www.revportcardiol.org
Revista
Portuguesa
de
Cardiologia
Portuguese
Journal
of
Cardiology
CASE
REPORT
Percutaneous
closure
of
a
large
ascending
aortic
pseudoaneurysm
Marta
Afonso
Nogueira
a,∗,
António
Fiarresga
a,
Lídia
de
Sousa
a,
Ana
Galrinho
a,
Ninel
Santos
a,
Isabel
Nobre
b,
Álvaro
Laranjeira
c,
Rui
Cruz
Ferreira
aaDepartmentofCardiology,SantaMartaHospital,Lisbon,Portugal bDepartmentofRadiology,LusíadasHospital,Lisbon,Portugal
cDepartmentofCardiothoracicSurgery,SantaMartaHospital,Lisbon,Portugal
Received27April2015;accepted16October2015
Availableonline3February2016
KEYWORDS Ascendingaorta; Pseudoaneurysm; Percutaneousclosure
Abstract Pseudoaneurysmoftheascendingaortaisararecomplication,usuallyafterthoracic
surgeryortrauma.
Since surgical repair is associated with very high morbidity and mortality, percutaneous
closurehasbeendescribedasanalternative.
In this regard,we present acase in which a symptomatic large pseudoaneurysm of the
ascendingaortawastreatedpercutaneouslyduetothehighsurgicalrisk.
Despitethetechnicaldifficulties,thisprocedurehadagoodfinalresultfollowedbyclinical
success.
©2016SociedadePortuguesa deCardiologia.Publishedby ElsevierEspaña,S.L.U.All rights
reserved. PALAVRAS-CHAVE Aortaascendente; Pseudoaneurisma; Encerramento percutâneo
Encerramentopercutâneodeumvolumosopseudoaneurismadaaortaascendente Resumo Opseudoaneurismadaaortaascendenteconsistenumacomplicac¸ãorara,
habitual-mentenasequênciadecirurgiacardiotorácicaoutraumatismo.
Dado queareparac¸ãocirúrgicadomesmose associaaumaelevada morbimortalidade,o
encerramentopercutâneotemvindoaserdescritocomoumaalternativaviável.
∗Correspondingauthor.
E-mailaddress:marta.afonso.nogueira@gmail.com(M.A.Nogueira). http://dx.doi.org/10.1016/j.repc.2015.09.021
Neste contexto,apresentamosum casocaracterizadoporum volumosoe sintomático
pseu-doaneurismadaaortaascendente,oqualforasubmetidoatratamentopercutâneo,devidoao
elevadoriscocirúrgico.
Apesardasdificuldadesdopontodevistatécnico,esteprocedimentoobteveumbom
resul-tadofinal,comsucessoemtermosclínicos.
©2016SociedadePortuguesadeCardiologia.PublicadoporElsevierEspaña,S.L.U.Todosos
direitosreservados.
Introduction
Pseudoaneurysmoftheascendingaortaisarelativelyrare but serious complication that usually develops following thoracicsurgery,includingaorticvalvereplacement, coro-nary artery bypass grafting, aortic dissection repair and orthotopiccardiactransplantation.1---5Theincidenceofthis
complication following aortic surgery can reach 23% at 15 years after surgery. Other potential etiologies include endocarditisandthoracictrauma.6
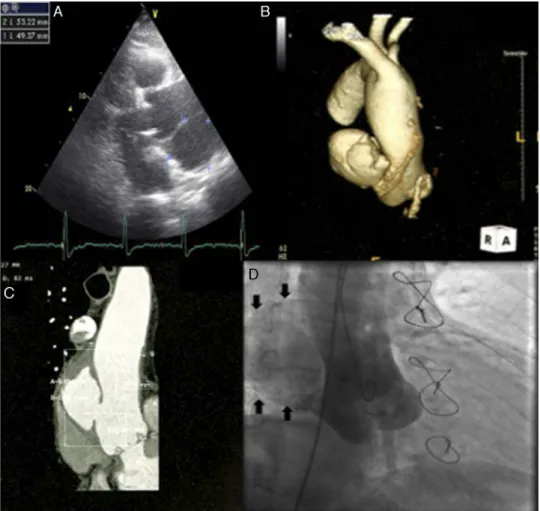
Figure1 Imaging ofascendingaortic pseudoaneurysm.(A)Transthoracic echocardiographyshowingascending aortic
pseudo-aneurysminparasternalview;(B)three-dimensionalcomputedtomography(CT)reconstructionofaorta;(C)CTscanwith
intra-venouscontrastshowingthedimensionsoftheneckandcavityofthepseudoaneurysm;(D)aortographywithcontrastopacification
ofpseudoaneurysmcavity(solidarrows).
Clinical presentation ranges from completely asymp-tomaticfor yearstosymptomsrelated tothemasseffect onsurroundingstructures.6
Ifleftuntreated,aorticpseudoaneurysmscanevolveto rupture,thrombosis,distalembolizationandfistula forma-tion,withhighmortality(upto61%).6
Surgical repairof thiscomplication isthe conventional treatment, but it is associated with very high morbidity andmortality(mortalitycanreach46%)andinsomecases is not even feasible (due to the technical difficulties in
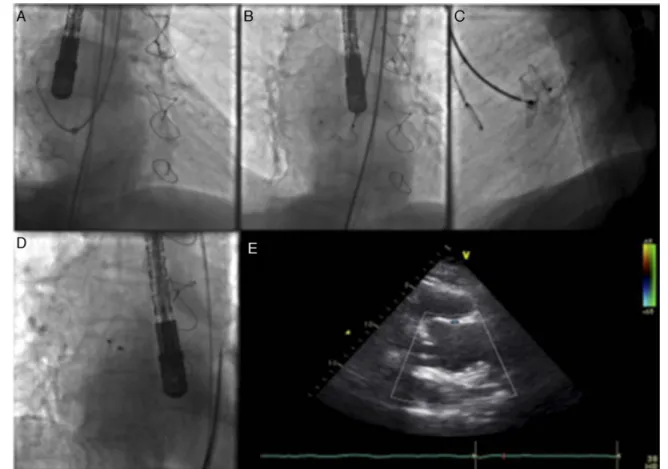
Figure2 Images illustratingpercutaneousclosureofaortic pseudoaneurysm. (A)Left internalmammary diagnosticcatheter
insidethedeliverysheathengagingthepseudoaneurysmcavity;(B)Amplatzeratrialseptaldefect(ASD)occluderwiththedistal
diskopenedinsidethepseudoaneurysmcavity,andtheproximaldiskmisshapeninsidetheaorticlumen;(C)AmplatzerASDdevice
deployedacrosstheaorticwalldefect;(D)AmplatzerASDdevicereleasedinastableposition;(E)transthoracicechocardiography
showingpositionofthedevicewithoutinterferingwiththebioprosthesis.
patients who have undergone prior complex thoracic sur-geries),sopercutaneousclosure hasbeendescribed asan alternative.1---6
Inthepast,severalpercutaneoustechniquesforclosure of a pseudoaneurysm have been attempted such asstent grafting, coil implantation or thrombin injection, but the finalresultsobtainedweresuboptimal.Inrecentyears, dif-ferent types of deviceshave occasionallybeen usedwith successinoff-labelindications.Thefirstpercutaneous clo-surewaspublishedin2005,butexperiencesincethenhas beenlimited,usuallytopatientsnotsuitableforsurgeryor withhighsurgicalrisk.Thelatestcasewaspublishedin2014, withagoodfinalresultandwithoutcomplications.2---4,6
Over-all,thesuccessratefor percutaneousclosureis80%,with a 12% device embolization rate and an 8% failure rate of thetranscathetertechniquetoclosethepseudoaneurysm, necessitatingconversiontosurgicalclosure.5,6
Wepresentacaseinwhichasymptomaticlarge pseudo-aneurysmoftheascendingaortawastreatedpercutaneously duetothepatient’shighsurgicalrisk.
Case
report
An 81-year-old man with a history of aortic bioprosthe-sisimplanted duetosevere aorticregurgitation,coronary
arterydisease(treatedbypercutaneoustransluminal coro-nary angioplasty of the mid left anterior descending artery),arterial hypertensionand dyslipidemia,was eval-uated for atypical thoracic pain, after an asymptomatic period of two years post surgery. The patient was med-icated with aspirin 100 mg daily, lisinopril 20 mg daily, carvedilol 6.25 mg twice daily, omeprazole 20 mg daily androsuvastatin10mg,withgoodcontrolof vascularrisk factors.
During complementary investigation, a chest X-ray showed widening of the mediastinal silhouette and a transthoracicechocardiogram revealed a pseudoaneurysm of the ascending aorta, 35 mm above the aortic valve (Figure1A).
Coronary computed tomography angiography (CCTA) (Figure1Band 1C)andaortography(Figure1D)confirmed alarge pseudoaneurysm(98 mm×48mm) anda defectin theaorticwall(19mm×19mm).
The patientwas considered to beat high surgical risk (EuroSCORE II of 12.21%) and was referred for percuta-neous treatment (closure of the pseudoaneurysm with a non-dedicateddevice).
Firstofall,anattemptwasmadewitha9FAmplatzer®
TorqueVue® deliverysheaththrougharight femoralartery
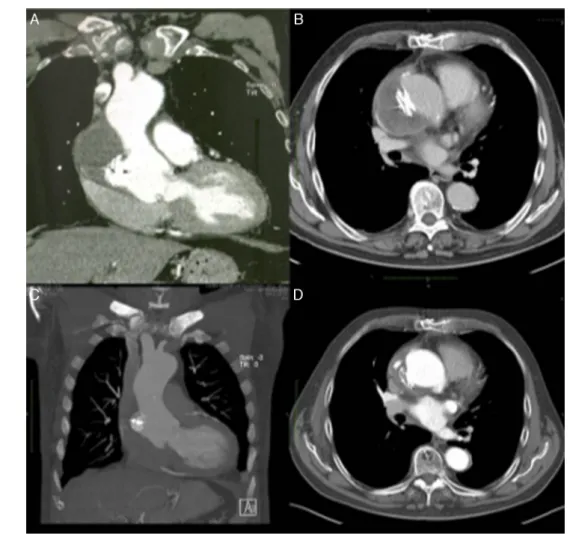
Figure3 Evolutionovertimeofascendingaortic pseudoaneurysmclosure.(A andB)Computedtomography(CT) scanatone
monthshowingAmplatzerASDdeviceinastablepositionandorganizingthrombusinsidethepseudoaneurysmcavity;(CandD)CT
scanatoneyearwithdevicemaintainingitspositionandpartialresolutionoftheexcludedpseudoaneurysmcavity.
standard 0.035 wire and a left internal mammary diag-nostic catheter inside the delivery sheath, but this was too short and did not enter the pseudoaneurysm cavity (Figure 2A). The sheath was then changed to a 12 F St. Jude®/Daig®sheaththatsuccessfullyenteredthe
pseudoa-neurysm. A 20 mm Amplatzer® atrial septal defect (ASD)
occluder was used, although considerable resistance was encountered navigating the device and it was impossible to proceed behind the aortic arch. An 8F Judkins Right guidecatheter,withitsproximaltipcut,wasplacedinside the delivery sheath for extra support, in a mother-child technique,enabling the deviceto navigatedistally inthe sheath. At first, the proximaldisk did not conformto its originalconfiguration(Figure2B),butafteraseriesof care-ful retrieval and reposition maneuvers the device finally acquiredastableposition(Figure2C---E).
CCTA at one month (Figure 3A and B) and 12 months (Figure3C andD) after theprocedure showed thedevice correctlypositionedandcompleteclosureofthe pseudoa-neurysmwiththrombosisofitscavity.
After14monthsoffollow-upthepatientremains asymp-tomaticandwithoutanyevents.
Discussion
and
conclusion
This case report illustrates a relatively rare complication of thoracic surgery, namely an ascending aorta pseudoa-neurysm.
Althoughsurgicalrepairremainsthedefinitivetherapy,in viewofthepatient’shighperioperativeriskhewastreated bypercutaneousclosureofthepseudoaneurysm,whichhas ahigh(80%)successrate,asdescribedintheliterature.2---6
Experiencewithpercutaneousclosureofaortic pseudo-aneurysms has increased steadily since the introduction of the technique in 2005, with several benefits, includ-ingfewerpotentialcomplicationsandavoidanceofsurgical risk.6
Inthiscase,despiteallthetechnicaldifficulties,the pro-cedurehadbothimagingandclinicalsuccess,renderingthe patientasymptomaticandwithouteventsinafollow-upof overoneyear.
Consequently,thisresultconfirmsthatpercutaneous clo-sure witha non-dedicateddevice isan effective andsafe alternative to surgery asa definitive treatment in aortic pseudoaneurysms.
Ethical
disclosures
Protection of human and animal subjects.The authors declarethatnoexperimentswereperformedonhumansor animalsforthisstudy.
Confidentialityofdata.Theauthorsdeclarethattheyhave followedtheprotocolsoftheirworkcenteronthe publica-tionofpatientdata.
Righttoprivacyandinformedconsent.Theauthorshave obtained the written informedconsent of thepatients or subjectsmentionedinthearticle.Thecorrespondingauthor isinpossessionofthisdocument.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
References
1.D’Attellies N, Diemont FF, Julia PL, et al. Management of pseudoaneurysm of the ascending aorta performed under
circulatory arrest by port-access. Ann Thorc Surg. 2001;71: 1010---1.
2.BashirF,QuaifeR,CarrollJD.Percutaneousclosureofascending aorticpseudoaneurysmusingAmplatzerseptaloccluderdevice: thefirstclinicalcasereportandliteraturereview.Catheter Car-diovascInterv.2005;65:547---51.
3.Kanani RS, Neilan TG, Palacios IF, et al. Novel use of the Amplatzer septaloccluder deviceinthe percutaneousclosure of ascendingaortic pseudoaneurysms: acase series.Catheter CardiovascInterv.2007;69:146---53.
4.StasekJ,PolanskyP,BisJ,etal.Thepercutaneousclosureofa largepseudoaneurysmoftheascendingaortawithanatrialseptal defectAmplatzeroccluder:two-yearfollow-up.CanJCardiol. 2008;24:e99---101.
5.NobleS,IbrahimR.EmbolizationofanAmplatzermVSDoccluder device usedfor percutaneous closure of an ascending aortic pseudoaneurysm: casereport and literaturereview. Catheter CardiovascInterv.2012;79:334---8.
6.Patel AV,Gupta S, Laffin LJ, et al. One size does notfit all: case report of two percutaneous closures of aortic pseudo-aneurysmandreviewoftheliterature.CardiovascRevascMed. 2014;15:160---4.