RESEARCH ARTICLE
Comparison of High, Intermediate, and Low
Frequency Shock Wave Lithotripsy for Urinary
Tract Stone Disease: Systematic Review and
Network Meta-Analysis
Dong Hyuk Kang1, Kang Su Cho2, Won Sik Ham1, Hyungmin Lee3, Jong Kyou Kwon4, Young Deuk Choi1, Joo Yong Lee1*
1Department of Urology, Severance Hospital, Urological Science Institute, Yonsei University College of Medicine, Seoul, Korea,2Department of Urology, Gangnam Severance Hospital, Urological Science Institute, Yonsei University College of Medicine, Seoul, Korea,3Division of Epidemic Intelligence Service, Korea Centers for Disease Control and Prevention, Osong, Korea,4Department of Urology, Severance Check-Up, Yonsei University Health System, Seoul, Korea
*joouro@yuhs.ac
Abstract
Objectives
To perform a systematic review and network meta-analysis of randomized controlled trials (RCTs) to determine the optimal shock wave lithotripsy (SWL) frequency range for treating urinary stones, i.e., high-frequency (100–120 waves/minute), intermediate-frequency (80–
90 waves/minute), and low-frequency (60–70 waves/minute) lithotripsy.
Materials and Methods
Relevant RCTs were identified from electronic databases for meta-analysis of SWL success and complication rates. Using pairwise and network meta-analyses, comparisons were made by qualitative and quantitative syntheses. Outcome variables are provided as odds ratios (ORs) with 95% confidence intervals (CIs).
Results
Thirteen articles were included in the qualitative and quantitative synthesis using pairwise and network meta-analyses. On pairwise meta-analyses, comparable inter-study heteroge-neity was observed for the success rate. On network meta-analyses, the success rates of low- (OR 2.2; 95% CI 1.5–2.6) and intermediate-frequency SWL (OR 2.5; 95% CI 1.3–4.6) were higher than high-frequency SWL. Forest plots from the network meta-analysis showed no significant differences in the success rate between low-frequency SWL versus intermedi-ate-frequency SWL (OR 0.87; 95% CI 0.51–1.7). There were no differences in complication rate across different SWL frequency ranges. By rank-probability testing, intermediate-fre-quency SWL was ranked highest for success rate, followed by low-freintermediate-fre-quency and
high-PLOS ONE | DOI:10.1371/journal.pone.0158661 July 7, 2016 1 / 22
a11111
OPEN ACCESS
Citation:Kang DH, Cho KS, Ham WS, Lee H, Kwon JK, Choi YD, et al. (2016) Comparison of High, Intermediate, and Low Frequency Shock Wave Lithotripsy for Urinary Tract Stone Disease: Systematic Review and Network Meta-Analysis. PLoS ONE 11(7): e0158661. doi:10.1371/journal. pone.0158661
Editor:Yu-Kang Tu, National Taiwan University, TAIWAN
Received:September 7, 2015
Accepted:June 20, 2016
Published:July 7, 2016
Copyright:© 2016 Kang et al. This is an open access article distributed under the terms of the
Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability Statement:All relevant data are within paper and its Supporting Information files.
Funding:This study was supported by a faculty research grant from the Yonsei University College of Medicine for 2014 (6-2014-0156).
frequency SWL. Low-frequency SWL was also ranked highest for low complication rate, with high- and intermediate-frequency SWL ranked lower.
Conclusions
Intermediate- and low-frequency SWL have better treatment outcomes than high-frequency SWL when considering both efficacy and complication.
Introduction
Since the introduction of shock wave lithotripsy (SWL) in the early 1980s, SWL has become a safe and accepted treatment modality for most intra-renal stones and many ureteral stones [1]. Despite the popular use of SWL, controversy remains regarding its success rate and the optimal shock wave (SW) frequency to achieve stone-free status.In vitroand animal studies have dem-onstrated that stone disintegration is influenced by the rate of SW administration, and slowing the rate to less than 120 SW/minute may improve stone fragmentation [2,3]. However, few clinical studies have evaluated the effect of varying SW frequency on stone fragmentation effi-ciency in humans [4,5].
The newly introduced network meta-analysis is a meta-analysis approach in which multiple treatments are compared using direct comparisons of interventions within randomized con-trolled trials (RCTs), and indirect comparisons are performed across trials based on a common comparator [6–9]. We performed a systematic review and network meta-analysis of RCTs to decide the optimal SW frequency range for disintegrating urinary stones by SWL. Frequency ranges were defined as high-frequency (100–120 SWs/minute), intermediate-frequency (80–90 SWs/minute), and low-frequency (60–70 SWs/minute).
Materials and Methods
Inclusion Criteria
Published RCTs that were in accordance with the following criteria were included: (i) Study design assessed different SW frequency ranges (100–120, 80–90, and 60–70 SWs/minute) to treat urinary tract stone disease. (ii) Baseline characteristics of patients from two or more groups were matched, including the total number of subjects and the values of each index. (iii) Outcomes of SWL were analyzed by stone-free or success rate according to each group. (iv) Standard indications for SWL to treat urinary tract stone disease were accepted. (v) Endpoint outcome parameters also included complication rate. (vi) The full text of the study was avail-able in English. This report was prepared in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (accessible athttp://www. prisma-statement.org/) [10]. A protocol for this study was shown inS1 Table.
Search Strategy
A literature search of all publications before 31 May 2015 was performed in EMBASE and PubMed. Additionally, a cross-reference search of eligible articles was performed to identify studies that were not found during the computerized search. The proceedings of appropriate meetings were also searched. Combinations of the following MeSH terms and keywords were used: extracorporeal shock wave lithotripsy, shock wave lithotripsy, frequency, renal stone, ure-ter stone, urolithiasis, success rate, stone-free, and randomized controlled trial (S2 Table).
Network Meta-Analysis of Optimal SWL Frequency
Data Extraction
A researcher (DHK) screened all titles and abstracts identified by the search strategy. Two other researchers (KSC and WSH) independently evaluated the full text of each paper to deter-mine whether a paper met the inclusion criteria. Disagreements were resolved by discussion until a consensus was reached or by arbitration mediated by another researcher (JYL).
Quality Assessment for Studies
After the final group of papers was agreed upon, two researchers (DHK and KSC) indepen-dently evaluated the quality of each article. The Cochrane Collaboration risk-of-bias as a qual-ity assessment tool for RCTs was used. This assessment includes assigning a judgment of“yes”,
“no”, or“unclear”for each domain to designate a low, high, or unclear risk of bias, respectively. If1 domain was deemed“unclear”or“no”, then the study was classified as having a low risk of bias; if 2–3 domains, then moderate risk of bias; and if4 domain, then a high risk of bias [11]. Quality assessment was performed with Review Manager 5 (RevMan 5.2.11 software, Cochrane Collaboration, Oxford, UK).
Heterogeneity Tests & Inconsistency Assessment
Heterogeneity of included studies was examined using the Q statistic and Higgins’I2statistic [12]. Higgins’I2measures the percentage of total variation due to heterogeneity rather than chance across studies. Higgins’I2was calculated as follows:
I2
¼Q df
Q 100%;
in which“Q”is Cochran's heterogeneity statistic, and“df”is the degrees of freedom. An I250% is considered to represent substantial heterogeneity [13]. For the Q statistic, heterogeneity was deemed to be significant for p<0.10 [14]. If there was evidence of heteroge-neity, the data were analyzed using a random-effects model. Studies in which positive results had been confirmed were assessed with a pooled specificity using 95% CIs. In addition, L’Abbe plot and Galbraith’s radial plot were created to evaluate heterogeneity [15,16]. To assess incon-sistency in the network, Cochran’s Q statistic and a net-heat plot were used and developed by Krahn et al. [17]. The net-heat plot is a graph that helps to identify pairwise comparisons that might be potential sources of important inconsistency in the network. A node-splitting analysis of inconsistency was applied in the forest plots of a network meta-analysis [18].
Statistical Analysis
Outcome variables measured at specific time points were compared in terms of odds ratios (OR) or mean differences with 95% CIs using a network meta-analysis. Analyses were based on non-informative priors for effect sizes and precision. Convergence and lack of auto-correlation were confirmed after four chains and a 50,000-simulation burn-in phase; finally, direct proba-bility statements were derived from an additional 100,000-simulation phase. The probaproba-bility that each group had the lowest rate of clinical events was assessed by Bayesian Markov Chain Monte Carlo modeling. Sensitivity analyses were performed by repeating the main computa-tions with a fixed-effect method. Model fit was appraised by computing and comparing esti-mates for deviance and deviance information criterion. All statistical analyses were performed with Review Manager 5 and R (R version 3.2.5, R Foundation for Statistical Computing, Vienna, Austria;http://www.r-project.org), the latter with associated netmeta, and gemtc pack-ages for pairwise and network meta-analyses.
Network Meta-Analysis of Optimal SWL Frequency
Results
Eligible Studies
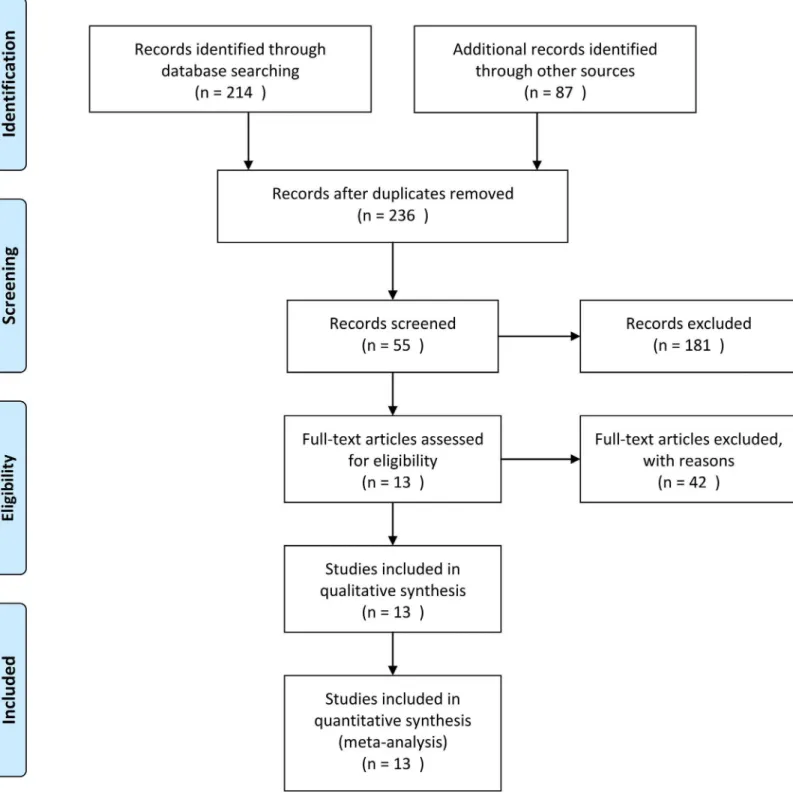
The database search retrieved 55 articles covering 236 studies for potential inclusion in the meta-analysis. Forty-two articles were excluded according to the inclusion/exclusion criteria; 28 articles were retrospective models, 11 articles were reviews, and 5 articles were reported as case series. The remaining 13 articles were included in the qualitative and quantitative synthe-sis using pairwise and network meta-analyses (Fig 1).
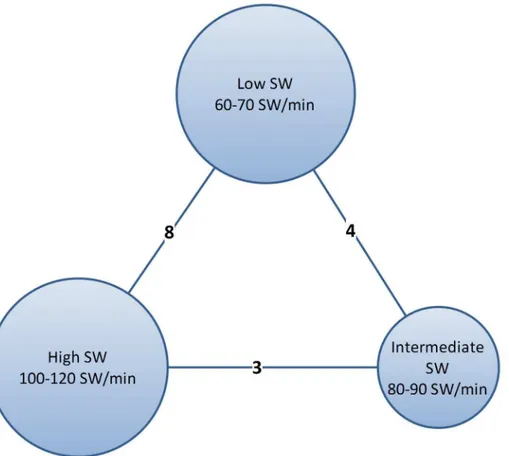
Data corresponding to confounding factors derived from each study are summarized in Table 1. Eight studies compared low-frequency SWL versus high-frequency SWL [5,19–25]. Four trials reported outcomes between low- versus intermediate-frequency SWL [20,26–28]. Three studies compared outcomes between high- and intermediate-frequency SWL [20,29,30] (Fig 2). We summarized the success and complications of enrolled studies inTable 2.
Quality Assessment
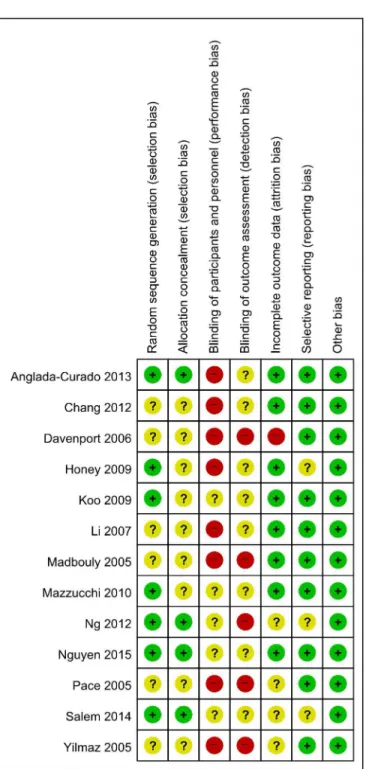
Fig 3presents details of quality assessment, as measured by the Cochrane Collaboration risk-of-bias tool. Seven trials exhibited a moderate risk of risk-of-bias for all quality criteria and two studies were classified as having a high risk of bias (Table 1). The most common risk factor for quality assess-ment was the blinding of participants and personnel (performance bias), and the second most common parameter concerned the blinding of outcome assessment (detection bias). These biases are related to study design, which can be performed in single-blinded or non-blinded formats.
Heterogeneity and Inconsistency Assessment, and Publication Bias
Forest plots of the pairwise meta-analyses of SWL success and complications are shown in Figs 4and5, respectively. A heterogeneity test for SWL success rate showed the following:χ2=46.78 with 14 df (P<0.001), and I2= 70.0% in the total test for success rate; andχ2= 8.35 with
2 df (P = 0.02) and I2= 76.1% in the test for subgroup differences. Thus, in success-rate analy-ses, the random-effect models were applied using the Mantel–Haenszel method. In the analysis of SWL complication rate, a heterogeneity test also demonstrated homogeneity withχ2= 6.58
with 8 df (P = 0.58) and I2= 0% in total test, andχ2= 0.53 with 2 df (P = 0.77) and I2= 0% in
the test for subgroup differences. Because there was no heterogeneity in forest plots for compli-cation rate, the fixed-effect models were applied using the Mantel–Haenszel method. In the L’Abbe plot, the success rate showed comparable inter-study heterogeneity (Fig 6A), and the complication rate had slight heterogeneity in the L’Abbe plot (Fig 6B). Radial plots revealed that three studies were located outside of the 95% CI of linear prediction (Fig 6C); however, the complication rates of all studies were inside of the 95% CI of linear prediction (Fig 6D).
On the assessments of homogeneity and consistency, the Q statistic showed inconsistency throughout the entire network (P = 0.073) and within designs (P = 0.0263); however, no incon-sistency was found between designs (P = 0.8434) on the success rate analysis. The Q statistic for the entire network between designs (after detaching single designs) demonstrated no incon-sistencies among all comparisons and triple comparisons with loops on success rate analysis. Additionally, on complication analysis, there was no inconsistency in the Q statistic (Table 3). On node-splitting analysis, no comparison demonstrated inconsistency among direct, indirect, and network comparisons (Fig 7). The net-heat plot also showed that there was only slight inconsistency throughout the entire network in terms of the success rate (Fig 8A), and there was no inconsistency in terms of the complication rate (Fig 8B).
Funnel plots from pairwise meta-analyses are demonstrated inFig 9; however, it was diffi-cult to assess publication bias using a limited number of studies, although some degree of bias
Network Meta-Analysis of Optimal SWL Frequency
is suspected. In addition, the Begg and Mazumdar rank correlation tests and Egger’s regression intercept tests for the success rate showed publication bias (P = 0.046 and P = 0.005, respec-tively). However, for the complication rate, there was no publication bias based on the two tests (P = 0.273 and P = 0.485, respectively).
Fig 1. Flow diagram of evidence acquisition.Thirteen studies were ultimately included in the qualitative and quantitative synthesis that used pairwise and network meta-analyses.
doi:10.1371/journal.pone.0158661.g001
Network Meta-Analysis of Optimal SWL Frequency
Table 1. Enrolled studies for this meta-analysis.
Study Year Location Size Lithotripter Models Type of lithotripter Frequency (SW/min) Frequency Categorya No. of Patients No. of Sessions Follow-up Duration Bias Riskb
Modified Bias Riskc
Pace et al [19]
2005 Renal N/A LithoTron (HealthTronics, Marietta, Georgia)
electrohydraulic 60 Low 111 1 3 months High Moderate
120 High 109 1
Yilmaz et al [20]
2005 Renal <20 mm Stone Litho3pter (PCK, Ankara,
Turkey); electrohydraulic
lithotripter
electrohydraulic 60 Low 57 1 10 days High Moderate
90 Intermediate 57 1
120 High 56 1
Madbouly et al [5]
2005 Renal or ureteral
30 mm electromagnetic Siemens Lithostar Multi-line lithotripter
electromagnetic 60 Low 76 1 to 3 3 months High Moderate
120 High 80 1 to 3
Davenport et al [21]
2006 Renal N/A Dornier Lithotripter S
electromagnetic 60 Low 49 1 3 months High Moderate
120 High 51 1
Li et al [29] 2007 Renal or ureteral
30 mm electromagnetic Siemens Lithostar Multi-line lithotripter
(Siemens, Munich, Germany)
electromagnetic 90 Intermediate 57 1 4 weeks High Moderate
120 High 59 1
Honey et al [22]
2009 Upper ureteral
5 mm Philips LithoTronTM spark gap lithotripter
electrohydraulic 60 Low 77 1 3 months High Moderate
120 High 86 1
Koo et al [23]
2009 Renal 20 mm Model S, Dornier MedTech, Wessling, Germany
electromagnetic 70 Low 51 1.3 6
months
Moderate Low
100 High 51 1.7
Mazzucchi et al [26]
2010 Renal or ureteral
>6 mm or symptomatic6
mm
Dornier Compact Delta lithotripter
electromagnetic 60 Low 143 N/A 3 months Moderate Low
90 Intermediate 157 N/A Chang et al
[25]
2012 Renal 5 to 20 mm Sonolith Praktis lithotripter (EDAP)
electroconductive 60 Low 81 N/A 3 months High Moderate
120 High 80 N/A
Ng et al [24] 2012 Renal 5 to 20 mm Sonolith Vision (EDAP)
electroconductive 60 Low 103 N/A 12 weeks High Moderate
120 High 103 N/A
Anglada-Curado et al [27]
2013 Distal ureteral
5 to 10 mm A Dornier Compact Delta lithotripter
electromagnetic 60 Low 78 1.14 12 months
Moderate Low
(Continued)
Table 1. (Continued)
Study Year Location Size Lithotripter Models Type of lithotripter Frequency (SW/min) Frequency Categorya No. of Patients No. of Sessions Follow-up Duration Bias Riskb
Modified Bias Riskc
80 Intermediate 72 1.56 Salem et al
[30]
2014 Renal 10 to 20 mm Dornier Lithotripter S
electromagnetic 80 Intermediate 30 1.53 After max. 3 sessions
High Moderate
120 High 30 2.1
Nguyen et al [28]
2015 Ureteral N/A Modified HM3 lithotripter
electrohydraulic 60 Low 127 N/A 3 months Moderate Low
90 Intermediate 113 N/A
a. Frequency ranges were defined as high-frequency (100–120 SWs/minute), intermediate-frequency (80–90 SWs/minute), and low-frequency (60–70 SWs/ minute).
b. Quality assessment was based on Cochrane’s risk of bias as a quality assessment tool for RCTs. If four or more domains are deemed“unclear”or“no,”the study was classified as having a high risk of bias. If two or three domains were deemed“unclear”or“no,”the study was classified as having a moderate risk of bias
c. Modified bias risk which excluded most common two biases (performance and detection biases), demonstrated that most of studies had low or moderate bias risk.
Pairwise Meta-analysis of Success and Complication Rates of SWL
Pooled data that assessed overall success showed a significantly lower rate of overall success with high-frequency SWL versus low-frequency SWL (OR 0.48; 95% CI 0.33–0.68; P<0.001), and high- versus intermediate-frequency SWL (OR 0.39; 95% CI 0.22–0.68; P<0.001). How-ever, forest plots showed no significant difference between intermediate- versus low-frequency SWL for success rate (OR 1.14; 95% CI 0.52–2.50; P = 0.74). The total test demonstrated that low-frequency SWL produced more favorable outcomes than high-frequency SWL (OR 0.56; 95% CI 0.39–0.79; P = 0.001) (Fig 4). Forest plots for complication rate demonstrated no signif-icant difference between high- versus low-frequency SWL (OR 1.41; 95% CI 0.92–2.18; P = 0.12), high- versus intermediate-frequency SWL (OR 0.98; 95% CI 0.38–2.51; P = 0.97), or intermediate- versus low-frequency SWL (OR 1.46; 95% CI 0.79–2.69; P = 0.22). The final pooled data for complication rate showed no significant difference between low-frequency SWL versus high-frequency SWL (OR 1.36; 95% CI 0.98–1.90; P = 0.07) (Fig 5).On subgroup analyses, there were no differences in the success rate for stones of less than 10 mm (Fig 10). However, for stones of 10 mm or greater, the success rate of low SW was higher than high SW (OR 0.31; 95% CI 0.17–0.56; P<0.001). Intermediate SW analyses that included only one study demonstrated success rates that were higher than high SW and lower than low SW (Fig 11). In renal stones, the success rate of low SW was higher than that of high SW (OR 0.47; 95% CI 0.27–0.81; P = 0.006;Fig 12).
Fig 2. Network plots for included studies.Eight studies compared low-shock wave (SW) versus high-SW frequency ranges. Four trials reported outcomes comparing low-SW versus intermediate-SW frequencies. Three studies compared outcomes between high-SW and intermediate-SW frequencies.
doi:10.1371/journal.pone.0158661.g002
Network Meta-Analysis of Optimal SWL Frequency
Network Meta-analysis of Success and Complication Rates of SWL
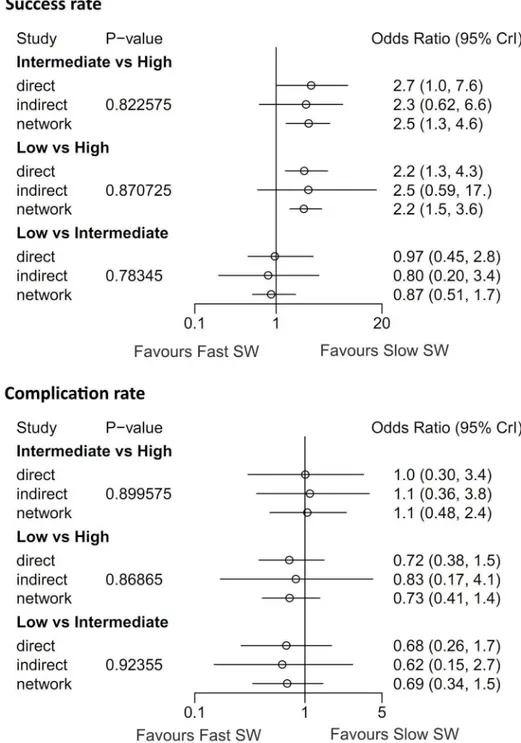
On network meta-analyses, the success rates of low- (OR 2.2; 95% CI 1.5–2.6) and intermedi-ate-frequency SWL (OR 2.5; 95% CI 1.3–4.6) were higher than high-frequency SWL (Fig 7A). Table 2. Success and complications of enrolled studies.Study Frequency (SW/min) Frequency Categorya No. of Patients No. of Success (%) Criterion of Success No. of Complication (%) Clavien grade
I II III IV
Pace et al [19]
60 Low 111 82 (73.9) <5 mm 12 (10.8) 10 1 1 0
120 High 109 66 (60.6) 21 (19.3) 19 1 1 0
Yilmaz et al [20]
60 Low 57 51 (89.5) <3 mm 0 (0) 0 0 0 0
90 Intermediate 57 50 (87.7) 0 (0) 0 0 0 0
120 High 56 41 (73.2) 1 (1.8) 1 0 0 0
Madbouly et al [5]
60 Low 76 75 (98.7) <2 mm NA N/A
120 High 80 72 (90.0) NA N/A
Davenport et al [21]
60 Low 49 29 (59.2) <4 mm 5 (10.2) N/A
120 High 51 31 (60.8) 4 (7.8) N/A
Li et al [29] 90 Intermediate 57 38 (66.7) <3 mm 5 (8.8) 5 0 0 0
120 High 59 27 (45.8) 6 (10.2) 6 0 0 0
Honey et al [22]
60 Low 77 50 (64.9) Stone
free
9 (11.7) 5 3 1 0
120 High 86 42 (48.8) 6 (7.0) 4 1 1 0
Koo et al [23]
70 Low 51 35 (68.6) Stone
free
NA N/A
100 High 51 14 (27.5) NA N/A
Mazzucchi et al [26]
60 Low 143 76 (53.1) 3 mm 7 (4.9) 6 1 0 0
90 Intermediate 157 86 (54.8) 10 (6.4) 7 3 0 0
Chang et al [25]
60 Low 81 57 (70.4) <4 mm NA N/A
120 High 80 46 (57.5) NA N/A
Ng et al [24]
60 Low 103 52 (50.5) <4 mm 14 (13.6) 14 0 0 0
120 High 103 37 (35.9) 23 (22.3) 23 0 0 0
Anglada-Curado et al [27]
60 Low 78 78 (100) Stone
free
NA N/A
80 Intermediate 72 67 (93.1) NA N/A
Salem et al [30]
80 Intermediate 30 27 (90.0) <3 mm 4 (13.3) 0 4 0 0
120 High 30 22 (73.3) 2 (6.7) 0 2 0 0
Nguyen et al [28]
60 Low 127 101
(79.5)
Stone free
13 (10.2) 6 2 1 4
90 Intermediate 113 103
(91.2)
17 (15.0) 4 1 5 7
a. Frequency ranges were defined as high-frequency (100–120 SWs/minute), intermediate-frequency (80– 90 SWs/minute), and low-frequency (60–70 SWs/ minute).
doi:10.1371/journal.pone.0158661.t002
Network Meta-Analysis of Optimal SWL Frequency
Forest plots from the network meta-analysis also showed no significant differences in the suc-cess rate between low-frequency SWL versus intermediate-frequency SWL (OR 0.87; 95% CI 0.51–1.7). In complication rate, there were no differences across all SW frequency categories (Fig 7B). In the rank-probability test, intermediate-frequency SWL had the highest rank for success rate, followed by low- and high-frequency SWL (Fig 13). Low-frequency SWL was also ranked highest for low complication rate. High- and intermediate-frequency SWL were ranked Fig 3. Risk-of-bias summary.Review author judgments for risk-of-bias items for each included study. Green, low risk of bias; Red, high risk of bias; Yellow, unclear of risk of bias.
doi:10.1371/journal.pone.0158661.g003
Network Meta-Analysis of Optimal SWL Frequency
lowest for low complication rate. A P-score test using a frequentist method to rank treatments in the network demonstrating intermediate-frequency SWL (P-score; 0.928) was superior to low- (P-score 0.572) and high-frequency SWL (P-score 0) in terms of the success rate [31]. Regarding the complication rate, the P-scores of low-, intermediate- and high-frequency SWL were 0.933, 0.217, and 0.350, respectively.
Discussion
With SWL implementation for curing urinary stone disease, balancing increased success rate with decreased complication remains a perennial problem for urologists. Many studies have Fig 4. Pairwise meta-analysis of success rate in each SW-frequency range following SWL.Pooled data that assessed overall success showed a significantly lower rate of overall success in the high-frequency SWL versus low-frequency SWL groups (OR 0.48; 95% CI 0.33–0.68; P<0.001), and in the
high-frequency SWL versus intermediate-frequency SWL groups (OR 0.39; 95% CI 0.22–0.68; P<0.001). However, forest plots showed no significant
difference in success rate between intermediate-frequency SWL versus low-frequency SWL.
doi:10.1371/journal.pone.0158661.g004
Network Meta-Analysis of Optimal SWL Frequency
shown that urinary stone size and location, lithotripter type, and operator skill are factors that influence the success rate of SWL treatment. Moreover, to maximize efficacy and SWL success rate, studies have focused on the effects of modifying controllable factors, such as SW fre-quency, maximum voltage escalation rate, and total number of shocks. In general, altering these factors is likely to illuminate an inverse relationship between the SWL efficacy and occur-rence of complications, depending on the magnitude of change. Thus, it is important to deter-mine the optimal range of these parameters that satisfies both efficacy and stability. Especially, many researchers have been interested in efficacy and stability resulting from using different SW frequencies.
Since the introduction of SWL, the most commonly used SW frequency has been 120 SW/ minute. However,in vivoandin vitroexperiments and clinical research from the mid-1990s Fig 5. Pairwise meta-analysis for complication rate in each shock wave frequency range following SWL.Forest plots for complication rate demonstrated no significant difference between high-frequency SWL versus low-frequency SWL (OR 1.41; 95% CI 0.92–2.18; P = 0.12), high-frequency SWL versus intermediate-frequency SWL (OR 0.98; 95% CI 0.38–2.51; P = 0.97), or intermediate-frequency SWL versus low-frequency SW (OR 1.46; 95% CI 0.79–2.69; P = 0.22).
doi:10.1371/journal.pone.0158661.g005
Network Meta-Analysis of Optimal SWL Frequency
showed that reducing the SW frequency increases stone fragmentation [2–4]. Since then, sev-eral RCTs have begun investigating the effect of decreasing SW frequency on procedure effi-cacy. The first RCTs were studies conducted by Madbouly et al [5] and Pace et al [19]. These groups compared the treatment outcome of SWL at 120 SW/minute versus 60 SW/minute, and both studies showed better outcomes using low-frequency SWL. Since then, several studies have further compared the influence of delivering high-frequency SWs versus low-frequency SWs, and confirmed improved results with low-frequency SWL [20,22–25].
Fig 6. L’Abbe plots of success (A) and complication rates (B), and Galbraith’s radial plots of success (C) and complication rates (D).In the L’Abbe plots, the success rate showed comparable inter-study heterogeneity, and the complication rate had slight heterogeneity. Radial plots revealed that three studies were located outside of the 95% CI of linear prediction; however, the complication rates of all studies were inside of the 95% CI of linear prediction.
doi:10.1371/journal.pone.0158661.g006
Network Meta-Analysis of Optimal SWL Frequency
Though the mechanism underlying the relative benefit of low-frequency SWL remains uncertain, several hypotheses have been generated regarding cavitation bubble generation. The first possible mechanism involves decreased mismatch of acoustic impedance [32]. This hypothesis states that higher SW delivery rates result in less effective SW energy transmission due to acoustic scattering and dampening, likely because of increased cavitation bubble pro-duction [33]. The shorter interval between SW pulses at higher delivery rates, the more bubbles are generated. Although cavitation bubbles on stone surfaces contribute to stone fragmenta-tion, continuous cavitation bubbles act as a barrier to SW energy transmission by forming bub-ble clouds, thereby reducing stone fragmentation effects. Thus, slower SW delivery rate removes the bubble barrier extent on the stone surface and supports better cluster dynamics that facilitate superior fragmentation [34]. Based on these hypothesized mechanisms, most studies that compared low-frequency versus high-frequency SWL have shown better results with low-frequency SW delivery. However, in the study conducted by Davenport et al [21], there was no difference in effectiveness between these two broad SWL frequency groups. The authors believed that the main reason for the similar results was that their studies were per-formed only on patients with small stones that were limited to the kidney. Our comprehensive meta-analyses of all reported RCTs to date confirm that performing SWL with a lower SW rate results in better outcomes than with a higher SW rate.
Though low-frequency SWL is more effective than high-frequency SWL, the main drawback is that it takes a longer time. Furthermore, although SWL approaches differ among countries and global regions, cost effectiveness aspects of lower SW delivery rates should be considered. Thus, several researchers have begun to take interest in using intermediate-frequency SWL. Li et al [29] reported that in 116 patients with renal or ureteral stones, 90 SW/minute led to better treatment outcomes than using 120 SW/minute, and the success rate was particularly increased in patients having a stone>10 mm. Salem et al [30] performed a study conducted on pediatric patients having larger renal stones (size range 10‒20 mm), and intermediate-frequency SWL
had significantly better treatment outcomes than using high-frequency SWL. In our meta-anal-ysis, the intermediate SW rate had significantly better efficacy than high-frequency SWL. Table 3. Design-based decomposition of Cochran’s Q in network meta-analyses of success and com-plication rates.
Success rate Complication rate
Q df P-value Q df P-value
Q statistic to assess homogeneity / consistency
Whole network 19.7 12 0.073 5.46 6 0.486
Within designs 18.87 9 0.026 5.46 5 0.362
Between designs 0.83 3 0.843 0 1 0.969
Between-designs Q statistic after detaching single designs
High vs. Intermediate 0.15 1 0.697 0.7 1 0.401
High vs. Low 11.5 6 0.074 4.76 4 0.313
Intermediate vs. Low 7.23 2 0.027 0 0 NA
Between-designs Q statistic after detaching single designs
High vs. Intermediate 0.82 2 0.662 0 0 NA
High vs. Low 0.68 2 0.712 0 0 NA
Intermediate vs. Low 0.77 2 0.680 0 0 NA
High vs. Intermediate vs. Low 0 1 0.975 NA NA NA
Q statistic to assess consistency under the assumption of a full design-by-treatment interaction random effects model
Between designs 0.48 3 0.924 0 1 0.982
doi:10.1371/journal.pone.0158661.t003
Network Meta-Analysis of Optimal SWL Frequency
Though differences in efficacy between high-frequency versus intermediate- and low-fre-quency SWL are obvious, there remains controversy about the comparative efficacy of Fig 7. Network meta-analysis for success and complication rates according to SWL frequency and node-splitting analyses of inconsistency.(A) The success rates of low- (OR 2.2; 95% CI 1.5–3.6) and intermediate-frequency SWL (OR 2.5; 95% CI 1.3–4.6) were higher than high-frequency SWL on the network analyses. (B) In terms of the complication rate, there were no differences across all SWL frequency groups. On node-splitting analysis, no comparisons demonstrated inconsistency between direct and indirect comparison in terms of success and complication rates. P-value: inconsistency p-values for each split comparison. Direct: direct comparison between two treatments. Indirect: indirect comparison between two treatments. Network: network meta-analysis between two treatments
doi:10.1371/journal.pone.0158661.g007
Network Meta-Analysis of Optimal SWL Frequency
intermediate- versus low-frequency SWL. Yilmaz et al [20] observed no difference in treatment outcome when comparing 90/minute and 60/minute SW rates, but the 90 SW rate was consid-ered to be the optimal frequency because of reduced procedural duration. Mazzucchi et al [26] reported no difference in the stone-free rate between two groups: one using 3000 total pulses at the 60 SW/minute rate, and the other implementing 4000 pulses at the 90 SW/minute rate. In a study of 154 patents with distal ureter stones, the 60 SW/minute rate showed better outcomes Fig 8. Net-heat plot for inconsistency.The net-heat plot also showed that there was only slight inconsistency throughout the entire network in terms of the (A) success rate; however, there was no inconsistency in terms of the (B) complication rate.
doi:10.1371/journal.pone.0158661.g008
Fig 9. Funnel plots of success (A) and complication rates (B).Little evidence of publication bias was demonstrated by visual or statistical examination of the funnel plots.
doi:10.1371/journal.pone.0158661.g009
Network Meta-Analysis of Optimal SWL Frequency
than the 80 SW/minute rate [27]. However, another study observed that the 90 SW/minute rate showed better outcomes than the 60 SW/minute rate [28]. Those researchers presented a different view than previous theories, and assumed that an increased SW delivery rate enhances cavitation bubble production on the stone surface, which enhanced fragmentation. In our meta-analysis, there was no significant efficacy difference between the intermediate-frequency and low-frequency groups. However, in the rank test, the intermediate SW rate was ranked highest for success. Because it remains difficult to conclusively determine the treatment out-come of the intermediate versus low SW rate with the existing data, large-sample RCTs should be performed.
We also performed a subgroup analysis for more stratified outcome data by size and loca-tion. There were several RCTs divided by 10-mm stone size, and there were no differences in the success rate for stones less than 10 mm. However, for stones of 10 mm or greater, the suc-cess rate of low SW was higher than high SW (five studies). The effect of SWL can be enhanced with larger stones, where SW energy is more effectively delivered to the stone surface, and this may be impacted by SW frequency. However, as only three studies included intermediate SW for stones of 10 mm or greater, the clinical significance might be very weak for intermediate-versus high-frequency groups and intermediate- intermediate-versus low-frequency groups.
As an indicator of treatment success, the complication rate is as important as the efficacy rate. Though decreased SW frequency may reduce incidental damage because of the decreased total number of shocks, it concurrently shows more effectiveness in stone fragmentation due to the altered cavitation bubble dynamics. Capillary rupture can be avoided by allowing more time for bubbles to dissipate between shocks [35]. Nonetheless, our pairwise and network meta-analyses indicated that there is no significant difference in the complication rate among Fig 10. Pairwise meta-analysis of success rates in each SW-frequency range following SWL in stones<10 mm.
There were no differences in the success rate for stones less than 10 mm.
doi:10.1371/journal.pone.0158661.g010
Network Meta-Analysis of Optimal SWL Frequency
the three SW-frequency groups. The reason might be because most studies have shown very low overall complication rates of SWL, without reference to using any specific SW frequency, which reflects the overall safety of the SWL approach. Therefore, although there might be no need to place great importance on potential complications when determining the optimal fre-quency for SWL, our rank-test results showed that low SW frefre-quency was ranked highest for the low complication rate. Thus, an additional study on complications of SWL depending on applied SW frequency is needed.
One limitation of our meta-analysis is that we did not assess the impact of the total number of SWs delivered as a function of SW frequency, which may have introduced critical bias. In the results, there was another limitation in that the success rate showed a degree of heterogene-ity in the forest, L’Abbe, and radial plots. Thus, we used a random effect model to analyze the outcome in terms of the success rate. Additionally, our study was also susceptible to a degree of publication bias. However, Sutton et al. reviewed 48 articles from the Cochrane Database of Systematic Reviews and showed that publication bias and related biases were common within their meta-analysis sample [36]. They found that these biases did not affect the conclusions in most cases. Similar to heterogeneity, inconsistency is caused by effect modifiers and specifically by an imbalance in the distribution of effect modifiers in the direct and indirect evidence from the network meta-analysis [37,38]. In our study, there was only slight inconsistency on network analyses using Cochran’s Q statistic, node-splitting analysis, and net-heat plots. Thus, in our results, there was agreement between direct and indirect comparison. Despite these limitations, our study has sufficient value as a meta-analysis because it spans studies performed over a Fig 11. Pairwise meta-analysis of success rates in each SW-frequency range following SWL in stones10 mm.
The success rate of low SW was higher than that of high SW (OR 0.31; 95% CI 0.17–0.56; P<0.001). Intermediate SW
analyses that included only one study demonstrated success rates that were higher than high SW and lower than low SW.
doi:10.1371/journal.pone.0158661.g011
Network Meta-Analysis of Optimal SWL Frequency
Fig 12. Pairwise meta-analysis of success rates in each SW-frequency range following SWL for renal stones.
The success rate of low SW was higher than that of high SW (OR 0.47; 95% CI 0.27–0.81; P = 0.006)
doi:10.1371/journal.pone.0158661.g012
Fig 13. Rank-probability test of network meta-analyses.Intermediate-frequency SWL had the highest rank for success rate, followed by low- and high frequency SWL (A) Low-frequency SWL also ranked highest for low complication rate, (B) High- and intermediate-frequency SWL were ranked lowest for low complication rate.
doi:10.1371/journal.pone.0158661.g013
Network Meta-Analysis of Optimal SWL Frequency
longer period than previous analyses [39]. Moreover, the current study is unique as it applied network meta-analysis methods in order to enhance the statistical confidence and overcome the limitations of pairwise meta-analysis.
Conclusions
Network meta-analysis of published RCT data on SWL frequency confirms that intermediate-frequency and low-intermediate-frequency SWL show better treatment outcomes than high-intermediate-frequency SWL in terms of both efficacy and complication rates. However, we require more data to conclu-sively determine whether intermediate versus low SW rates produce optimal results in SWL.
Supporting Information
S1 Table. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
(DOC)
S2 Table. Search strategy in PubMed. (DOC)
Acknowledgments
This study was supported by a faculty research grant from the Yonsei University College of Medicine for 2014 (6-2014-0156).
Author Contributions
Conceived and designed the experiments: JYL. Performed the experiments: DHK KSC WSH HL YDC JYL. Analyzed the data: DHK JYL. Contributed reagents/materials/analysis tools: JYL DHK. Wrote the paper: DHK KSC WSH JKK YDC.
References
1. Chung DY, Cho KS, Lee DH, Han JH, Kang DH, Jung HD, et al. Impact of colic pain as a significant fac-tor for predicting the stone free rate of one-session shock wave lithotripsy for treating ureter stones: a Bayesian logistic regression model analysis. PLOS One 2015; 10:e0123800. doi:10.1371/journal. pone.0123800PMID:25902059
2. Greenstein A, Matzkin H. Does the rate of extracorporeal shock wave delivery affect stone fragmenta-tion? Urology 1999; 54:430–2. PMID:10475348
3. Paterson RF, Lifshitz DA, Lingeman JE, Evan AP, Connors BA, Fineberg NS, et al. Stone fragmenta-tion during shock wave lithotripsy is improved by slowing the shock wave rate: studies with a new ani-mal model. J Urol 2002; 168:2211–5. PMID:12394761
4. Robert M, Rakotomalala E, Delbos O, Navratil H. Piezoelectric lithotripsy of ureteral stones: influence of shockwave frequency on sedation and therapeutic efficiency. J Endourol 1999; 13:157–60. PMID: 10360493
5. Madbouly K, El-Tiraifi AM, Seida M, El-Faqih SR, Atassi R, Talic RF. Slow versus fast shock wave litho-tripsy rate for urolithiasis: a prospective randomized study. J Urol 2005; 173:127–30. PMID:15592053
6. Caldwell DM, Ades AE, Higgins JP. Simultaneous comparison of multiple treatments: combining direct and indirect evidence. BMJ 2005; 331:897–900. PMID:16223826
7. Mills EJ, Thorlund K, Ioannidis JP. Demystifying trial networks and network meta-analysis. BMJ 2013; 346:f2914. doi:10.1136/bmj.f2914PMID:23674332
8. Yuan J, Zhang R, Yang Z, Lee J, Liu Y, Tian J, et al. Comparative effectiveness and safety of oral phos-phodiesterase type 5 inhibitors for erectile dysfunction: a systematic review and network meta-analysis. Eur Urol 2013; 63:902–12. doi:10.1016/j.eururo.2013.01.012PMID:23395275
Network Meta-Analysis of Optimal SWL Frequency
9. Kwon JK, Cho KS, Oh CK, Kang DH, Lee H, Ham WS, et al. The beneficial effect of alpha-blockers for ureteral stent-related discomfort: systematic review and network meta-analysis for alfuzosin versus tamsulosin versus placebo. BMC Urol 2015; 15:55. doi:10.1186/s12894-015-0050-5PMID:26104313
10. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLOS Med 2009; 6:e1000097. doi:10.1371/journal.pmed.1000097 PMID:19621072
11. Chung JH, Lee SW. Assessing the quality of randomized controlled urological trials conducted by korean medical institutions. Korean J Urol 2013; 54:289–96. doi:10.4111/kju.2013.54.5.289PMID: 23700493
12. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003; 327:557–60. PMID:12958120
13. Lee JY, Kang DH, Chung DY, Kwon JK, Lee H, Cho NH, et al. Meta-Analysis of the Relationship between CXCR4 Expression and Metastasis in Prostate Cancer. World J Mens Health 2014; 32:167– 75. doi:10.5534/wjmh.2014.32.3.167PMID:25606566
14. Fleiss JL. Analysis of data from multiclinic trials. Control Clin Trials 1986; 7:267–75. PMID:3802849
15. L'Abbe KA, Detsky AS, O'Rourke K. Meta-analysis in clinical research. Ann Intern Med 1987; 107:224– 33. PMID:3300460
16. Galbraith RF. A note on graphical presentation of estimated odds ratios from several clinical trials. Stat Med 1988; 7:889–94. PMID:3413368
17. Krahn U, Binder H, Konig J. Visualizing inconsistency in network meta-analysis by independent path decomposition. BMC Med Res Methodol 2014; 14:131. doi:10.1186/1471-2288-14-131PMID: 25510877
18. Neupane B, Richer D, Bonner AJ, Kibret T, Beyene J. Network meta-analysis using R: a review of cur-rently available automated packages. PLOS One 2014; 9:e115065. doi:10.1371/journal.pone. 0115065PMID:25541687
19. Pace KT, Ghiculete D, Harju M, Honey RJ. Shock wave lithotripsy at 60 or 120 shocks per minute: a randomized, double-blind trial. J Urol 2005; 174:595–9. PMID:16006908
20. Yilmaz E, Batislam E, Basar M, Tuglu D, Mert C, Basar H. Optimal frequency in extracorporeal shock wave lithotripsy: prospective randomized study. Urology 2005; 66:1160–4. PMID:16360432
21. Davenport K, Minervini A, Keoghane S, Parkin J, Keeley FX, Timoney AG. Does rate matter? The results of a randomized controlled trial of 60 versus 120 shocks per minute for shock wave lithotripsy of renal calculi. J Urol 2006; 176:2055–8. PMID:17070254
22. Honey RJ, Schuler TD, Ghiculete D, Pace KT. A randomized, double-blind trial to compare shock wave frequencies of 60 and 120 shocks per minute for upper ureteral stones. J Urol 2009; 182:1418–23. doi: 10.1016/j.juro.2009.06.019PMID:19683303
23. Koo V, Beattie I, Young M. Improved cost-effectiveness and efficiency with a slower shockwave deliv-ery rate. BJU Int 2010; 105:692–6. doi:10.1111/j.1464-410X.2009.08919.xPMID:19888982
24. Ng CF, Lo AK, Lee KW, Wong KT, Chung WY, Gohel D. A prospective, randomized study of the clinical effects of shock wave delivery for unilateral kidney stones: 60 versus 120 shocks per minute. J Urol 2012; 188:837–42. doi:10.1016/j.juro.2012.05.009PMID:22819406
25. Chang SH, Shon JH, Lee JW, Jo DS. Optimal frequency of shock wave lithotripsy in urolithiasis treat-ment; prospective randomized study. J Endourol 2012;A343.
26. Mazzucchi E, Brito AH, Danilovic A, Ebaid GX, Chedid Neto E, Azevedo JR, et al. Comparison between two shock wave regimens using frequencies of 60 and 90 impulses per minute for urinary stones. Clin-ics 2010; 65:961–5. PMID:21120294
27. Anglada-Curado FJ, Campos-Hernandez P, Carrasco-Valiente J, Anaya-Henares F, Carazo-Carazo JL, Alvarez-Kindelan J, et al. Extracorporeal shock wave lithotripsy for distal ureteral calculi: improved efficacy using low frequency. Int J Urol 2013; 20:214–9. doi:10.1111/j.1442-2042.2012.03133.xPMID: 22970896
28. Nguyen DP, Hnilicka S, Kiss B, Seiler R, Thalmann GN, Roth B. Optimization of Extracorporeal Shock Wave Lithotripsy Delivery Rates Achieves Excellent Outcomes for Ureteral Stones: Results of a Pro-spective Randomized Trial. J Urol 2015; 194:418–23. doi:10.1016/j.juro.2015.01.110PMID:25661296
29. Li WM, Wu WJ, Chou YH, Liu CC, Wang CJ, Huang CH, et al. Clinical predictors of stone fragmentation using slow-rate shock wave lithotripsy. Urol Int 2007; 79:124–8. PMID:17851280
30. Salem HK, Fathy H, Elfayoumy H, Aly H, Ghonium A, Mohsen MA, et al. Slow vs rapid delivery rate shock wave lithotripsy for pediatric renal urolithiasis: a prospective randomized study. J Urol 2014; 191:1370–4. doi:10.1016/j.juro.2013.11.028PMID:24262496
Network Meta-Analysis of Optimal SWL Frequency
31. Rucker G, Schwarzer G. Ranking treatments in frequentist network meta-analysis works without resampling methods. BMC Med Res Methodol 2015; 15:58. doi:10.1186/s12874-015-0060-8PMID: 26227148
32. Eisenmenger W. The mechanisms of stone fragmentation in ESWL. Ultrasound Med Biol 2001; 27:683–93. PMID:11397533
33. Huber P, Debus J, Jochle K, Simiantonakis I, Jenne J, Rastert R, et al. Control of cavitation activity by different shockwave pulsing regimes. Phys Med Biol 1999; 44:1427–37. PMID:10498515
34. Choi MJ, Coleman AJ, Saunders JE. The influence of fluid properties and pulse amplitude on bubble dynamics in the field of a shock wave lithotripter. Phys Med Biol 1993; 38:1561–73. PMID:8272432
35. Zhong P, Zhou Y, Zhu S. Dynamics of bubble oscillation in constrained media and mechanisms of ves-sel rupture in SWL. Ultrasound Med Biol 2001; 27:119–34. PMID:11295278
36. Sutton AJ, Duval SJ, Tweedie RL, Abrams KR, Jones DR. Empirical assessment of effect of publication bias on meta-analyses. BMJ 2000; 320:1574–7. PMID:10845965
37. Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. Evidence synthesis for decision making 4: inconsistency in networks of evidence based on randomized controlled trials. Med Decis Making 2013; 33:641–56. doi:10.1177/0272989X12455847PMID:23804508
38. Salanti G, Del Giovane C, Chaimani A, Caldwell DM, Higgins JP. Evaluating the quality of evidence from a network meta-analysis. PLOS One 2014; 9:e99682. doi:10.1371/journal.pone.0099682PMID: 24992266
39. Li K, Lin T, Zhang C, Fan X, Xu K, Bi L, et al. Optimal frequency of shock wave lithotripsy in urolithiasis treatment: a systematic review and meta-analysis of randomized controlled trials. J Urol 2013; 190:1260–7. doi:10.1016/j.juro.2013.03.075PMID:23538240
Network Meta-Analysis of Optimal SWL Frequency