w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Biofeedback
therapy
combined
with
diet
to
treating
ODS
(Anismus):
2
years
outcome
Fakhryalsadat
Anaraki
a,
Tahereh
Foroughifar
b,∗,
Reza
Bagherzadeh
Saba
c,
Elaheh
Miri
Ashtiani
d,
Zinat
Ghanbari
baShahidBeheshtiUniversityofMedicalScience,TaleghaniHospital,DepartmentofSurgery,Tehran,Iran
bTehranUniversityofMedicalSciences,ImamKhomeiniHospitalComplex,DepartmentofPelvicFloor,Tehran,Iran cIranUniversityofMedicalSciences,Rasool-e-AkramHospital,DepartmentofSurgery,Tehran,Iran
dShahidBeheshtiUniversityofMedicalSciences,DepartmentofRehabilitationSciences,Tehran,Iran
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30October2016 Accepted21December2016 Availableonline2February2017
Keywords:
Obstructeddefecationsyndrome Anismus
Biofeedbacktherapy Diet
a
b
s
t
r
a
c
t
Object:Theadvantagesofbiofeedbacktherapyalongwithdietinpatientswith constipa-tionareamongtheissuesdiscussednowadays.Theaimofthisstudywastoevaluate2 yearsoutcomeofbiofeedbacktherapyalongwithdietinpatientswithobstructeddefecation syndrome(ODS)(Anismus).
Methodology:Thefocusofthisprospectivestudyisagroupof129patientswithODS consti-pation,whowerereferredtotwotertiary-carereferralacademiccentersfrom2013to2016. Patientsreceivedbiofeedbacktherapycombinedwithappropriatedietincasesgroupand receiveddietincontrolsgroup.Goodresponsewasdefinedasasubjectwithatleast50 percentimprovementfrombeforetoafterbiofeedbacktherapyonaClevelandClinicFlorida ConstipationScoringSystem(CCF).Factorsassociatedwithbetteroutcomewereanalyzed usingSPSS20software.
Results:Outofthe129patients,112patients(86.8%)werefemale.Themeanageofpatients was42.44±15.05years.ThemeanCCFscoreofthepatientsbeforeandafterbiofeedback therapywas12.41±4.39and6.00±3.28respectivelyincasegroup(p-value<0.001).In addi-tion,themeanCCFscoreofthepatientsbeforeandafterdiettherapywas12.82±4.85and 9.43±3.79respectivelyincontrolgroup(p-value<0.001).WhileCCFscoreinbothcaseand controlgroupsreducedsignificantlyaftertherapy,therateofthisreductionwashigherin casegroup(p<0.001).
Conclusion: Ourfindingssuggestthatbiofeedbacktherapycombinedwithdietwillimprove patientsoutcomeinODSconstipation.Prospectiveclinicaltrialswithlargersamplesizes arerecommendallowingforcausalcorrelations.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](T.Foroughifar).
http://dx.doi.org/10.1016/j.jcol.2016.12.004
Terapia
por
biofeedback
combinada
com
dieta
no
tratamento
da
SDO
(Anismus):
desfecho
de
2
anos
Palavras-chave:
Síndromedadefecac¸ãoobstruída Anismus
Terapiaporbiofeedback Dieta
r
e
s
u
m
o
Objetivo: Asvantagensdaterapiaporbiofeedback,juntamentecomadieta,empacientes comconstipac¸ãosesituam entreostópicosatualmenteemdiscussão. Oobjetvodesse estudofoiavaliarosresultados,após2anos,daterapiaporbiofeedbackassociadaàdieta empacientescomsíndromedadefecac¸ãoobstruída(SDO)(Anismus).
Metodologia: O enfoque desse estudo prospectivo é um grupo de 129 pacientes com constipac¸ãoporSDO,encaminhadosadoiscentrosacadêmicosdereferênciapara atendi-mentoterciárioentreosanosde2013e2016.Ospacientesreceberamterapiaporbiofeedback emcombinac¸ãocomdietaapropriadanogrupodeestudo(casos),eapenasdietanogrupo decontrole.Boarespostafoideinidacomoopacientecompelomenos50%demelhora desdeantesatéapósaterapiaporbiofeedback,comousodeumSistemadePontuac¸ão paraConstipac¸ãodoCentroMédicoClevelandClinicFlorida(CCF).Osfatoresassociadosa melhordesfechoforamanalisadoscomousodoprogramaSPSS20.
Resultados: Dos129pacientes,112(86,8%)erammulheres.Amédiadeidadedospacientes erade4244±15,05years.OescoreCCFmédiodospacientesantesedepoisdaterapiapor biofeedbackfoi12,41±4,39e6,00±3,28respectivamentenogrupodecasos(P<0,001).Além disso,oescoreCCFmédiodospacientesantesedepoisdadietoterapiafoi12,82±4,85e 9,43±3,79respectivamentenogrupodecontrole(P<0,001).EmboraoescoreCCFtantono grupodecasoscomonogrupodecontroletenhaapresentadoreduc¸ãosignificativaapósa terapia,ograudessareduc¸ãofoimaiselevadonogrupodecasos(P<0,001).
Conclusão: Nossosachadossugeremqueaterapiaporbiofeedbackemcombinac¸ãocoma dietamelhoraoresultadoparaospacientesapresentandoconstipac¸ãoporSDO. Recomen-damosarealizac¸ãodeestudosclínicosprospectivoscomamostrasmaisexpressivas,que permitamoestabelecimentodecorrelac¸õescausais.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Constipation is one of the most common digestive prob-lems and it is associatedwith muchcost forits diagnosis andtreatment.1–3 Itiscategorizedinprimaryandsecondary
forms.4Primaryformsofconstipationoccurdueto(1)slow
colonictransit,(2)obstructeddefecationsyndrome,(3)items includedbothslowtransitandODS,and(4)irritablebowel syn-dromeconstipation.Secondaryformsofconstipationoccur duetoperipheralneurogeniccausessuchasdiabetesor auto-nomicneuropathy,centralneurogeniccausessuchasmultiple sclerosis,spinalcordinjuriesandParkinson,non-neurological causes such as hypokalemia, hypercalcemia, pregnancy, and anorexia, and eventually medical causes suchas opi-oid,hypertensiontreatmentdrugs,tricyclicantidepressants, etc.
Amongtheprimarycausesofconstipation,thereis dys-functioninmusclesresponsiblefordisposalandanatomical abnormalities of pelvic organs in ODS, so defecation will be difficult.5 ODS isthe cause of one-third of all cases of
constipation.5Inthissyndrome,thenaturalfeelingofneedto
defecateoccurswiththeinabilitytodefecateintherequired time.ODSoccurseitherduetofunctionalcausessuchas para-doxicalcontractionsofpelvicfloormusclesandinsufficient contractionofmusclesduringthedefecationoranatomical
causessuchasrectocele,intussusception,mucosaprolapse, andperinealdescending.
ThemainfunctionalreasonproposedforODSisanismus. Anismusincludesabout15–50percentofcasesofchronic con-stipationbasedondiagnosticcriteria.6Someoftheanismus
symptoms include excessive straining, incomplete defeca-tion, difficult and incomplete defecation with great time intervals.7
Oneofthesimplediagnosticwaysinevaluationofpatients withconstipationisdigitalrectalexamination.Indigital rec-tal examination,the perineal feeling, anocutaneous reflex, reflexcontractionsoftheexternalanalsphincterare exam-ined. Looseness,spasm,tenderness,mass,blood,andstool intherectumaredetermined.Sphinctertoneand puborec-talinrestandsqueezeareexamined.Inthestrainingstate, therelaxationoftheexternalsphinctermuscleor puborec-talalongwithperinealdescentisexamined.Indigitalrectal examination, sensitivity and specialty to diagnose dyssyn-ergyhavebeenreported87%and75%,respectively.8Oneof
coordinaterectal,analsphincteranal,andabdominalmuscles forcompletedefecationandtogetbettersensoryperception inpatients with reduced rectal sensation. In recent years, studies havefoundthat biofeedback ispreferred overdiet, exercise,laxatives,polyethyleneglycol,diazepam,and treat-mentbyballoondisposal.10–13 Itisnotalsofollowedbybad
sideeffects.
Themainobjectiveofthisstudyistoinvestigatethe short-termeffectsofbiofeedbacktherapycombinedwithdietinthe treatmentofdyssynergicdysfunctioninpelvicfloormuscles asacommoncauseofconstipation.
Methodology
Thisstudywasconductedusingprospectivemethod.Inthis study,129patients(men and women)referredtoclinicsof TehranandShahidBeheshtiUniversity ofMedicalSciences duetoconstipation(accordingtoRomeIIIcriteria)between theyears2013to2016wereselected,andtheywere followed-upfortwoyears.Afterobtainingcarefulhistoryandphysical examinationsuchasdigitalrectalexam,theywereincluded in the study by diagnosing paradox contractions of pelvic floormusclesasthemaincauseofconstipation.Oneofthe measurestaken beforeand aftertreatment was anal EMG assessment.Theethicalconsentformtoparticipateinthe studywastakenfrompatients.
Demographicdataincludingage,gender,weight,and edu-cation, history of pregnancy in women, type and number of childbirth were asked from patients. Chief complaint, symptomssuchasabdominalpainorrectalbleedingduring defecation,previoushysterectomysurgery,andanyurinaryor analprevioussurgerywereasked.
Inpelvicexamination,perinealdescending,fissure, hem-orrhoids, sphincter tone examination by digital rectal examination, Rectocele, enterocele, and priniocele, pro-lapse of rectal mucosa and intussusceptions of mucosa weretaken intoconsideration.Puborectaland anal sphinc-ter muscle status was examined using digital rectal examination.
Inthedigitalexamination,weexaminedthecontracting power in which patient contracted his abdominal, gluteal musclesandpelvicfloorwithhisallpower(aroundthe exam-iner’sfinger).Then,weexaminedtheendurancecontraction inwhichthepatientwasaskedtomaintainhispelvicfloor statusfor 10s. Werecorded the duration inwhich patient could maintainhis contraction,which it could last from 1 to10s. This number should approachto10 gradually dur-ing the biofeedback treatment. In examining and treating patientswith biofeedback,afterputtingthe probe into the rectum, restingpressure,strength,squeezeamplitude,and restingamplitudeofpelvicfloormusclesweremeasured.All oftheaboveexaminationswerealsoconductedattheendof biofeedbacktreatment.
Inaddition,constipationscorewasassessedbyCleveland ClinicConstipationScoringSystemQuestionnaire,whichits validity and reliability were already evaluated by Agachan etal.14 Accordingtothisquestionnaire,theminimumscore
iszeroandthemaximumscoreis30.
Inclusionandexclusioncriteriaofstudy
Inclusioncriteriaincludedadiagnosisofconstipationdueto pelvicfloormuscledisorders(ODS)basedonacarefulhistory anddigitalrectalexamination.
Exclusion criteriaofstudy includedinflammatorybowel disease,aninfectionwithHIV,neurologicaldisorders, urinary-stress incontinence requiring surgery, urgent incontinence requiringsurgery,andfecalincontinenceaswellaspatients who donotperceivebiofeedback andpatientswho arenot willing toparticipateinthestudy.Patientsalsounderwent colonoscopytoruleoutothercausesofconstipationandto ruleoutintestinaltumorsandmalignancies,andcolonicslow transit,whichallofthemwerenormal.Finally,patientswho werefollowed-upforlessthan2yearswereexcludedfromthe study.
Finally, patients selectedbasedon the examinationand questionnaire were considered candidate for biofeedback treatmentanddiet,whichoutof129patients,80ofthemwere accepted(biofeedbackcombinedwithdiet).Accordingly,49of themwere treatedthroughonlybydietduetovarious rea-sonssuchinabilitytopaybiofeedbackcosts,lackofaccessto skilledphysicaltherapist,longdistancefromhealthcenters, etc.Accordingly,patientsweredividedintotwogroups:case group (biofeedback combined with diet) and control group (onlydiet).
Diet
Inallcaseandcontrolpatients,observingspecificdietbased on the following protocol was taught to patients and all patientsobservedthisdiet:
• Taking10-8glassesoffluidsdaily(excepttea)atmeals inter-vals
• Takingdairyproductsexceptyogurt
• Usinggroundwheatbranwithmilk
• Usingvegetablesandfruits(especiallyplums,grapes,figs, kiwi)
• Reducedusedofapplesandbananas
• Reduceduseofstarchyfoods(rice–potato–pasta)
• Moderateduseofmedicationsthatcauseconstipation
• Takingpsyllium
Biofeedbackperformedthroughthisprotocol15,16
a) Open the software program and enter pertinent patient data.ConfigureacontinuousprogramwiththeEMG sen-sitivitybasedonthepatient’smuscletestinggrade. b) Usinganinternalelectrode,providepatientwithprivacyto
selfinsertorassistasneeded.Lubricantwasmade avail-able.
c) EstablishingarestingbaselineofEMGactivityforlast2min. d) Askthepatienttoperformseveralcontractionsand relax-ationsofthepelvicfloormusclesinconjunctionwiththe movementonthevisualdisplay.
f) Configureabaselinetestsessioninawork/restmodewith work times manual muscle testing endurance score in secondsandresttimesequals10suseaprotocolof10total contractions.
g) Printandfileasessionsummaryreport,includingdatasuch asmaximumandminimumEMGmuscleactivityin micro-volts,andvisualdisplayoftotaltestingsession.
h) Removeinternalelectrode.
i) Cleanallelectrodesandcablesaccordingtoclinicalsetting policy.
Weperformedbiofeedbackusinganinternalelectrodein theanalandsurfaceelectrodewhichislocatedonthethigh’s externalsurface.
Results
Patientcharacteristics
Inthisstudy,129patientsincluding112females(86.8%)and 17males(13.2%)werestudied.Themeanageofpatientsin thisstudywas42.44±15.05attheagerangeof15–78years.
ThemeanBMIofthepatientsinthisstudywas25.63±3.78. Outof129patients,61patients(47.3%)hadacademic educa-tion,62patients(48.1%)hadeducationuptohighschool,and sixpatients(4.7%)wereilliterate.
Outof129patients,80patientswereincludedinthecase groupbasedoninclusionandexclusioncriteriaofstudy.They receivedbiofeedbackalongwithdiet.Inaddition,49patients wereincludedinthecontrolgroup,whoreceivedonlydiet.
Thechiefcomplaintofpatientswasrespectivelydifficult defecationin54patients(41.9%),painin45patients(34.9%), bleeding in 12 patients (9.3%), incontinency in 10 patients (7.8%),andmassin8patients(6.2%).
Outof80patientsinthecasegroup,28 patients(35.0%) hadthehistoryofdiseaseassociatedwithconstipationinthe past.Additionally,35patients(43.8%)hadahistoryofdoing anorectalsurgery.Outof80patientincasegroup,20patients (25.0%)had ahistoryoftakingdrugrelatedtotreatmentof constipationorinducedconstipationinthepast.
Outof112womenparticipatedinthestudy,56patients (50.0%)hadthehistoryofNVDand34patients(30.3%)hada historyofcesareansection(Table1).
SignificantdifferencewasnotfoundbetweentheCCFscore beforetreatmentamongwomen(meanCCFscore=12.60)and men(meanCCFscore=12.35)(p=0.837).
Pretreatmentversuspost-treatment;EMG
All components of the muscles and anal sphincter tone includingstrength,squeezeamplitude,restingamplitudeand endurancecontractionimprovedafter11.39±4.38sessionsof biofeedbackamongthe80patientsingroupcase(Table2).
Pretreatmentversuspost-treatment;physicalexam
Beforetreatment,outof80patientsinthecasegroupinDigital RectalExamination(DRE),39patients(48.8%)hadabnormal restingpressure,16 patients(20.0%)hadabnormalsqueeze
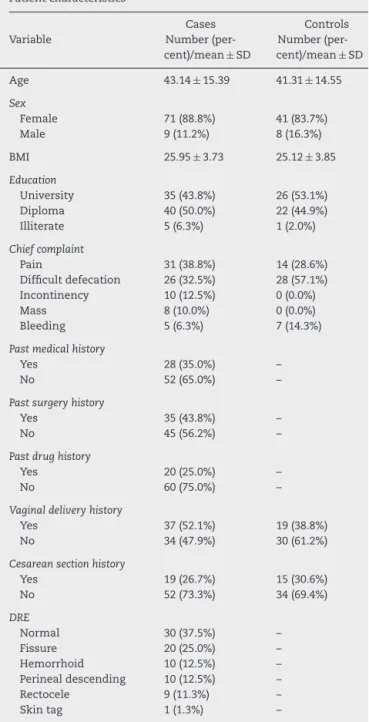
Table1–Demographicinformationandgeneral
characteristicsofpatientsincaseandcontrolgroups.
Patientcharacteristics
Cases Controls Variable Number
(per-cent)/mean±SD
Number (per-cent)/mean±SD Age 43.14±15.39 41.31±14.55
Sex
Female 71(88.8%) 41(83.7%) Male 9(11.2%) 8(16.3%)
BMI 25.95±3.73 25.12±3.85
Education
University 35(43.8%) 26(53.1%) Diploma 40(50.0%) 22(44.9%) Illiterate 5(6.3%) 1(2.0%)
Chiefcomplaint
Pain 31(38.8%) 14(28.6%) Difficultdefecation 26(32.5%) 28(57.1%) Incontinency 10(12.5%) 0(0.0%) Mass 8(10.0%) 0(0.0%) Bleeding 5(6.3%) 7(14.3%)
Pastmedicalhistory
Yes 28(35.0%) –
No 52(65.0%) –
Pastsurgeryhistory
Yes 35(43.8%) –
No 45(56.2%) –
Pastdrughistory
Yes 20(25.0%) –
No 60(75.0%) –
Vaginaldeliveryhistory
Yes 37(52.1%) 19(38.8%) No 34(47.9%) 30(61.2%)
Cesareansectionhistory
Yes 19(26.7%) 15(30.6%) No 52(73.3%) 34(69.4%)
DRE
Normal 30(37.5%) – Fissure 20(25.0%) – Hemorrhoid 10(12.5%) – Perinealdescending 10(12.5%) – Rectocele 9(11.3%) – Skintag 1(1.3%) –
pressure, and 76 patients (95.0%) had abnormal paradoxi-cal contraction,which it became significantlynormalafter biofeedbackexaminationofpatients(p<0.001)(Table2).
Inaddition,outof80patientsinthecasegroupinDRE,the mostcommonfindingsinpatientswere respectivelyfissure in20patients(25.0%),hemorrhoidin10patients(12.5%), peri-nealdescendingin10patients(12.5%),rectocelein9patients (11.3%)andskintagonlyin1patient(1.3%).However,physical examinationof30patients(37.5%)wasnormal.
Pretreatmentversuspost-treatment;symptoms
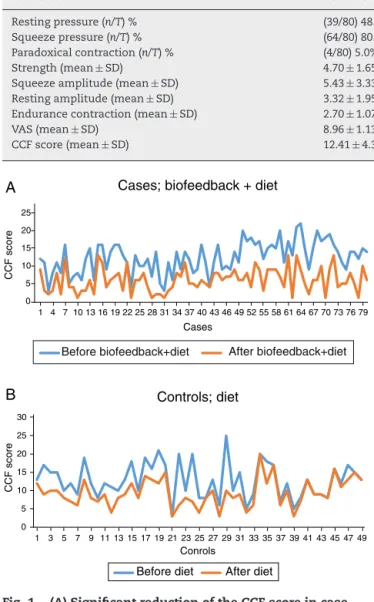
Table2–Biofeedbacktherapyalongwithdietincasegroupresultedinasignificantimprovementinallvariables
measuredinpatients.Inadditiontoinformationrelatedtopatients’electromyography,themeanVASandCCFScoreof
patientsimprovedsignificantlyafterbiofeedbacktherapyalongwithdiet(p<0.001).Effectsofbiofeedbackcombineddiet
therapyonDRE,EMG,VAS&CCFscoreinpatientswithODS.
Variables Pre-treatment Post-treatment p-Value
Restingpressure(n/T)% (39/80)48.8% (79/80)98.8% <0.001 Squeezepressure(n/T)% (64/80)80.0% (80/80)100% <0.001 Paradoxicalcontraction(n/T)% (4/80)5.0% (78/80)97.5% <0.001 Strength(mean±SD) 4.70±1.65 2.61±1.22 <0.001 Squeezeamplitude(mean±SD) 5.43±3.33 16.88±6.28 <0.001 Restingamplitude(mean±SD) 3.32±1.95 2.40±0.86 <0.001 Endurancecontraction(mean±SD) 2.70±1.07 6.09±1.00 <0.001
VAS(mean±SD) 8.96±1.13 3.84±1.99 <0.001
CCFscore(mean±SD) 12.41±4.39 6.00±3.28 <0.001
A
B
0 5 10 15 20 251 4 7 10 13 16 19 22 25 28 31 34 37 40 43 46 49 52 55 58 61 64 67 70 73 76 79
CCF score
Cases
Cases; biofeedback + diet
Before biofeedback+diet After biofeedback+diet
0 5 10 15 20 25 30
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49
CCF score
Conrols
Controls; diet
Before diet After diet
Fig.1–(A)SignificantreductionoftheCCFscoreincase grouppatientsafterbiofeedbackalongwithdiet(p<0.001); (B)significantreductionoftheCCFscoreincontrolgroup patientsafterthebiofeedbackalongwithdiet(p<0.001), whileinbothcaseandcontrolgroups,CCFscoreafter treatmentsignificantlyreduced,butrateofthisreductionis moreincasegroup(p<0.001).
3–22,whichitreducedafterthetreatmentto6.00±3.28atthe rangeof1–13(Table2).However,meanCCFscoreinthe con-trolgroupbeforetreatmentwas12.82±4.85attherangeof 3–25,whichitreducedto9.43±3.79attherangeof3–20after treatment(p<0.001).WhileCCFscoresignificantlydecreased aftertreatmentinbothcaseandcontrolgroups,therateof reductioninthecasegroupwassignificantlyhigher(p<0.001) (Fig.1).
The mean VAS score of case group before the start of biofeedbackwas8.96±1.13thatitbecame3.84±1.99afterthe treatment,whichwassignificantly(onaverage,about5points) reduced(p<0.001)(Table2).
Outof80patientsinthecasegroup,44patients(55.0%)had goodsatisfactoryresponse(over50%reductioninCCFscore) andtherestofthepatients(45.0%)hadnotenoughsatisfaction despiteimprovementinEMGcomponents.However,outof49 patientsincontrolgroup,onlyfourpatients(8.2%)hadgood satisfactoryresponseand45patients(91.8%)hadnotenough satisfactionwithresultsoftreatment(onlydiet).
Satisfactoryversusunsatisfactoryresponse
Significant differencewasnotfoundbetweenthemale and femalegenderintermsofsatisfactoryresponseafter treat-mentinthecasegroup(p=0.628),whilesignificantdifference wasfoundbetweenpatientsolderthan40yearsandpatients aged40andunder40yearsintermsofsatisfactoryresponse aftertreatmentincasegroup(p=0.010)(Table3).
Additionally,significantcorrelationwasfoundbetweenthe BMIofpatients and satisfactory response(p=0.05), so that patientswho hadaBMIlessthan25 hadabetterresponse totreatment,comparedwithpatientswhohadaBMIequalor 25orover25(Table3).
The relationship between ahistory ofC/S and the sat-isfactory response was also significant (p=0.004), so that patientswhohadnohistoryofC/Shadmuchmoresatisfactory responsecomparedtopatientswithahistoryofC/S(Table3). Additionally,outofpatientsincasegroupwhounderwent C/S,26.3%hadagoodoutcome,butoutofpatientswhowere undertheNVD,56.8%ofthemhadagoodoutcome.However,it couldbeconcludedthatpatientsunderwentNVDgavebetter responsetobiofeedbackalongwithdietcomparedtopatients underwentC/S.
Mean endurance contraction before treatment has sig-nificant correlation with satisfactory response of patients aftertreatmentwithbiofeedbackanddiet(p=0.002),sothat patientswhohadlowermeanendurancecontractionbefore treatmentprovidedmuchmoresatisfactoryresponseafterthe courseoftreatmentwithbiofeedbackalongwithdiet.
Finally,asignificantrelationshipwasfoundbetweenthe mean VAS score of patients before treatment and satis-factory response after treatment in case group (p=0.011). Thus, patients who had moreVAS score before treatment providedbettersatisfactoryresponsetotreatmentafterthe treatment.
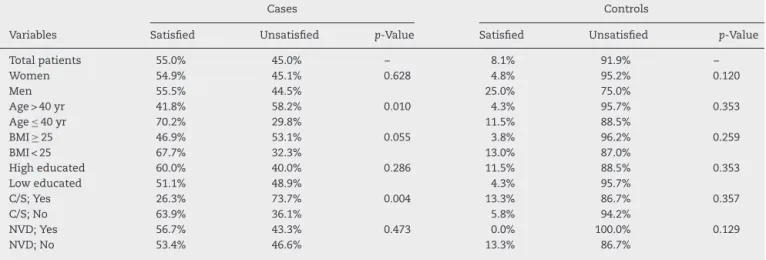
Table3–Inthecasegrouppatients40≥years,BMI<25yearsandfinallypatientswithoutcesareanhadmuchmore
satisfactionwiththanbiofeedbacktherapyalongwithdiet,whiletheserelationshipswerenotsignificantincontrol
group.Correlationsbetweensatisfactoryresponseandvariables:.
Cases Controls
Variables Satisfied Unsatisfied p-Value Satisfied Unsatisfied p-Value
Totalpatients 55.0% 45.0% – 8.1% 91.9% –
Women 54.9% 45.1% 0.628 4.8% 95.2% 0.120
Men 55.5% 44.5% 25.0% 75.0%
Age>40yr 41.8% 58.2% 0.010 4.3% 95.7% 0.353
Age≤40yr 70.2% 29.8% 11.5% 88.5%
BMI≥25 46.9% 53.1% 0.055 3.8% 96.2% 0.259
BMI<25 67.7% 32.3% 13.0% 87.0%
Higheducated 60.0% 40.0% 0.286 11.5% 88.5% 0.353
Loweducated 51.1% 48.9% 4.3% 95.7%
C/S;Yes 26.3% 73.7% 0.004 13.3% 86.7% 0.357
C/S;No 63.9% 36.1% 5.8% 94.2%
NVD;Yes 56.7% 43.3% 0.473 0.0% 100.0% 0.129
NVD;No 53.4% 46.6% 13.3% 86.7%
Multivariateanalysis
InthemultivariateanalysisbasedonCoxregressionmodel, variablesthathadsatisfactoryresponseofpatientsin single-variable analysis as well as variables that were seemingly correlated with satisfactory responseof patients including gender,age,BMI,VASbeforetreatmentandC/Shistorywere includedinmodel.Finally,itwasfoundthatage,C/Shistory andtheVASscorepriortoinitiationoftreatmentwere effec-tiveinprognosisofcasegrouppatients(p<0.05).
Discussion
Thisstudy proved thatbiofeedback therapy hassignificant impactinimprovementofpatientswithODS.Itbecameclear whenwefoundthatoutof80patientstreatedwith biofeed-back along with diet, 55.0 ofthem experiencedCCF score reductionover 50%afterthe courseoftreatment and they weresatisfiedwiththetreatment.However,outof49patients treated only with diet, 8.1% of them experienced relative improvement.
Theimpactoftreatmentwithbiofeedbackhasbeenproven invariousstudies.Inastudy conductedbyMuradRegadas et al. in 2016 on 116 patients with anismus to examine the impact of biofeedback along with diet on recovery of patients,itwasfoundthat59%ofpatientsweresatisfiedwith resultsofthetreatment.6Othersimilarstudiesconfirmthese
results.17–21FollowingimprovementinCCFscore,VASscore
ofpatientsalsoimprovedsignificantlyafterbiofeedbackand dietincasegroup,indicatingtheimpactofbiofeedbackonthe recoveryofpatients.
Inthisstudy,theeffectofbiofeedbackonEMG,muscletone, andpelvicsphincterswashigherthanitseffectonpatients’ satisfactionwithtreatment.ThismeansthatEMGindicesof pelvicmusclesofalmostallpatientsaftertreatmentimproved comparedtobeforetreatment.Manystudieshadfoundresults differentfromresultsofourstudy.Inthesestudies,despite clinical improvement of patients, significant improvement wasnotseeninEMGofpatientsafterbiofeedback.6,17,22–24
Inourstudy,despitethegeneralimprovementinresting pressure,squeezepressure,paradoxicalcontraction,strength, squeezeamplitude,restingamplitude,and endurance con-traction,satisfactoryresponseofpatientswasnotcomplete afterbiofeedbacktherapyalongwithdiet.Itmay bedueto otherreasons,exceptforpelvicmuscledysfunction,including anatomicdisorderssuchasRectocele,enterocele,andperineal descendingaswell asother primaryandsecondary causes ofconstipationsuchasneuropathiesandevenpsychological causes.
Themainweakness ofthisstudy was shortdurationof followupofpatients.Somestudieshavefollowed-upthe pos-itiveimpactofbiofeedbacklongtimesafterthetreatment(up to 5years after treatment),25–27 but the weakness of
stud-ies conductedin this regard is prolonged follow-up of the patients.
Inthis study,wecontinuethe follow-upofpatientsand wereleasethelong-termeffectofbiofeedbacktreatmenton patientswithODS,whilewecouldprovethepositiveimpact ofbiofeedbacktherapyunderthelightofcomparingthecase group with controlgroup inthis study.Another important pointinthisstudywastheimpactofpatients’ageonresponse tobiofeedbacktherapyalongwithdiet,sothatsignificant dif-ference wasfoundamongpatientsolderthan40years and 40 years old and youngerpatients interms of satisfactory responseafterthetreatmentinthecontrolgroup(p=0.010). Itwasfoundthat40yearsoldandyoungerpatientsprovided betterresponsetotreatmentcomparedtoolderthan40years patients.
This issue was not foundin our similar previous stud-ies.Itisduetobetterresponseofmusclesandsphinctersof youngpatientsreceivedbiofeedbacktherapyalongwithdiet comparedtomusclesandsphinctersofolderpeopleandthe direct impactofthe phenomenon ofaging inmuscle cells inresponsetotreatment.However,thebettercooperationof youngerpatients,especiallyduringEMGandeyeexamination, shouldnotbeoverlooked.
byMuradRegadasetal.in2009,significantdifferencewasnot foundbetweendistributionofpelvicdiseaseinwomenand typeofchildbirthamongthem.28
Otherdisadvantageofthisstudywaslackofstudyingand treatmentofpatientswithother typesofconstipation.Itis recommendedthatfurtherstudytobeconductedonpatients withothertypesofconstipation.
Conclusion
Thestudyshowedthatbiofeedbacktherapyalongwithdiet couldbeaneffectiveandacceptableoptionforpatientswith ODS,althoughitseemsthatmorestudiesarerequiredinthis area,especiallywithlargersamplesizesandlongerfollowup.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. SinghG,LingalaV,WangH,VadhavkarS,KahlerKH,MithalA, etal.Useofhealthcareresourcesandcostofcareforadults withconstipation.ClinGastroenterolHepatol.2007;5:1053–8.
2. StewartWF,LibermanJN,SandlerRS,WoodsMS,Stemhagen A,CheeE,etal.Epidemiologyofconstipation(EPOC)studyin theUnitedStates:relationofclinicalsubtypesto
sociodemographicfeatures.AmJGastroenterol. 1999;94:3530–40.
3. SethiS,MikamiS,LeClairJ,ParkR,JonesM,WadhwaV,etal. InpatientburdenofconstipationintheUnitedStates:an analysisofnationaltrendsintheUnitedStatesfrom1997to 2010.AmJGastroenterol.2014;109:250–6.
4. WaldA.Etiologyandevaluationofchronicconstipationin adults.UpToDate,Basow,DS(Ed).UpToDate,Waltham,MA.; 2008Oct1.
5. GreenbergR,ItahR,DekelR.Obstructeddefecation syndrome.Harefuah.2008;147:493–7.
6. Murad-RegadasSM,RegadasFS,BezerraCC,deOliveiraMT, RegadasFilhoFS,RodriguesLV,etal.Useofbiofeedback combinedwithdietfortreatmentofobstructeddefecation associatedwithparadoxicalpuborectaliscontraction (Anismus):predictivefactorsandshort-termoutcome. DiseasesColonRectum.2016;59:115–21.
7. PareP,FerrazziS,ThompsonWG,IrvineEJ,RanceL.An epidemiologicalsurveyofconstipationinCanada:definitions, rates,demographics,andpredictorsofhealthcareseeking. AmJGastroenterol.2001;96:3130–7.
8. TantiphlachivaK,RaoP,AttaluriA,RaoSS.Digitalrectal examinationisausefultoolforidentifyingpatientswith dyssynergia.ClinGastroenterolHepatol.2010;8:955–60.
9. RaoSS.Dyssynergicdefecationandbiofeedbacktherapy. GastroenterolClinicsNorthAm.2008;37:569–86.
10.ChiarioniG,SalandiniL,WhiteheadWE.Biofeedbackbenefits onlypatientswithoutletdysfunction,notpatientswith isolatedslowtransitconstipation.Gastroenterology. 2005;129:86–97.
11.RaoSS,SeatonK,MillerM,BrownK,NygaardI,StumboP, etal.Randomizedcontrolledtrialofbiofeedback,sham
feedback,andstandardtherapyfordyssynergicdefecation. ClinGastroenterolHepatol.2007;5:331–8.
12.HeymenS,ScarlettY,JonesK,RingelY,DrossmanD, WhiteheadWE.Randomized,controlledtrialshows biofeedbacktobesuperiortoalternativetreatmentsfor patientswithpelvicfloordyssynergia-typeconstipation. DiseasesColonRectum.2007;50:428–41.
13.KoutsomanisD,Lennard-JonesJE,KammMA.Prospective studyofbiofeedbacktreatmentforpatientswithslowand normaltransitconstipation.EurJGastroenterolHepatol. 1994;6:131–8.
14.AgachanF,ChenT,PfeiferJ,ReissmanP,WexnerSD.A constipationscoringsystemtosimplifyevaluationand managementofconstipatedpatients.DiseasesColon Rectum.1996;39:681–5.
15.IrionJM,IrionG,editors.Women’shealthinphysicaltherapy. LippincottWilliams&Wilkins;2010.p.126–30.
16.BerghmansBo.Evidence-basedphysicaltherapyforthe pelvicfloor;2015.p.56–67.
17.GillilandR,HeymenS,AltomareDF,ParkUC,VickersD, WexnerSD.Outcomeandpredictorsofsuccessof biofeedbackforconstipation.BrJSurg.1997;84:1123–6.
18.FaridM,ElMonemHA,OmarW,ElNakeebA,FikryA,Youssef T,etal.Comparativestudybetweenbiofeedbackretraining andbotulinumneurotoxininthetreatmentofanismus patients.IntJColorectalDis.2009;24:115–20.
19.GliaA,GylinM,GullbergK,LindbergG.Biofeedbackretraining inpatientswithfunctionalconstipationandparadoxical puborectaliscontraction.DiseasesColonRectum. 1997;40:889–95.
20.Fernández-fragaX,AzpirozF,CasausM,ApariciA,
MalageladaJR.Responsesofanalconstipationtobiofeedback treatment.ScandJGastroenterol.2005;40:20–7.
21.TurnbullGK,RitvoPG.Analsphincterbiofeedbackrelaxation treatmentforwomenwithintractableconstipation
symptoms.DiseasesColonRectum.1992;35:530–6.
22.BattagliaE,SerraAM,BuonafedeG,DugheraL,ChistoliniF, MorelliA,etal.Long-termstudyontheeffectsofvisual biofeedbackandmuscletrainingasatherapeuticmodalityin pelvicfloordyssynergiaandslow-transitconstipation. DiseasesColonRectum.2004;47:90–5.
23.Chiotakakou-FaliakouE,KammMA,RoyAJ,StorrieJB,Turner IC.Biofeedbackprovideslongtermbenefitforpatientswith intractable,slowandnormaltransitconstipation.Gut. 1998;42:517–21.
24.WieselPH,DortaG,CuypersP,HerranzM,KreisME,Schnegg JF,etal.Patientstatisfactionafterbiofeedbackfor
constipationandpelvicfloordyssynergia.SwissMedWeekly. 2001;131:152–6.
25.LeeBH,KimN,KangSB,KimSY,LeeKH,ImBY,etal.The long-termclinicalefficacyofbiofeedbacktherapyforpatients withconstipationorfecalincontinence.JNeurogastroenterol Motil.2010;16:177–85.
26.LeeHJ,BooSJ,JungKW,HanS,SeoSY,KooHS,etal. Long-termefficacyofbiofeedbacktherapyinpatientswith dyssynergicdefecation:resultsofamedian44months follow-up.NeurogastroenterolMotility.2015;27:787–95.
27.RaoSS,ValestinJ,BrownCK,ZimmermanB,SchulzeK. Long-termefficacyofbiofeedbacktherapyfordyssynergic defecation:randomizedcontrolledtrial.AmJGastroenterol. 2010;105:890–6.