeedbackVertiguardTM como substituto
sensorialdosistemavestibularempacientessembonsresultadosàRV.
Método: Estudoprospectivoclínicorandomizado.TrezepacientessemrespostasatisfatóriaàRV convencionalforamrandomizadosentregrupodeestudo(GE),queutilizouoestímulovibratório doVertiguardTM pordezdiasegrupocontrole(GC)queusouoequipamentodesligado.Para
avaliac¸ãopréepós-tratamentofoiutilizadooprotocoloTestedeIntegrac¸ãoSensorial(TIS)da PosturografiaDinâmicaComputadorizada(PDC)eduasescalasdeautopercepc¸ãodoequilíbrio: ABC(Activities-specificBalanceConfidence)eDHI(DizzinessHandicapInventory).
Resultados: ApenasoGEapresentoumelhoraestatisticamentesignificanteem C5(p=0,007) e C6 (p=0,01)daPDC apóstreinamento.Na escala ABChouve diferenc¸asignificante noGE (p=0,04).NoDHIocorreudiferenc¸asignificantenoaspectofísico emambos osgrupose no aspectofuncional(p=0,04)apenasnoGE.
Conclusão:Oestímulodesubstituic¸ãosensorialdoVertiguardTMauxiliouaintegrac¸ãodasredes
neuraisenamanutenc¸ãodapostura,melhorandoasestratégiasutilizadasnarecuperac¸ãodo equilíbriocorporal.
©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Postural stability is achievedby the central processingof sensoryafferentscomposedof visual,vestibular,auditory, and proprioceptive information.1 The vestibular system,
responsible for theintegration ofthis information, deter-mines the appropriate motor response to information incoming from,and outgoingto, environmentaldemands. Thelossofvestibularinformationsetsinmotionastructural reorganizationofthecentralnervoussystem(CNS),that cre-atesnewneuralnetworkstoreplacethelostafferentinput.2
These changesare responsiblefor central compensation,3
whichoccursthankstoneuronalandneurochemical activ-itycausedbysensoryconflictsexperiencedintheabsence of vestibular information.4 Central compensation may be
accelerated by means of vestibular rehabilitation (VR),5
which usesphysical exercise torestore the main reflexes relatedtobodybalance.6,7Thisconceptofneural
reorgani-zationinordertoaddressthelossofvestibularfunctionhas beentermedsensorysubstitution(SS).8
SS can assist in the process of gait and posture stabilization,9 byfacilitatingcentralcompensationof
sen-sory loss, whether partial or complete.10 Currently, VRis
supported by newman---machine interfaces(MMIs). These
interfaces provide stimuli that replace missing natural information,enablingthecreationofalternativepathways thatact inmaintaining balance.11 Thus,MMIs arenothing
morethan alternative stimuli that act on the facilitation of SS. There are descriptions of the additionalbeneficial effects of neurofeedback in the recovery of body bal-ancewithelectrotactilestimuliappliedtothetongue,12,13
auditory biofeedback,14,15 and audiovisual biofeedback.16
However, Basta and Ernst17 believe in the effectiveness
of using vibrotactile biofeedback; with this, the subject is not deprived of the natural perception of sound and visualstimulifromtheenvironment.Studieshaveshownthe effectivenessofvibrotactilebiofeedbackequipmentapplied on the lateral aspect of the trunk, with increased pos-tural stability18 and improved alignment of the center of
mass.19
In a controlled double-blinded pilot study, 36 patients dividedintofivegroupswithvestibulardisordersofdifferent etiologies showed significant reduction in body oscilla-tionaftertrainingwiththeVertiguardTMdevice.20 Another
SensoryOrganization Test(SOT) protocolof Computerized DynamicPosturography(CDP).21
Theaimofthisstudywastoevaluatetheeffectivenessof vibrotactileneurofeedback(VertiguardTM)asasensory
sub-stitutein patients whodidnot obtaina goodresponse to conventionalVR.
Methods
ThisstudywasapprovedunderNo.0896/09bythe Institu-tionalEthicsCommittee.Allparticipantssignedaninformed consentpriortotheirinclusioninthestudy.Theyarepartof theinitialsample,15subjectswithvestibulardisorderswho didnot achievesatisfactory results afterfollowing a con-ventionalprotocolofvestibularrehabilitation.Neurological and/ororthopediclimitationsthatpreventedtherealization ofCDPortrainingwiththeVertiguardTMwereconsideredas
exclusioncriteria.Thesubjectswererandomlyassignedto astudygroup(SG)(whoreceivedthevibrationduring train-ing)andacontrolgroup(CG)(whotrainedwiththepower off).Thesametherapistperformedalltraining;ordersand directionswereexactlythesameforbothgroups.
Patients included in the study followed a protocol of anamnesis, otorhinolaryngological examination, static (Romberg) and dynamic (Fukuda) stability tests, coordi-nation tests, audiometry, acoustic impedance, electro-oculographywithcaloricstimulationusingwater (at 44◦C
and30◦C;andat18◦Cwhentherewerenoresponsestothe
foregoingtemperatures),andtheSOTprotocol oftheCDP (EquitestNeuroComTM).22
Next,thesubjectsansweredtheBrazilianversionoftwo assessment questionnaires, the Dizziness Handicap Inven-tory(DHI)23 and theActivities-specificBalance Confidence
(ABC)Scale.24,25
TheDHIassessesandquantifiestheimpactofdizziness onqualityof life of the patient.It consists of three sep-arate assessments distributed among 25 questions; seven assessphysicalaspects(worseningofdizzinessasaresultof movementsoractions);nineconsiderthefunctionalaspects (limitationofactivitiesofdailylivingbydizziness);thefinal ninequestionsassesstheemotional aspects(lossofsocial lifeorfeelingsofinsecurity,fear,depressioncausedby dizzi-ness).The patientmustrespondtoall25 questions,using ‘yes’, which corresponds to4 points; ‘sometimes’, which correspondsto2points,or‘no’,whichcorrespondstozero points.Therefore,thehigherthescore,theworsethe qual-ityoflife.
The ABC scale quantifies the self-perception level of bodybalancedisorders andhelpsin selectingappropriate
Figure1 VertiguardTMcoupledtothepatient’swaist.
interventions. The patientquantifies(inpercentage,from zeroto100%)his/herself-confidenceinperforming16tasks of daily living.Therefore, thehigher thepercentage, the higherhis/herself-confidence.
After evaluation, patients were trained with VertiguardTM. The device has body balance assessment
and training functions. It consists of an adjustable belt placed around the patient’s waist (Fig. 1) containing a main unit fitted with two gyroscopes, which detect the direction of the body oscillation (anterior/posterior, R/L side),andfourvibrating stimulatorsarrangedat anglesof 90◦ between them (Fig.2). These vibrating units respond
to the command of the main unit to produce vibration, signalingthedirectionofbodydisplacement.
Theassessmentaimstoquantify,accordingtoan estab-lishednormalstandard,thebodymovementsofthesubject whenperformingvariousstaticanddynamictasks,namely: patientstandingwitheyesopenandclosed; supportedon one footwitheyes open; supported ononeleg witheyes closed (only for patients younger than 60 years); march-ingeightsteps,touchingtheheelwiththebigtoe(tandem gait); standingwithopen andclosed eyes ona foam sur-face;supportedononefootwitheyesopen;marchingeight steps,touchingtheheeltothebigtoe(tandemgait)ona foamsurface;walking3m;walking3mperformingcircular movementsof thehead; walking3m movinghead upand down;walking3mwithclosedeyes;skippingasequenceof sixobstacles;andsittingdownandstandingupfromachair (forsubjectsover60years).Whenusedinthetrainingmode, the main unit selects and stores the six worst responses obtained in the previous evaluation, tobetrained over a period of ten days,according to the protocol established when the equipment was developed at the University of
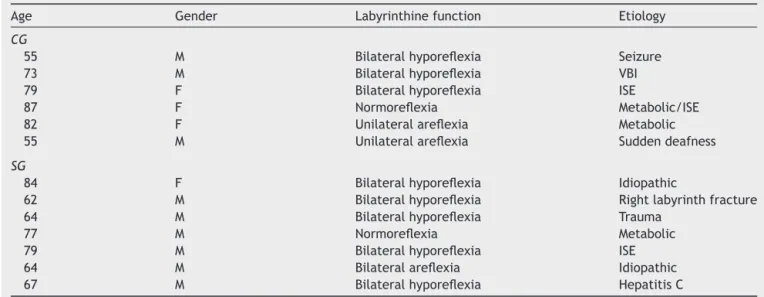
Table1 PresentationofCGandSGaccordingtoage,gender,vestibularfunction,andetiologyofbodyimbalance. Age Gender Labyrinthinefunction Etiology
CG
55 M Bilateralhyporeflexia Seizure 73 M Bilateralhyporeflexia VBI 79 F Bilateralhyporeflexia ISE
87 F Normoreflexia Metabolic/ISE 82 F Unilateralareflexia Metabolic 55 M Unilateralareflexia Suddendeafness
SG
84 F Bilateralhyporeflexia Idiopathic
62 M Bilateralhyporeflexia Rightlabyrinthfracture 64 M Bilateralhyporeflexia Trauma
77 M Normoreflexia Metabolic 79 M Bilateralhyporeflexia ISE 64 M Bilateralareflexia Idiopathic 67 M Bilateralhyporeflexia HepatitisC
CG,controlgroup;SG,studygroup;VBI,vertebral-basilarinsufficiency;ISE,imbalancesyndromeoftheelderly;TBI,traumaticbrain injury.Areflexiawasconsideredastheabsenceofpost-caloricresponses;hyporeflexiaasangularvelocities<4◦/s.
Table2 MeanvaluesforC5andC6beforeandaftertrainingintheCGandSG.
Group C5pre- C5post- p C6pre- C6post- p
CG 34.83 48.88 0.098 43.33 54.05 0.165 SG 26.85 53.23 0.007a 15.85 41.19 0.012a
CG,controlgroup;SG,studygroup.
a Statisticalsignificance.
Berlin.Whileperformingtheselectedtasks,ifany inappro-priatebodydeviationoccurs,thestimulatorsemitvibratory signals indicating to the subject the direction of his/her movement. Thus, the equipment helps in the perception of inappropriatemovements, replacingthelost vestibular information.
The clinicaleffectofthetreatmentwasdeterminedby acomparisonbetweentheresultsofevaluationsperformed beforeandafterthetreatmentwiththeconditions5and6 oftheSOTprotocol oftheCDP---conditionstypically con-sidered as vestibular. The responses of the twoscales of assessmentwerealsocompared,inordertodeterminethe self-perception of the patient regarding his/her improve-ment.
The difference between the posturographic values obtainedbeforeandaftertreatment,consideringthatthey followanormaldistribution,wasdeterminedbypaired Stu-dent’st-test andconsidered significantwhen p<0.05.For DHIand ABCscales, theKruskal---Wallistest was used--- a particularlysuitabletest,becauseofthesmallsamples.
Results
Fifteensubjectsagreedtoparticipateinthestudy(tenmen andfivewomen,age71.3±10.8years).Duringthetraining process,twopatientscouldnotcompletetheprotocoldue tohealthissues,reducingthefinalsampleto13individuals, sevenintheSGandsixinthe CG.Table1showsthe age,
gender,vestibularfunction,andetiologyofthesubjectsin thesample.
ThevaluesobtainedinposturographyconditionsC5and C6andontheABCandDHIscales inthebeginning ofthe experiment showed nostatistical difference between the CGandSG,characterizingtheseashomogenousgroups.
Between pre- and post-treatment means, a significant differencefor C5 (p=0.007)and C6 (p=0.012) wasfound onlyintheSG.Thepre-andpost-treatmentoftheC5and C6areshowninTable2.
Among the responses to DHI questionnaire before and after treatment, a significant difference in the physi-cal aspect in the CG (p=0.0400) and the SG (p=0.0423) was observed; and in functional aspect, only in the SG (p=0.0427).TheresultsfoundareshowninTable3.
Theresults forABCscaledemonstratea significant dif-ferencebetweenthebeginningandendofthetreatmentin theSG(p=0.04)butnotintheCG(p=0.12).Thenumerical valuesareshowninTable4.
Discussion
The results of this study suggest that VertiguardTM
Table3 NumericalvaluesofmeansobtainedontheDizzinessHandicapInventory(DHI)scalebeforeandaftertrainingbythe CGandSG.
DHI Pre-physical Post-physical p Pre-functional Post-functional p Pre-emotional Post-emotional p
CG 17.66 10.33 0.04a 19.33 14.33 0.09 15.66 10.66 0.21
SG 13.71 5.42 0.04a 18.85 7.71 0.04a 15.71 7.71 0.14
CG,controlgroup;SG,studygroup.
aStatisticalsignificance.
Table 4 Percent values of means obtained on the Activities-specificBalanceConfidence(ABC)scalebeforeand aftertrainingbyCGandSG.
ABC Pre- Post- p
Controlgroup 58.84 69.68 0.12 Studygroup 68.66 88.03 0.04a
CG,controlgroup;SG,studygroup.
aStatisticalsignificance.
limitedinthesecases,andothermethodsthatseeksensory substitutionhavebeenstudied.
The present sample was composed of elderly individ-uals(meanage71.3years)whoclearlyhadseverepostural impairment, which represents the reason they did not achieve improvement with conventional VR. It can be observedthat, evenwithlargernumbers ofsubjects with bilaterallycompromisedlabyrinthinefunction,onlySG sub-jects,whoreceivedthevibrotactilestimulation,showeda statistically significant improvement in conditions C5 and C6. This result suggests that the additional vibrotactile stimuluswasabletostabilizethepostureunderthose chal-lengingconditionsencounteredduringtraining.
Conditions C5 and C6 of the SOT protocol of the CDP arecalledvestibularconditionsbecause,onunstableground withabsent(C5)orconflicting(C6)vision,postural mainte-nancedepends exclusively onvestibularinformation. The commitment tothis information causes exaggerated pos-turaloscillation,orfalls.Theimprovementachievedbythe grouptreatedwithvibration(SG)suggeststhattheCNSused theadditionalstimulustointegrateextrainformationand improveitsposturalrecoverystrategies.
Addressingassessmentscales,improvementofthe func-tionalaspect of DHI wasnotedin the group treated with vibrationduringtraining.This resultimpliesthat onlythe subjectsinthetreatedgroupshowedareductionof inter-ferencefrom theirdizzinessin their dailytasks afterthis therapeutic approach, demonstrating theeffectiveness of thetrainingassociated withsensorysubstitution. Patients feltsaferinperformingtheiractivitiesdespitetheir phys-icallimitations.Withregardtothephysical aspectofDHI, it is useful to note that both the SGand the CG showed improvementoftheirindicesaftertheintervention.These resultscanbeexplainedbytheintensivephysicalexercise performed during the period by subjects previously suf-fering restrictiondue to theirlimitation of movement. In contrast,neithergroupachievedchangesintheemotional aspectbetween pre- andpost-training phases. Therefore, therewasnodifferenceintheemotionalimpactcausedby dizzinessintheirlifeaftertheintervention.
Thelevelofself-confidence,measuredbytheABC ques-tionnaire,improvedsignificantlyonlyinthegroupreceiving the vibrotactilestimulus.Again, theseresults suggest the beneficialimpactofvibrotactilestimulationassociatedwith vestibular rehabilitation in the recovery of cases with severelyimpairedposturalcontrol.
Conclusion
Thiswasapreliminarystudy,conductedwithasmallnumber of patients, butit already hasshown unquestionably that vibrotactile biofeedback, asa sensory substitution to the vestibularsystem, is auseful toolin patients with limita-tionsintheirposturalrecoverywithconventionalvestibular rehabilitationprotocols.
Funding
ThisstudywasfundedbyaCAPESresearchgrantfromJuly 2011toJune2013.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.BalohR,HonrubiaV.Vestibularfunction:anoverview.In: Clin-icalneurophysiologyofthevestibularsystem.3rded.Oxford: UniversityPress;2001.p.17---20.
2.DuffauH.Brainplasticity:frompathophysiologicalmechanisms totherapeuticapplications.JClinNeurosci.2006;13:885---97. 3.HorakF.Posturalcompensationforvestibularloss.RestorNeurol
Neurosci.2010;28:57---68.
4.TelianS,ShepardN.Updateonvestibularrehabilitationtherapy. OtolaryngolClinNorthAm.1996;29:359---71.
5.BittarR,PedaliniM,FormigoniG.Porqueareabilitac¸ão vesti-bularfalha.InterArchOtorhinolayngol.2000;1:118---22. 6.Ekvall-Hansson E. Vestibular rehabilitation. In: Stone JH,
BlouinM,editors.Internationalencyclopediaofrehabilitation. 2013.Availablefrom:http://cirrie.buffalo.edu/encyclopedia/ en/article/278/
7.PulaskiPD,ZeeMD,RoinsonDA.Thebehaviorofthe vestibule-ocular reflex at high velocity head rotation. Brain Res. 1981;15:9---61.
8.RestakR. Seucérebronuncaenvelhece:descubracomovocê podedesenvolvertodoo seupotencial.3a Edic¸ãoSão Paulo:
EditoraGente;2006.p.2003.Títulooriginal:‘‘TheNewBrain: howthemodernageisrewiringyourmind’’.
reducingswayinbilateralvestibularlosspatients.GaitPosture. 2010;31:213---7.
10.Bach-y-Rita, Kercel. Sensory substitution and the human---machineinterface.TrendsCognSci.2003;7:541---6. 11.WangW,CollingerJL,PerezMA,Tyler-KabaraEC,CohenLG,
Bir-baumerN,etal.Neuralinterfacetechnologyforrehabilitation: exploitingandpromotingneuroplasticity.PhysMedRehabilClin NAm.2010;21:157---78.
12.DanilovY,TylerM,SkinnerK,HogleR,Bach-y-Rita.Efficacyof electrotactilevestibularsubstitutioninpatientswithperipheral andcentralvestibularloss.JVestibRes.2007;17:119---30. 13.BarrosC,BittarR,BottinoM.Recuperac¸ãodoequilíbrio
cor-poralnaarreflexia vestibularbilateralpormeio dainterface homem-máquina (IHM): estudo preliminar. Arq Int Otorrino-laringol.2007;11:278---83.
14.DozzaM, Chiari L, Chan B, RocchiL, Horak FB, CappelloA. Influenceofaportableaudio-biofeedbackdeviceonstructural propertiesofposturalsway.JNeuroengRehabil.2005;31:2---13. 15.DozzaM,HorakFB,ChiariL.Auditorybiofeedbacksubstitutes forlossofsensoryinformationinmaintainingstance.ExpBrain Res.2007;178:37---48.
16.MirelmanA,HermanT,NicolaiS,ZijlstraA,ZijlstraW,Becker C, et al. Audio-biofeedback training for posture and bal-anceinpatientswithParkinson’sdisease.JNeuroengRehabil. 2011;8:35.
17.BastaD,ErnstA.Modernrehabilitationforvestibulardisorders usingneurofeedbacktrainingprocedures.HNO.2008;56:990---5.
18.DozzaM,ConradW,PeterkaR,ChiariL,HorakF.Effectsof prac-ticingtandemgaitwithandwithoutvibrotactilebiofeedbackin subjectswithUVL.JVestibRes.2007;17:195---204.
19.Horak F, Dozza M, Peterka R, Chiari L, Wall C. Vibrotactile biofeedbackimprovestandemgaitinpatientswithunilateral vestibularloss.NYAcadSci.2009;1164:279---81.
20.BastaD,ErnstA.Vibrotactileneurofeedbacktrainingwiththe Vertiguard®-RT-system. A placebo-controlled double-blinded
pilot study on vestibular rehabilitation. HNO. 2011;59: 1005---11.
21.BastaD,Rossi-IzquierdoM,Soto-VarelaA, GretersME, Bittar RS, Steinhagen-Thiessen E, et al. Efficacy of a vibrotac-tile neurofeedback training in stance and gait conditions for the treatment of balance deficits: a double-blind, placebo-controlledmulticenterstudy.OtolNeurotol.2011;32: 1492---9.
22.FurmanJ.Roleofposturographyinthemanagementof vesti-bularpatients.OtolaryngolHeadNeckSurg.1995;112:8---15. 23.CastroA,GazzolaJ,NatourJ,Gananc¸aF.DHIDizziness
Hand-icap Inventory: versão brasileira. Pró-Fono R Atual Cient. 2007;19:97---104.
24.PowellE,MyersA.TheActivities-specificBalanceConfidence (ABC)Scale.JGerontolABiolSciMedSci.1995;50:28---34. 25.Marques A, Mendes Y, Assumpc¸ão A, Pereira C, Taddei U.