www.rpped.com.br
REVISTA
PAULISTA
DE
PEDIATRIA
ORIGINAL
ARTICLE
Factors
associated
with
short
sleep
duration
in
adolescents
Érico
Pereira
Gomes
Felden
a,∗,
Douglas
Filipin
a,
Diego
Grasel
Barbosa
a,
Rubian
Diego
Andrade
a,
Carolina
Meyer
a,
Fernando
Mazilli
Louzada
baUniversidadedoEstadodeSantaCatarina(Udesc),Florianópolis,SC,Brazil
bUniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
Received2March2015;accepted26May2015 Availableonline4November2015
KEYWORDS
Schoolhealth; Sleep; Habits; Adolescents
Abstract
Objective: Thisstudyaimedtoinvestigatetheprevalenceandfactorsassociatedwithshort sleepdurationinadolescentsfromMaravilha---SantaCatarina(SC),southernBrazil.
Methods: Thesampleconsistedof516adolescentsaged10---19yearsofbothgenders.Issues associatedwithshortsleepdurationanddifficultyfallingasleep,chronotype,daytime sleepi-ness,physicalactivity,sedentarybehaviorandweightstatuswereinvestigated.
Results: Theprevalenceofshortsleepduration(<8honschooldays)was53.6%.Adolescents aged 17---19 yearsshowed a 2.05-fold(95%CI: 1.20---3.50) greaterprevalenceof shortsleep durationthanthoseaged10---12years.Theonesstudyinginmorningandeveningshiftshada higherprevalenceofshortsleepdurationcomparedtothoseintheafternoonshift.Olderage andschoolshiftwerethemainfactorsassociatedwithshortsleepduration.
Conclusions: AdolescentsfromMaravilhashowedhighprevalenceofshortsleepduration,and olderadolescentsthatstudiedinthemorningandeveningshiftsshowedreducedsleep. ©2015SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(https://creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Saúdeescolar; Sono;
Hábitos; Adolescentes
Fatoresassociadosàbaixadurac¸ãodosonoemadolescentes
Resumo
Objetivo: Investigaraprevalênciaeosfatoresassociadosàbaixadurac¸ãodosonode adoles-centesdomunicípiodeMaravilha(SC),Brasil.
Métodos: A amostrafoiformadapor516adolescentes,de10a19anos,deambosossexos. Foraminvestigadas questõesassociadas àbaixadurac¸ãodosono,como dificuldadedepegar nosono,cronotipo,sonolênciadiurna,atividadefísica,comportamentosedentárioestatusde peso.
∗Correspondingauthor.
E-mail:[email protected](É.P.G.Felden).
http://dx.doi.org/10.1016/j.rppede.2015.10.007
Resultados: Aprevalênciadebaixadurac¸ãodosono(<8hnosdiascomaula)foide53,6%.Os adolescentescom17-19anostiveram2,05(IC95%1,20-3,50)vezesmaischancesdeapresentar baixa durac¸ãodosonodoqueoscom10-12 anos.Aquelesqueestudavamnosturnosmanhã enoiteapresentarammaiorprevalênciadebaixadurac¸ãodesono,comrelac¸ãoaosdoturno datarde.Idademaisavanc¸adaeturnoescolarforamosprincipaisfatoresassociadosàbaixa durac¸ãodosono.
Conclusões: OsadolescentesdeMaravilhaapresentaramaltaprevalênciadebaixadurac¸ãodo sono.Osmaisvelhos,queestudamdemanhãeànoite,apresentaramsonoreduzido.
©2015SociedadedePediatriadeS˜aoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Humanbeingsgo throughtransformations throughout life, both in physical aspect and in behavior.1 In this context,
especiallyinadolescence,itispossibletoobservesignificant
changesintheexpressionofthesleep/wakecycle,including
adelayinthesleepphase,characterizedbygoingtosleep
andwakingupatlatehours.2,3Thisbiologicaltendencymay
beexacerbatedbybehaviorssuchastheuse ofelectronic
mediaduringthenight,which,addedtosocialengagements
earlyinthemorning,increasetheprevalenceofshortsleep
durationinthispopulation.4
Overtheyears,inadolescence,theprevalenceof
short-duration, poor quality of sleep and excessive daytime
sleepinesstendstoprogressivelyincrease.1---8Thistrendwas
identifiedinthestudybyBernardetal.,9withadolescents
fromSãoPaulo.The authorsobservedthattheprevalence
ofshortsleepdurationwas5%at10yearsofage,14%at12
years,reaching59%attheendofadolescence.
Recentstudieshavebeentryingtounderstandwhich
fac-tors are associated with the reduction of sleep hours in
adolescence.3,8,10---12 Inthiscontext,some biological
varia-bles,aswellassocialandbehavioralones,areanalyzedin
ordertobetterunderstandtheexpressionofthesleep/wake
cycleatthisstageoflife.Thisissuebecomesmoreimportant
astheshortsleepduration,particularlyduringadolescence,
isassociatedwithcognitivedeficitsanddecreaseinhealth
status.13---15
Consideringthenegativeeffectsofshortsleepduration
inadolescentsandthefewpopulation-basedstudiesfound
inBrazil,especiallyinsmallmunicipalities,thisstudyaimed
toinvestigate the prevalence and factorsassociated with
shortsleepdurationinadolescentsfromthemunicipalityof
Maravilha,inthestateofSantaCatarina,southernBrazil.
Method
Thesampleconsistedof516adolescents(263males),with ameanageof14.57(1.77)years.Thissamplewasbasedon apopulationof2969adolescentsaged10---19years,ofboth genders,regularlyenrolledinpublicschoolsinthe munici-palityofMaravilha,stateofSantaCatarina,southernBrazil in2013.16
The sample sizewasdefinedusingthe proposalofLuiz
andMagnanini,17 considering asampling error offive
per-centagepointsand1.5forthedesigneffect.Basedonthis
calculation,a minimumof513 adolescentswasestimated
toconstitutea representativeschool-based sample inthe
municipality.Sample selection was performed by clusters
and proportional to the age groups of 10---14 and 15---19
years,takingintoaccountthepopulationofstudentsinthe
finalyearsofelementaryschooland inthethreeyearsof
highschool.
The adolescents answered a structured questionnaire
containingquestionson thefollowing factors:
sociodemo-graphic,relatedtosleepandhealth.
As for sociodemographic factors, the following were
assessed:gender, age,placeofresidence(ruralorurban),
schoolshift(morning,afternoonandevening),income
(min-imumwagesreceivedby thefamily) andschoolingof the
householdhead. Regarding income, the adolescentswere
classifiedaslow income(upto3 minimumwages ---MW),
middleincome(3---6MW)andhighincome(morethan6MW).
Regarding factors related tosleep, the following data
wereanalyzed: sleepdurationwasevaluatedaccording to
thetimein bed, based onthetimes when goingto sleep
andwaking up on school days.The adolescentswith less
than8hadayinbedwereconsideredashavingshortsleep
duration.3,9,18 Additionally, the time when going to sleep
andwakingupwereinvestigatedconsidering specific days
oftheweek:fromMondaytoThursday,fromFridayto
Sat-urday,fromSaturdaytoSunday,andfromSundaytoMonday.
Thedifficultyinfallingasleepwasinvestigatedthroughthe
question‘‘Do you have difficulty infalling asleep?’’, with
thefollowing responseoptions: (a) never, (b) sometimes,
(c)always.3
DaytimesleepinesswasassessedusingthePediatric
Day-timeSleepinessScale(PDSS).19 Thisscale consistsof eight
multiple-choicequestions.Eachquestionhasfiveresponse
options, using a Likert scale: 0=never; 1=almost never;
2=sometimes;3=frequentlyand4=always.Attheend,
ques-tionscoresweresummed,withthescalescorerangingfrom
zeroto32.Highscores indicatemoredaytimesleepiness.
Astherearenoclassificationsforthisscale,theadolescents
were allocated considering the tertiles. Thus, those
ado-lescentsat the third tertile (highest scoreof PDSS)were
classifiedashavingmoredaytimesleepiness.
Chronotype wasinvestigated usingthe Munich
Chrono-type Questionnaire (MCTQ).20 In this questionnaire, the
chronotypedefinitionisgivenasaphaseofthesleep/wake
cycle,representedbythecorrectedhalf-sleepphase,also
consideringthefreedays.ThechronotypeinMCTQisgiven
themorningness,whilehighervaluesrepresenteveningness.
Theadolescentsweredividedintotertilesconsideringthe
MCTQ score,withthefirsttertile representing thosewith
morningbehavior.
Finally, regarding health-related factors, the
percep-tionof health and stress, weight status, physical activity
level and time in sedentary behaviors were investigated.
Sedentarybehavior wasinferredby thetimespent inthe
sitting position, which was investigated by the question
‘‘How long do you usually spend in the sitting position
ona weekday?’’.21 This question was extracted fromthe
‘‘InternationalPhysicalActivityQuestionnaire’’and
consid-ers in its analysis the time during which the adolescents
remainseatedduringtheday,atwork,atschoolorcollege,
athomeandduringtheirfreetime,includingthetimespent
studying,resting,doinghomework,visitingafriend,
read-ing,sittingor lyingdownwhile watching TV.Thisanalysis
doesnotincludethetimespentsittingduringtransportby
bus,train,subwayorcar.Asintheanalysisofsleepinessand
chronotype,thespecializedliteraturedoesnothavea
spe-cificcutoffforthelongorshorttimeofsedentarybehavior.
Therefore,thestrategyof usingtertileswasalsoadopted
forthisvariable.
The subjective perception of adolescents’ health was
investigated through the question: ‘‘How do you classify
your current health status?’’. For this question, a
pos-itive health perception was considered for the answers
‘‘excellent’’and‘‘good’’,andanegativehealthperception
fortheanswers‘‘regular’’and‘‘bad’’.22
Thissamestrategy wasadopted toinvestigatethe
per-ception of stress, which was inferred by the question:
‘‘Howwouldyoudescribethelevelofstressinyourlife?’’.
The following response options were considered: rarely
stressed(livingverywell);sometimesstressed(livingfairly
well);oftenstressed(oftenfacingproblems)andexcessively
stressed (difficulty to cope with daily life). Adolescents
that answered the question with the alternatives ‘‘often
stressed’’and ‘‘excessively stressed’’were considered as
havingahigh-stressperception.
Asfor theweightstatusvariable,heightwasmeasured
usinga stadiometer, fixed verticallyon the wall,and the
body mass was measured using a digital scale with 100
g of precision, following the recommended measurement
proceduresby Alvarezand Pavan.23 The bodymass index
(BMI)wasobtainedfromtheratiobetweenbodymass(kg)
and squared height (m). The categorization of this
vari-ablewascarried outconsidering thecriteria proposedby
theInternationalObesityTaskForce, byageandgender,24
complementedby scores indicative of low weight in Cole
et al.24,25 Weight status wascategorized as underweight,
normalweight,overweightandobesity.
The level of physical activity wasinvestigated through
thequestionnaireproposed byFlorindo etal.26 This
ques-tionnaire consists of 17 questions on habitual physical
activity,consideringthetotaltimein minutesandweekly,
and was validated considering the cardiorespiratory
fit-ness.Theadolescentswereclassifiedasinsufficientlyactive
if they performed less than 300 min of weekly physical
activity.27
Descriptiveanalyseswereperformed(means,frequency
and standard deviations). The Kolmogorov---Smirnov test
indicatedthattheanalyzeddatawerenonparametric.Thus,
the Kruskal---Wallis test was used to compare continuous
variables, whereas the Chi-square test was used to
ver-ify the association between proportions. Due tothe high
prevalenceobservedofshortsleepduration,Poisson
regres-sion was carried out to investigate associations between
thevariables.28 The adjusted modelconsidered the
varia-blesgender,agerange,schoolshift,familyincome,daytime
sleepiness,napsandtimespentinthesittingpositionwith
p<0.25inthecrudeanalysis.29Consideringthisanalysis,the
followingvariableswereexcludedfromtheadjustedmodel:
placeofresidence,chronotypeandphysicalactivity.A
sig-nificancelevelof5%wasconsideredforallanalyses.
TheInformedConsentformwasgiventoalladolescents
youngerthan18tobesignedbyparents/guardians,andall
adolescents involved in the study received the Informed
Assent form. The project was evaluated by the
institu-tion’s Institutional Review Board, according to Edict N.
535,621/2013.
Results
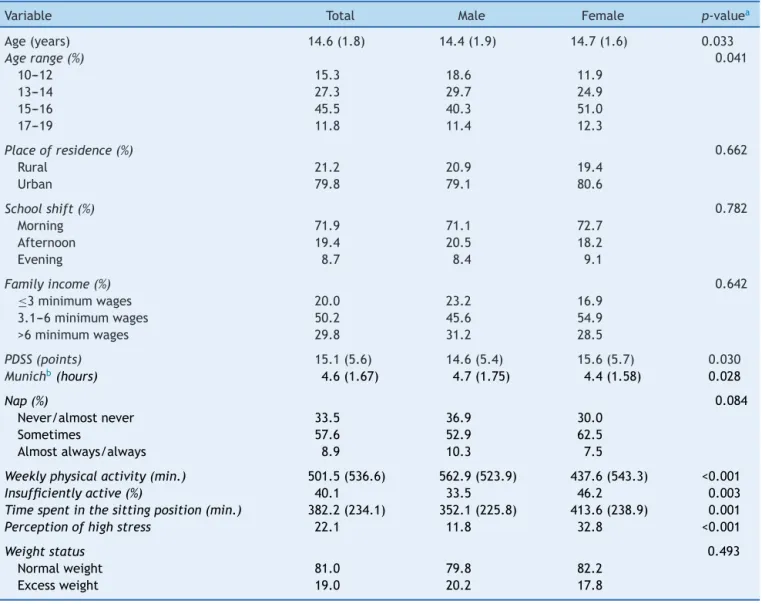
ThesampledescriptivedataareshowninTable1.The
inves-tigated adolescentswere,onaverage,14.6±1.7yearsold
and most of them lived in the urban area of the
munici-pality.Theassessedadolescentsremainedameanof382.2
minadayinthesittingposition,andthefemaleadolescents
spentmoretimethanmalesinthisbehavior(p=0.001).The
girls had lowerlevelsof physical activity (p=0.003) and a
higherprevalenceofexcessivestressperception(p<0.001)
whencomparedtoboys.
Meansleepduration was7.9±1.6 hand nodifferences
wereidentifiedbetweengenders(p=0.216).Theprevalence
ofshortsleepduration(lessthan8h)was53.6%,with
differ-encesbetweenagegroups(p<0.001).Sleepdurationduring
adolescenceandondifferentdaysoftheweekisshownin
Figs.1and2.
Fig. 2 shows a trend of decreasing hours of sleep
throughoutadolescence.Whiletheprevalenceofshortsleep
duration at 10---12 years was 31.2%, in the age group of
17---19yearstheprevalenceincreasedto70%.Additionally,
asshownin Fig.2,the adolescentstended tohave longer
sleepdurationduringtheweekend.
Table 2 shows the association analysis between short
sleepdurationandtheindependentvariables.Theadjusted
analysis showed that the age range variablewas strongly
associatedwiththeoutcome.Therefore,adolescentsaged
15---16and17---19hadrespectively;1.71-(95%CI:1.09---2.69)
and2.05-fold(95%CI:1.20---3.50)higherprevalenceofshort
sleepduration,whencomparedtotheagegroupof10---12
years.
Anotherfactorstronglyassociatedwithshortsleep
dura-tion wastheschool shift. Adolescents whostudied in the
morningshifthad1.82-fold(95%CI:1.35---2.46)higher
preva-lenceofshortsleepduration,whencomparedtostudents
in the afternoon shift. In the adjusted analysis,
adoles-centswhostudiedintheeveningshifthad1.68-fold(95%CI:
1.14---2.46)higherprevalenceofshortsleepdurationin
rela-tiontoadolescentswhostudiedintheafternoonshift.
Althoughdaytimesleepiness,nappingandtimeinthe
sit-tingpositiondidnotremainassociatedwiththeoutcomein
Table1 Descriptivedataofthesamplewithdifferencesbetweengenders.
Variable Total Male Female p-valuea
Age(years) 14.6(1.8) 14.4(1.9) 14.7(1.6) 0.033
Agerange(%) 0.041
10---12 15.3 18.6 11.9
13---14 27.3 29.7 24.9
15---16 45.5 40.3 51.0
17---19 11.8 11.4 12.3
Placeofresidence(%) 0.662
Rural 21.2 20.9 19.4
Urban 79.8 79.1 80.6
Schoolshift(%) 0.782
Morning 71.9 71.1 72.7
Afternoon 19.4 20.5 18.2
Evening 8.7 8.4 9.1
Familyincome(%) 0.642
≤3minimumwages 20.0 23.2 16.9
3.1---6minimumwages 50.2 45.6 54.9
>6minimumwages 29.8 31.2 28.5
PDSS(points) 15.1(5.6) 14.6(5.4) 15.6(5.7) 0.030
Munichb(hours) 4.6(1.67) 4.7(1.75) 4.4(1.58) 0.028
Nap(%) 0.084
Never/almostnever 33.5 36.9 30.0
Sometimes 57.6 52.9 62.5
Almostalways/always 8.9 10.3 7.5
Weeklyphysicalactivity(min.) 501.5(536.6) 562.9(523.9) 437.6(543.3) <0.001
Insufficientlyactive(%) 40.1 33.5 46.2 0.003
Timespentinthesittingposition(min.) 382.2(234.1) 352.1(225.8) 413.6(238.9) 0.001
Perceptionofhighstress 22.1 11.8 32.8 <0.001
Weightstatus 0.493
Normalweight 81.0 79.8 82.2
Excessweight 19.0 20.2 17.8
PDSS,PediatricDaytimeSleepinessScale.
a p-valueofChi-squareorKruskal---Wallis. b ChronotypeaccordingtoMunich’sclassification.
withshortsleepduration.Adolescents atthe thirdtertile of the sleepiness scale had 1.26-fold (95%CI: 1.03---1.56) higherprevalenceofshortsleepdurationthantheonesat the firsttertile. Nappingwas associatedwith lowersleep
0 3 6 9
10 to 12 13 to 14
Age ranges (years)
17 to 19 15 to 16
Sleep duration (hours)
Figure1 Sleepdurationdecreasewithincreasingage.
duration in the ‘‘sometimes’’ category (PR=1.26; 95%CI: 1.04---1.54)andinthe‘‘always’’category(PR=1.50;95%CI: 1.16---1.95), indicating that adolescents with shorter noc-turnal sleep more frequently napped. The time spent in
Mon/Thur 7
7.5 8 8.5 9 9.5
Boys Girls
Sat/Sun
Weekdays
Sleep duration (hours)
Fri/Sat Sun/Mon
Table2 Poissonregressionanalysisconsideringshortsleepdurationasthedependentvariable.
Variable Prevalence(%) Unadjustedanalysis Adjustedanalysis
PR(95%CI) PR(95%CI)
Gender
Male 51.0 1 1
Female 56.4 1.10(0.94---1.30) 1.02(0.80---1.32)
Agerange
10---12 31.2 1 1
13---14 46.8 1.50(1.03---2.18) 1.46(0.91---2.34)
15---16 60.9 1.95(1.38---2.76) 1.71(1.09---2.69)
17---19 70.0 2.24(1.55---3.25) 2.05(1.20---3.50)
Placeofresidence Excluded
Rural 48.5 1
Urban 54.9 1.13(0.91---1.41)
Schoolshift
Morning 58.3 1.82(1.35---2.46) 1.59(0.93---2.71)
Afternoon 32.0 1 1
Night 63.6 1.98(1.38---2.86) 1.68(1.14---2.46)
Familyincome
≤3minimumwages 49.3 1 1
3.1---6minimumwages 51.9 1.05(0.85---1.29) 1.03(0.76---1.39)
>6minimumwages 60.9 1.23(1.00---1.53) 1.19(0.86---1.64)
PDSS
1sttertile 47.1 1 1
2ndtertile 54.7 1.16(0.95---1.43) 1.05(0.77---1.41)
3rdtertile 59.7 1.26(1.03---1.56) 1.10(0.79---1.52)
Chronotype Excluded
1sttertile 51.9 1
2ndtertile 50.3 0.97(0.78---1.19)
3rdtertile 57.7 1.14(0.91---1.36)
Nap
Never/almostnever 44.8 1 1
Sometimes 56.7 1.26(1.04---1.54) 1.13(0.86---1.49)
Almostalways/always 67.4 1.50(1.16---1.95) 1.23(0.79---1.92)
Physicalactivity Excluded
Active 51.9 1
Insufficientlyactive 56.2 1.08(0.92---1.27)
Timespentinthesittingposition
1sttertile 47.3 1 1
2ndtertile 57.1 1.20(1.00---1.47) 1.01(0.74---1.38)
3rdtertile 61.2 1.29(1.07---1.57) 1.09(0.80---1.49)
PDSS,PediatricDaytimeSleepinessScale.
thesittingpositionshowedassociationsin thesecond ter-tile (OR=1.20; 95%CI: 1.00---1.47) and in the third tertile (OR=1.29; 95%CI: 1.07---1.57), indicating that adolescents whospent more time in sedentary behaviors had shorter durationofsleepatnight.
Discussion
Thisstudy showedevidenceofassociationsbetween short sleep duration and the adolescents’ school shift and age range.Theprevalenceofshortsleepdurationwasof53.6%
among the assessed adolescents. This prevalence is high comparedtootherstudies.3,9,12,30 Althoughtheprevalence
was high, higher percentages were observed in
North-American adolescents.11 It is worth mentioning that the
municipalityofMaravilha---SCissmallandhasahigh
per-centage of rural population, and this prevalence was not
expected.
Adolescentswithshortsleepdurationshowan increase
in several health risks. Javaheri et al.31 warn that short
sleepdurationand thepoor qualityofsleepare,in many
cases, associatedwith increasedpresence of pathologies.
duration andincreased presence of stress in adolescents.
Furthermore,asseen inthe studyby Nova etal.,12
Span-ishadolescentswithadequate sleepdurationhada lower
incidenceofallergies.
Therewasatrendofincreasedprevalenceofshortsleep
durationthroughoutadolescence.Asdescribedinthe
liter-ature,ageisstronglyassociatedwithshortsleepduration,
considering the maturation of thecentral nervoussystem
and risk behaviors, suchas usingelectronic media,
espe-cially at night.10,32 In adolescence, individuals are more
likelytohaveabiologicalphenomenoncalleddelayed
sleep-phase, in which adolescents tend to sleep and wake up
at late hours,33 which may contribute to increased
day-timesleepiness,ifsleepisnotrecovered duringtheday.32
Moreover,thisbiologicaltendencyisexacerbatedbycertain
behaviors which, added to early morning school
commit-ments,markedlyincrease thenumberofadolescentswith
shortsleepduration.4
Duetotheaforementionedreasons,itcanbeemphasized
thattheadolescentsattendingdaytimeandnighttimeschool
shifts showed a higher association with short sleep
dura-tion.Older adolescentsandthosestudying at theseshifts
constitute a majorrisk group for shortsleep duration. In
the study by McKnight-Eily et al.,11 the authors propose,
to diminish the high prevalence of short sleep duration,
individualobservationofadolescents,indicatingchangein
behavior and eventhe change of the school shift. In this
context,LouzadaandMenna-Barreto34discussthe
possibil-ityof starting classes at a later hourin the morningas a
possibleintervention.However,thesameauthorshighlight
thedifficultyforschoolstoadopttheserecommendations,
considering the working hours of parents and even the
cultureofvaluingactivitiesthatstartearlyinthemorning.
Itwasobservedthatthehighestfrequencynappingwas
associatedwithshortsleepdurationinadolescents.
Proba-bly,adolescentswhomorefrequentlynapusethishabitasa
waytocompensatefortheshortdurationofnocturnalsleep.
ThisresultcorroboratesthefindingsofBernardetal.,9who
also found a higherprevalence of shortsleep durationin
adolescentswitha higherfrequency of napping.Although
thishabitrepresentsawaytocompensateforsleepdeficit,
according to Carskadon et al.,2 it can delay the
propen-sitytonighttimesleep,delayingitsonsetandreducingits
duration.Therefore,itisnecessary toinvestigatenapping
dose-response,considering itsfrequency andduration,for
possiblerecommendationstoadolescents.
Finally, it is noteworthy that adolescents withshorter
sleepdurationhadhighertimeofsedentarybehavior.Thus,
astheliteratureindicatesanincreasingprevalenceofshort
sleepduration,itisalsopossibletoidentifythatadolescents
spendmoretimeinsedentarybehaviors,especiallyinfront
oftheTVandattheinternet.35,36 Itisthereforenecessary
toinvestigatewhetherthoseadolescentswithshortersleep
durationpreferto spendmore timein activitieswithlow
energyexpendituredueto,forinstance,excessivedaytime
sleepiness.
Positives pointsof this study can be highlighted, such
as, theuse ofa representativesample of asmalltownin
the countryside, rarely studied, aswell asthe discussion
ofassociationsnotavailableinthenationalliterature.The
main limitationofthis studyis theuse ofaquestionnaire
toindirectlyassesstheissuesofsleepandphysicalactivity,
whicheventhougharevalidatedtools,mayleadto
under-estimatedoroverestimatedmeasuresbytheadolescents.
The adolescents from Maravilha --- SC showed a high
prevalence ofshort sleepduration,and the older
adoles-centsandtheoneswhostudiedinthemorningandevening
schoolshiftsshowedreducedsleepduration.Thisresult
indi-catestheneedforactionsaimedatschoolchildren’shealth
focused on biological and behavioral profiles at different
stagesofadolescence.Inthisrespect,itisworth
mention-ingthattheadolescentmaynotnoticechangesintheirsleep
patterns,andthuseducationalmeasuresareimportantsince
thestartoftheelementaryschool,helpingthemtoestablish
andmaintainadequatesleephygiene.Inthissense,itis
rec-ommendedthatclassesshouldbeofferedintheafternoon
forallschoolyearsandeventhecreationofanintermediate
shiftstartingatmidmorning.
Eventhoughageandschoolshiftwerethefactorsmost
stronglyassociatedwithshortsleepduration,thehabitof
napping, sedentary behaviors and daytime sleepiness are
important variables that must be considered in the short
sleepdurationanalysis.Thus,itisrecommendedtoperform
studiesthatwillprovideknowledgeonthecausal
associa-tionsbetweenthesevariablesandtoindicate,withhigher
precision,theadequate nappingtime,sothatthe
adoles-centwillnothavelossofnocturnalsleep.Itisalsoessential
toproposewaystominimizetheeffectofsleepdeprivation
onincreaseddaytimesleepinessandtimespentinsedentary
behaviors,consideringtheadolescent’sreality.
Funding
Thestudyreceivednofunding.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
References
1.Borges GA, Schwarztbach C. Idade da menarca em adoles-centesdeMarechalCândidoRondon-PR.RevBrasCineantropom DesempenhoHum.2003;5:15---21.
2.CarskadonMA,VieiraC,AceboC.Associationbetweenpuberty anddelayedphasepreference.Sleep.1993;16:258---62. 3.PereiraÉF,TeixeiraCS,LouzadaFM.Sonolênciadiurna
exces-sivaemadolescentes:prevalênciaefatoresassociados.RevPaul Pediatr.2010;28:98---103.
4.Moore M, Meltzer LJ. The sleepy adolescent: causes and consequences of sleepiness in teens. Paediatr Respir Rev. 2008;9:114---21.
5.Levy D,Gray-Donald K, Leech J, Zvagulis I, Pless IB. Sleep patternsandproblemsinadolescents.JAdolescHealthCare. 1986;7:386---9.
6.HicksRA,PellegriniRJ.Thechangingsleephabitsof college-students.PerceptMotSkills.1991;72:1106.
7.MontagnerH,DeRoquefeuilG,DjakovicM.Biological, behav-ioral andintellectualactivity rhythmsofthechildduringits developmentindifferenteducationalenvironments.In:Biologic rhythmsinclinicalandlaboratorymedicine;1992.p.214---29. 8.ChenMY,WangEK,JengYJ.Adequatesleepamongadolescents
9.BernardoMP,PereiraEF,LouzadaFM,D’AlmeidaV.Durac¸ãodo sonoemadolescentesdediferentesníveissocioeconômicos.J BrasPsiquiatr.2009;58:231---7.
10.Pereira ÉF, Teixeira CS, Andrade RD, Bleyer FT, Lopes AS. Associac¸ãoentreoperfildeambienteecondic¸õesdetrabalho comapercepc¸ãodesaúdeequalidadedevidaemprofessores deeducac¸ãobásica.CadSaudeColet.2014;22:113---9. 11.McKnight-Eily LR, Eaton DK, Lowry R, Croft JB,
Presley-Cantrell L, Perry GS. Relationships between hours of sleep andhealth-riskbehaviorsinUSadolescentstudents.PrevMed. 2011;53:271---3.
12.NovaE,Martínez-GómezD,Gómez-MartínezS,etal.Influence ofhealthbehavioursontheincidenceofinfectionandallergy in adolescents:theAFINOS cross-sectional study.BMC Public Health.2014;14:19.
13.Tomás Vila M, Miralles Torres A, Beseler Soto B, Revert Gomar M, Sala Langa M, Uribelarrea Sierra A. Attention-deficit/hyperactivitydisorderand sleepdisturbances.Results ofanepidemiologicalstudyinschoolchildreninGandia,Spain. AnPediatr(Barc).2008;69:251---7.
14.Anacleto TS, Louzada FM, Pereira ÉF. Ciclo vigília/sono e o transtornodedéficitdeatenc¸ão/hiperatividade.RevPaul Pedi-atr.2011;29:437---42.
15.SoaresCS,deAlmondesKM.Sonoecognic¸ão:implicac¸õesda privac¸ãodosonoparaapercepc¸ãovisualevisuoespacial.Psico. 2012;43:85---92.
16.Brasil--- InstitutoBrasileirodeGeografiaeEstatística.Síntese de indicadores sociais; 2010. Available from: http://www. ibge.gov.br/home/estatistica/populacao/condicaodevida/ indicadoresminimos/sinteseindicsociais2010/SIS2010.pdf
[accessed08.04.15].
17.LuizRR,MagnaniniMM.Alógicadadeterminac¸ãodotamanho daamostraeminvestigac¸õesepidemiológicas.CadSaudeColet. 2000;8:9---28.
18.Perez-ChadaD,Perez-LloretS,VidelaAJ,etal.Sleepdisordered breathinganddaytimesleepinessareassociatedwithpoor aca-demic performanceinteenagers.Astudyusingthepediatric daytimesleepinessscale(PDSS).Sleep.2007;30:1698---703.
19.Drake C, Nickel C, Burduvali E, Roth T, Jefferson C, Badia P. The pediatric daytime sleepiness scale (PDSS): Sleep habitsand schooloutcomesinmiddle-schoolchildren.Sleep. 2003;26:455---8.
20.RoennebergT,Wirz-JusticeA,MerrowM.Lifebetweenclocks: dailytemporalpatternsofhumanchronotypes.JBiolRhythms. 2003;18:80---90.
21.Pardini R, Matsudo S, Araújo T, et al. Validac¸ão do ques-tionáriointernacionaldeníveldeatividadefísica(IPAQ-versão 6):estudopilotoemadultosjovensbrasileiros.RevBrasCien MovBrasília.2001;9:39---44.
22.Geiger SD, Sabanayagam C, Shankar A. The relation-ship between insufficient sleep and self-rated health in a nationally representative sample. J Environ Public Health. 2012;2012:518263.
23.AlvarezBR,PavanAL,PetroskiE.Alturasecomprimentos.In: PetroskiEL,editor.Antropometria:técnicasepadronizac¸ões, vol.3,4thed.Blumenau:NovaLetra;2007.p.31---44.
24.Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standarddefinitionforchildoverweightandobesityworldwide: internationalsurvey.BMJ.2000;320:1240.
25.ColeTJ,FlegalKM,NichollsD,JacksonAA.Bodymassindexcut offstodefinethinnessinchildrenandadolescents:international survey.BMJ.2007;335:194---7.
26.Florindo AA, Romero A, Peres SV, Silva MV, Slater B. Development and validation of a physical activity assess-ment questionnaire for adolescents. Rev Saude Publica. 2006;40:802---9.
27.PateRR,FreedsonPS,SallisJF,etal.Compliancewithphysical activityguidelines:prevalenceinapopulationofchildrenand youth.AnnEpidemiol.2002;12:303---8.
28.BarrosAJ,Hirakata VN.Alternativesforlogistic regressionin cross-sectionalstudies:anempiricalcomparisonofmodelsthat directlyestimatetheprevalenceratio.BMCMedResMethodol. 2003;3:21.
29.HosmerDW,LemeshowS.Appliedlogisticregression.Hoboken: JohnWiley&Sons;2004.
30.TagayaH,UchiyamaM,OhidaT, etal. Sleephabitsand fac-tors associated with short sleep duration among Japanese high-schoolstudents:acommunitystudy.SleepBiolRhythms. 2004;2:57---64.
31.JavaheriS, Storfer-IsserA, Rosen CL,RedlineS. Sleep qual-ity and elevated blood pressure in adolescents. Circulation. 2008;118:1034---40.
32.Zavada A, Gordijn MC, Beersma DG, Daan S, RoennebergT. ComparisonoftheMunich chronotypequestionnairewiththe Horne---Ostberg’s Morningness---Eveningness score. Chronobiol Int.2005;22:267---78.
33.CrowleySJ,AceboC,CarskadonMA.Sleep,circadianrhythms, and delayed phase in adolescence. Sleep Med. 2007;8: 602---12.
34.LouzadaF,Menna-BarretoL. O sono nasalade aula: tempo escolar e tempo biológico. Rio de Janeiro: Vieira e Lent; 2007.
35.Oehlschlaeger MH,PinheiroRT,Horta B,Gelatti C,San’Tana P.Prevalenceofsedentarismanditsassociatedfactorsamong urbanadolescents.RevSaudePublica.2004;38:157---63.