w w w . r b o . o r g . b r
Original
Article
Low-term
results
from
non-conventional
partial
arthroplasty
for
treating
rotator
cuff
arthroplasthy
夽
Antônio
Carlos
Tenor
Júnior
∗,
José
Alano
Benevides
de
Lima,
Iúri
Tomaz
de
Vasconcelos,
Miguel
Pereira
da
Costa,
Rômulo
Brasil
Filho,
Fabiano
Rebouc¸as
Ribeiro
OrthopedicsandTraumatologyService,HospitaldoServidorPúblicoEstadualdeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received29January2014 Accepted5June2014 Availableonline23April2015
Keywords:
Replacementarthroplasty Shoulder
Rotatorcuff
a
b
s
t
r
a
c
t
Objective:ToevaluatetheevolutionofthefunctionalresultsfromCTA®hemiarthroplasty forsurgicallytreatingdegenerativearthroplathyoftherotatorcuff,withameanfollow-up of5.4years.
Methods:EighteenpatientswhounderwentCTA®partialarthroplastytotreatdegenerative arthroplathyoftherotatorcuffbetweenApril2007andJune2009werereevaluated,with minimumandmeanfollow-upsof4.6yearsand5.4years,respectively.Preand postopera-tiveparametersforfunctionalityandpatientsatisfactionwereused(functionalscaleofthe UniversityofCaliforniainLosAngeles,UCLA).Allthepatientsunderwentprior conserva-tivetreatmentfor6monthsandunderwentsurgicaltreatmentbecauseoftheabsenceof satisfactoryresults.Patientswereexcludediftheypresentedanyofthefollowing:previous shouldersurgery;pseudoparalysis;insufficiencyofthecoracoacromialarch(type2Bin See-bauer’sclassification);neurologicallesions;orinsufficiencyofthedeltoidmuscleandthe subscapularismuscle.
Results:Withameanfollow-upof5.4years,14patientsconsideredthattheyweresatisfied withthesurgery(78%);themeanrangeofjointmotionforactiveelevationimprovedfrom 55.8◦beforetheoperationto82.0◦aftertheoperation;themeanexternalrotationimproved from18.9◦beforetheoperationto27.3◦aftertheoperation;andthemeanmedialrotation remainedatthelevelofthethirdlumbarvertebra.ThemeanUCLAscoreafterthemean follow-upof5.4yearswas23.94andthiswasanimprovementincomparisonwiththe preoperativemeanandthemean1yearaftertheoperation.
Conclusion:Thefunctional resultsfrom CTA® hemiarthroplastyfortreating rotator cuff arthroplastyinselectedpatientsremainedsatisfactoryafterameanfollow-upof5.4years. ©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkdevelopedintheShoulderandElbowGroup,StatePublicServants’Hospital,SãoPaulo,SP,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](A.C.TenorJúnior). http://dx.doi.org/10.1016/j.rboe.2015.04.006
Resultados
em
longo
prazo
da
artroplastia
parcial
não
convencional
para
o
tratamento
da
artroplastia
do
manguito
rotador
Palavras-chave:
Artroplastiadesubstituic¸ão Ombro
Manguitorotador
r
e
s
u
m
o
Objetivo:Avaliaraevoluc¸ãodoresultadofuncionaldahemiartroplastiaCTA®notratamento cirúrgicodaartropatiadegenerativadomanguitorotadorcomumseguimentomédiode5,4 anos.
Métodos: Foramreavaliados18 pacientessubmetidosàartroplastiaparcialCTA® parao tratamentodaartropatiadegenerativadomanguitorotadorentreabrilde2007ejunhode 2009,comseguimentomínimoemédiode4,6anose5,4anos,respectivamente.Foram usa-dosparâmetrospréepós-operatóriosdefuncionalidadeesatisfac¸ãodospacientes(escala funcionaldaUniversidadedaCalifórniaemLosAngeles[UCLA]).Todosospacientesfizeram tratamentoconservadorprévioporseismeseseforamsubmetidosaotratamentocirúrgico naausênciaderesultadosatisfatório.Foramexcluídospacientescomcirurgiapréviano ombro,pseudoparalisia,insuficiênciadoarcocoracoacromial(tipo2Bdaclassificac¸ãode Seebauer),lesãoneurológicaouinsuficiênciadomúsculodeltoideedomúsculo subescapu-lar.
Resultados:Comumseguimentomédiode5,4anos,14pacientesseconsideravamsatisfeitos comacirurgia(78%).Aamplitudedemovimentoarticularmelhorounaelevac¸ãoativamédia evarioude55,8◦nopré-operatóriopara82◦nopós-operatório.Arotac¸ãoexternamédia melhoroudeemmédia18,9◦nopré-operatóriopara27,3◦nopós-operatório.Amédiada rotac¸ãomedialmanteve-senoníveldaterceiravértebralombar.OescoreUCLAmédio, apósseguimentomédiode5,4anos,foide23,94emelhorouemcomparac¸ãocomasmédias pré-operatóriaedoprimeiroanopós-operatório.
Conclusão: OsresultadosfuncionaisdahemiartroplastiaCTA®notratamentoda artroplas-tiadomanguitorotadorempacientesselecionadosmantiveram-sesatisfatóriosapósum seguimentomédiode5,4anos.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Thefirstauthortodescribetheclinicalfindingsfrom arthropa-thyoftherotatorcuffwas RobertAdams,in1857.In1981, Halverson et al.1 described the “Milwaukee shoulder”, in whichcrystalsofcalciumphosphatesuchashydroxyapatite wereinvolvedinacellularreactionwithreleaseof collage-nasesand jointdestruction.However,Neerwasthefirst to usetheterm“arthropathyofthe rotatorcuff”,in1977,ina studypublishedin1983.2Neerbelievedthatextensiveinjury totherotatorcuffwasthecauseofthearthropathyand pre-sentedthehypothesisthatthispathologicalconditionmight bethe resultofmechanical factors suchasanterosuperior instability,andnutritionalfactorssuchaslossoftheclosed jointspace,withimpairmentofnutrientdiffusiontothejoint surface.Interruptionofthebonecirculationthatisprovided bytherotatorcuffalsocontributestowardthemetabolicloss atthe humeralhead. Thefinal resultfromthese mechani-calandmetabolicalterations,inassociationwithosteopenia throughdisuseoftheglenohumeraljointduetopain,consists ofcollapseoftheglenohumeraljoint.1–4
Morerecently,in1997,CollinsandHarryman5produceda synthesisfromthetwotheoriesandformulatedthe hypothe-sisthatcranialmigrationofthehumeralhead,resultingfrom lossofthe stability thatthe rotator cuffprovides, leads to
abnormalglenohumeralcontactandformationofdebrisinthe joint.Thus,aninflammatorycascadecausedbythecalcium phosphatecrystalsthatarereleasedisdeveloped.
Theincidenceofrotatorcuffinjuriesincreaseswithage. They arerelatively rarebeforethe ageof40 years,become morefrequentinthefifthandsixthdecadesoflifeand con-tinuetoincrease intheseventh decade andbeyond. Many casesdonotpresentsymptomsandapproximately50%ofall individualsovertheageof80yearsmayhaveasymptomatic rotatorcuffinjuries.6,7
degenerativearthropathy,andproposedaclassification sys-temconsistingoffiveevolutionarystages.However,thesedo notguidethetherapy.
Seebauer12 developed a biomechanical, functional and morphologicalclassificationsystemthatpresentstherapeutic relevanceand assessesthe integrityoftheanterior stabili-zersoftheshoulderandcoracoacromialarch,thepresence ofdynamicstabilityandtheupwardmigrationofthehumeral head.Additionalexaminations,suchascomputed tomogra-phyandmagneticresonanceimaging,arenotnecessaryfor diagnosing arthropathy of the rotator cuff, but they help in making preoperative assessments to analyze the bone stock and the conditions ofthe rotator cuff, suchas fatty degeneration.12–14
Treatmentsforarthropathyoftherotatorcuffshouldbe startedusingnon-surgicalmethods,suchasmodificationof activities,useofanalgesicand/oranti-inflammatory medica-tionsanduseofsubacromialcorticosteroidinfiltration.6,15
Surgical treatment is indicated for patients who do notrespondtoconservative treatment. Proceduressuchas arthroplastytoresect thehumeral headand glenohumeral arthrodesisareconsideredtobesalvagemethods,tobeusedin patientspresentingmultiplesurgicalfailures,deficiencyofthe deltoidmuscleandinfection.Arthroscopyfordebridement, tenotomyofthebicepsandtuberculoplastycanbeperformed, particularlyinelderlypatientsandthosewithlowfunctional demands.Conventionaltotalarthroplastyoftheshoulderis nowcontraindicatedinpatientspresentingarthropathyofthe rotatorcuffbecauseofthehighrateoflooseningoftheglenoid component.Thecurrentalternativearthroplastyoptionsfor arthroplastyoftherotatorcuffarenon-conventional(CTA®)
partialarthroplastyanduseofareverseprosthesis.3,16–18 CTA® partialarthroplastypresents greaterlateral extent
with coverage ofthe tubercleand produces better contact andconnectionwiththecoracoacromialarch(Figs.1and2). Reverse prostheses are based on the concepts ofGramont etal.,19involvingmovingthecenterofrotationmediallyand distally,withgainsindeltoidmusclefunction.Thisprinciple
Fig.1–CTAprosthesiswithitslateralextent,shownon
intraoperativephototakenbytheauthor.
Fig.2–CTAprosthesisshownonpostoperativeradiograph
producedbytheauthor.
improvedthestabilityoftheimplantandtherangeofmotion. Nonetheless,despitethegoodresultsfromreverseprostheses, thisisatechnicallymorecomplexprocedurewithhigher com-plicationrates(5%to33%).CTA® hemiarthroplastypresents
goodresultsinselectedpatients,withlowerincidenceof com-plicationsthanthatofreverseprostheses.3,20–24
Patients who are candidatesfor CTA® hemiarthroplasty
needtobefreefrompseudoparalysis,presenta coracoacro-mial arch that maintains the relative kinematics of the shoulderjoint,withoutanterosuperiorescape(Seebauertypes IA,IBandIIA),absenceofprevioussurgeryinvolvingresection ofthecoracoacromialarch,functioningmotor(intactdeltoid) andsufficientsubscapularmuscle.3,25–28
Theobjectiveofthisstudywastoevaluatetheevolutionof thefunctionalresultsfromCTA®partialarthroplastyfor
sur-gicallytreatingdegenerativearthropathyoftherotatorcuff, afterameanfollow-upof5.4years.
Methods
Between December 2006 and June 2009, 23 shoulders of 23 patients underwent CTA® partial arthroplasty to treat
arthropathyoftherotatorcuff.Duringameanfollow-upof1.6 years,therewereimprovementsintheclinicalparametersand UCLAscore,asdescribedinthepaperbyBrasilFilhoetal.14 These patientswere evaluatedprospectivelyinthe present studyafterameanfollow-upof5.4years.
Amongthe23patientswhowereincludedinthefirststudy, threewereexcludedfromthepresentstudybecausetheyhad diedinthemeantimeandtwobecausetheywerelostfromthe follow-up.Thus,18patientsremainedinthestudy(Table1). Amongthese,therewasonepatientwho evolvedwithlate postoperativeinfection andrequiredsurgerytoremovethe prosthesis.
Table1–Patientdata.
Patient Sex Timesinceop (years)
Age Side UCLAbeforeop UCLAone yearafterop
UCLAfinal evaluation
Elev/extrot/med rotbeforeop
Elev/extrot/med rotafterop
1 M 6.7 86 D 1+2+1+3+0=7 10+4+1+3+0=18 10+4+2+2+0=18 30/10/L2 40/10/L2 2 M 6.6 69 D 2+2+2+3+0=9 8+4+3+3+5=23 10+10+5+4+5=34 80/40/L3 120/50/L2 3 M 6.5 79 ND 2+4+3+3+0=12 8+6+3+3+5=25 8+8+4+3+5=28 54/0/T11 130/10/T8 4 F 6.0 89 D 2+4+3+2+0=11 8+6+3+3+5=22 8+6+3+3+5=25 40/10/L1 56/10/L1 5 F 5.8 67 ND 2+2+1+3+0=8 10+6+2+3+5=26 10+8+2+2+5=27 50/20/T12 70/40/T11 6 F 5.7 88 D 2+2+0+3+0=7 8+6+2+4+0=20 8+6+3+3+0=20 68/24/T12 80/30/T12 7 F 5.5 77 D 2+4+1+2+0=9 8+4+1+3+5=21 10+4+0+2+5=21 12/10/L5 20/20/L3 8 F 5.4 81 D 2+2+2+3+0=9 8+8+3+4+5=28 8+6+3+3+5=25 60/40/L1 110/44/L1 9 F 5.2 73 D 2+2+1+3+0=8 4+4+3+3+0=14 2+4+3+3+0=12 62/10/L1 90/20/L2 10 F 5.1 84 D 2+2+2+2+0=8 4+6+3+2+0=25 6+4+3+4+0=17 60/20/T11 70/20/T10 11 F 5.0 78 D 2+4+3+2+0=11 6+8+5+4+5=28 6+8+5+4+5=28 70/20/L2 120/36/L2 12 F 4.9 72 ND 2+2+0+2+0=6 8+4+2+3+5=22 8+8+3+4+5=28 56/40/L3 70/44/L2 13 F 4.7 70 ND 2+4+3+2+0=11 8+6+2+3+5=24 8+6+2+3+5=24 50/16/L1 60/30/T12 14 F 4.6 74 D 2+2+2+3+0=9 4+4+3+4+5=20 8+8+5+4+5=30 60/10/T10 110/20/T8 15 F 4.6 83 D 2+2+1+3+0=8 6+4+2+3+5=18 6+4+3+3+5=21 52/10/Trochanter 70/26/Sacrum 16 F 4.6 81 D 2+4+3+2+0=11 8+8+4+4+5=29 8+6+4+4+5=27 70/10/T10 120/22/T8 17 F 5.2 87 D 1+2+3+3+0=9 6+4+3+3+5=21 6+4+3+3+5=21 40/20/L3 60/30/L3 18 F 6.0 66 ND 2+2+2+3+0=9 8+4+3+4+5=24 8+6+2+4+5=25 90/30/L5 80/30/L5
M,male;F,female;D,dominantside;ND,non-dominantside;Elev,elevation;extrot,externalrotation;medrot,medialrotation;op,operation; UCLA,UniversityofCalifornia,LosAngeles.
PublicServants’Hospital).Adeltopectoralaccessroutewas used.
Thelengthofpostoperativefollow-uprangedfrom4.6to 6.7years,withameanof5.4.Themeanagewas78years.The dominantlimbwasaffectedin13patients(72.2%).
TheSeebauerclassificationwas used.12 In stageIA, the headiscenteredintheglenoid;inIB,theheadmigrates medi-allyandtheglenohumeralspacebecomespinched;inIIA,the humeralheadmigratessuperiorly,butisstabilizedbythe cora-coacromialarch,whichremainsintact;andinIIB,thehumeral headmigrates anterosuperiorly, dueto insufficiencyofthe coracoacromialarch.
Amongthe18patientsincludedinthisstudy,threewere classifiedbeforetheoperationasSeebauerlA,sevenaslBand eightasllA.
Theinclusioncriteriawerethatthepatientsneededtobe symptomaticandclassifiedasSeebauerlA,lBandllA,whodid notimprovewithconservativetreatmentoveraminimumof sixmonths.Theexclusioncriteriaweresituationsinwhich thepatientsimprovedthroughclinicaltreatmentorpresented previoussurgeryorneurologicallesionsinthelimbaffected, arthropathyclassifiedasSeebauerllBorinsufficiencyofthe deltoidmuscleandsubscapularismuscle.
Inevaluatingtheresults,thefunctionalscaleofthe Univer-sityofCaliforniainLosAngeles(UCLA)wasused,asmodified byEllmanandKay.29Toevaluatesatisfaction,theNeer crite-riawereused.Tomeasuretherangeofmotion,themethod oftheAmericanAcademyofOrthopedicSurgeonswasused. TocomparetheUCLAscoreandrange-of-motionresults,the nonparametricFriedmantestwasused.27–30
The statistical significance of the differences in means betweenthequantitativevariableswasascertainedbymeans of the paired Student’s t test and the differences in vari-ance were ascertained by means of analysis of variance (ANOVA).Thenormalityofthevariableswastestsusingthe Shapiro–Wilktest.Alloftheanalyseswereperformedusing
asignificancelevelof5%.Resultswithp-values<0.05were consideredtobestatisticallysignificant.Two-tailedoptional hypotheseswerealwaysenvisaged.
The information gathered formed a database that was developedusingtheExcel®softwareforWindowsandthe
sta-tisticalanalysiswas performedusingthe Stata® 11SE and
SPSS®16.0software.
Results
Afterameanfollow-upof5.4years,14patientsconsidered thattheywere satisfiedwiththesurgery(78%).Amongthe fourwhoweredissatisfied,threecomplainedabouttheirlack of gain inrange ofmotion, althoughtheyreported having achieved animprovementinpain inrelationtobefore the operation.Foronepatient,thedissatisfactionwasduemainly topain(Fig.3).
Satisfied 13
Dissatisfied 4
Movement 3
Pain 1
Fig.3–Patientdistributionaccordingtosatisfactionlevel
Table2–PvaluesforthevariablesoftheUCLAscore,comparedbetweenbeforetheoperation,afteroneyearoffollow-up andatfinalevaluation.
Variables Beforeoperation Oneyearafterwards Finalevaluation p
Mean(SP) Min–Max Mean(SP) Min–Max Mean(SP) Min–Max
Pain 1.89(0.32) 1–2 7.22(1.83) 4–10 7.67(1.97) 2–10 <0.001
Function 2.67(0.97) 2–4 5.33(1.53) 4–8 6.11(1.88) 4–10 <0.001 Activeflexion 1.83(1.04) 0–3 2.67(0.97) 1–5 3.06(1.26) 0–5 <0.001
Flexionforce 2.61(0.50) 2–3 3.28(0.57) 2–4 3.22(0.73) 2–4 0003
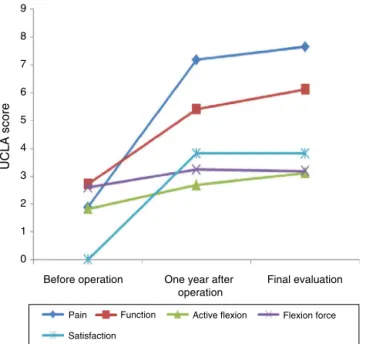
Satisfaction 0.00(0.00) 0–0 3.89(2.14) 0–5 3.89(2.14) 0–5 <0.001 UCLAscore 9.00(1.64) 6–12 22.39(4.23) 14–29 23.94(5.30) 12–34 <0.001
Inrelationtotherangeofmotionafterameanfollow-upof 5.4years,therewasanimprovementinthemeanactive ele-vation,whichwentfrom55.8◦beforetheoperationto82◦after
the operation. The mean external rotation improved from 18.9◦beforetheoperationto27.3◦aftertheoperation(Fig.4). Themeanmedialrotationremainedatthelevelofthethird lumbarvertebra.
ThemeanUCLAscoreafterthemeanfollow-upof5.4years was23.94andthiswasasignificantimprovementin compar-isonwiththepreoperativemeanofnine(p<0.001).Asmall improvementwasobservedinrelationtothemeanafterthe firstpostoperativeyear(22.39),butwithoutstatistical signifi-cance.Themeanpainlevelwas7.67,witharangefrom2to 10;functionwas6.11,rangingfrom4to10;activeflexionwas 3.06,rangingfrom0to5;anteriorflexionforcewas3.22, ran-gingfrom2to4;andsatisfactionwas3.89,rangingfromzero to5.Therewerestatisticallysignificantimprovementsinall thecriteriaforassessingtheUCLAscore(Table2andFig.5).
Thereweresignificantimprovementsbetweenthepreand postoperativeevaluations,bothatoneyearafterthe opera-tionandattheendofthefollow-up.However,therewasno statisticallysignificantchangebetweenthetwopostoperative evaluations,performedatmeansofoneand5.4yearsafterthe operation(Table3).
Discussion
CTA®partialarthroplastyfortreatingarthropathyofthe
rota-tor cuff is a relatively recent procedure, with few studies
Elevation
Angle
90
80
70
60
50
40
30
20
10
0
Before operation After operation External rotation
Fig.4–Comparisonofthemeananglesofelevationand
externalrotationfrombeforetoaftertheoperation.
availableinthe literature,especiallywithlong-term follow-ups.3,31,32
Vitotskyetal.13conductedastudywithameanfollow-up of32monthsandminimumoftwoyears,on60patientswho underwentCTA®partialarthroplasty,includingSeebauerIA,
IBandIIApatients.Theyobtainedsatisfactoryresultsin89%of thecases,withmeanimprovementsof22◦inexternalrotation and60◦inflexion.Inoursample,afteraminimumfollow-up of4.6yearsand meanof5.4years,among18 CTA® partial
arthroplastyproceduresin18patients,themeansatisfaction rateobtainedwas78%,withameanimprovementinelevation from55.8◦to82◦andinexternalrotationfrom18.9◦to27.3◦. Justasinourstudy,Vitotskyetal.13didnotincludeSeebauer IIBpatients.
Over a mean follow-up of 3.7 years, Goldberg et al.18 obtainedasatisfactionrateof78%,withmeanimprovements of33◦inelevationand23◦inexternalrotationthroughusing conventionalhemiarthroplasty.Thepatientswithaminimum elevationof90◦achievedthebestresults.Inourstudy,patients withelevationsoflessthan90◦wereexcluded.
Ina studywithamean follow-upof28.2 monthson 15 casesofhemiarthroplasty,Zuckermanetal.26obtainedmean improvementsof17◦inelevationand14◦inlateralrotation.
Before operation
UCLA score
Pain 9
8
7
6
5
4
3
2
1
0
Function Active flexion Flexion force
Satisfaction
One year after operation
Final evaluation
Fig.5–ComparisonoftheUCLAscoresbeforethe
Table3–PvaluesforthevariablesoftheUCLAscoreoverseparatetimes.
Pain Function Activeflexion Flexionforce Satisfaction UCLAscore
Beforeoperationvs.oneyearafteroperation p<0.001 p<0.001 p<0.002 p<0.002 p<0.001 p<0.001 Beforeoperationvs.finalevaluation p<0.001 p<0.001 p<0.003 p<0.005 p<0.001 p<0.001 Oneyearsafteroperationvs.finalevaluation p=0.157 p=0.448 p=0.207 p=1.00 p=1.00 p=0.303
Thesatisfactionrate amongthe patientswas 87%and the UCLAscoreimprovedfrom11to22points.
Checchiaetal.33followedup11patientswhounderwent hemiarthroplastytotreatarthropathyoftherotatorcuff,for amean of 69 months.They obtaineda pain improvement rateof81.8%,satisfactoryresultsin54%andamean UCLA scoreof22.7points.Theseauthorsobservedthatcertain fac-torswereassociatedwithunsatisfactoryevolution, suchas previoussurgeryontheshoulderwithimpairmentofthe cora-coacromialarchandpreviousinjuryofthedeltoidmuscle.In oursample,patientswithpreviousshouldersurgeryandthose classifiedasSeebauerIIBwereexcluded.
In our study, patients whose main preoperative symp-tomwas limitationofmovements presentedunsatisfactory resultsafterthesurgery,suchthatthreeofthefourdissatisfied patientsreportedthiscomplaint.Thisfindingisinconformity withthestudybyNametal.34
The UCLA functional score, which assesses pain, func-tion, active flexion,anterior flexion force and satisfaction, improvedfrompoor(meanofninepoints)beforethe oper-ation,toreasonableafterfollow-upsofoneyearand5.4years (meansof22.39and 23.94points,respectively), which con-firmedthathemiarthroplastywasagoodoptionforsurgically treatingarthropathyoftherotatorcuffinselectedpatients. TherewasastatisticallysignificantimprovementinUCLA,in relationtobeforetheoperation,whilethedifferencebetween themeanpostoperativetimesofoneyearand5.4yearswas smallandnon-significant.Thiscanbeunderstoodas main-tenanceofthepositiveresultsfromtheprosthesisoverthis postoperativeperiod.
Since this is a surgical procedure indicated for elderly patients, oneofthe factors that causeddifficulty in carry-ingoutthepresentstudywasinrelationtomakinglong-term reevaluationsonallthepatients,becauseofdeathsandloss offollow-up.
Conclusion
Thefunctional resultsfrom non-conventional CTA® partial
arthroplasty for treating arthropathy ofthe rotator cuff in selectedpatientsremainedsatisfactoryafteramean follow-upof5.4years.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. HalversonPB,CheungHS,McCartyDJ,GarancisJ,MandelN. Milwaukeeshoulder:associationofmicrospheroids
containinghydroxyapatitecrystals,activecollagenase,and neutralproteasewithrotatorcuffdefectsII.Synovialfluid studies.ArthritisRheum.1981;24(3):474–83.
2.NeerCS2nd,CraigEV,FukudaH.Cuff-teararthropathy.J BoneJointSurgAm.1983;65(9):1232–44.
3.RockwoodCA,MatsenFA,editors.Theshoulder.6thed. Philadelphia:Saunders/Elsevier;2009.
4.CofieldRH,ParviziJ,HoffmeyerPJ,LanzerWL,IlstrupDM, RowlandCM.Surgicalrepairofchronicrotatorcufftears.A prospectivelong-termstudy.JBoneJointSurgAm. 2001;83(1):71–7.
5.CollinsDN,HarrymanDT2nd.Arthroplastyforarthritisand rotatorcuffdeficiency.OrthopClinNAm.1997;28(2): 225–39.
6.BokorDJ,HawkinsRJ,HuckellGH,AngeloRL,Schickendantz MS.Resultsofnonoperativemanagementoffull-thickness tearsoftherotatorcuff.ClinOrthopRelatRes.
1993;(294):103–10.
7.ZumsteinMA,JostB,HempelJ,HodlerJ,GerberC.Theclinical andstructurallong-termresultsofopenrepairofmassive tearsoftherotatorcuff.JBoneJointSurgAm.
2008;90(11):2423–31.
8.EcklundKJ,LeeTQ,TiboneJ,GuptaR.Rotatorcufftear arthropathy.JAmAcadOrthopSurg.2007;15(6):340–9. 9.ZemanCA,ArcandMA,CantrellJS,SkedrosJG,BurkheadWZ
Jr.Therotatorcuff-deficientarthriticshoulder:diagnosisand surgicalmanagement.JAmAcadOrthopSurg.
1998;6(6):337–48.
10.JensenKL,WilliamsGRJr,RussellIJ,RockwoodCAJr.Rotator cuffteararthroplasthy.JBoneJointSurgAm.
1999;81(9):1312–24.
11.HamadaK,FukudaH,MikasaM,KobayashiY.
Roentgenographicfindingsinmassiverotatorcufftears:a long-termobservation.ClinOrthopRelatRes.1990;(254): 92–6.
12.SeebauerL.Biomecanicalclassificationofcuffteararthropaty [abstract].In:Globalshouldersocietymeeting.2003.p.17–9. 13.VisotskyJL,BasamaniaC,SeebauerL,RockwoodCAJr,Jensen
KL.Cuffteararthroplasthy:pathogenesis,classification,and algorithmfortreatment.JBoneJointSurgAm.2004; 86(Suppl2):35–40.
14.BrasilFilhoR,RibeiroFR,TenorJuniorAC,FilardiFilhoCS, CostaGBL,StortiTM,etal.Resultadosdotratamentocirúrgico daartroplastiadegenerativadomanguitorotadorutilizando hemiartroplastiaCTA®.RevBrasOrtop.2012;47(1):66–72. 15.ZvijacJE,LevyHJ,LemakLJ.Arthroscopicsubacromial
decompressioninthetreatmentoffullthicknessrotatorcuff tears:a3-to6-yearfollow-up.Arthroscopy.1994;10(5):518–23. 16.ArntzCT,MatsenFA3rd,JackinsS.Surgicalmanagementof
complexirreparablerotatorcuffdeficiency.JArthroplasty. 1991;6(4):363–70.
17.FranklinJL,BarrettWP,JackinsSE,MatsenFA3rd.Glenoid looseningintotalshoulderarthroplasty:associationwith rotatorcuffdeficiency.JArthroplasty.1988;3(1):39–46. 18.GoldbergSS,BellJE,KimHJ,BakSF,LevineWN,BiglianiLU.
Hemiarthroplastyfortherotatorcuff-deficientshoulder.J BoneJointSurgAm.2008;90(3):554–9.
19.GrammontP,TrouilloudP,LaffayJP,DeriesX.Conceptstudy andrealizationofanewtotalshoulderprosthesis.
20.SirveauxF,FavardL,OudetD,HuquetD,WalchG,MoléD. Grammontinvertedtotalshoulderarthroplastyinthe treatmentofglenohumeralosteoarthritiswithmassive ruptureofthecuffResultsofamulticentrestudyof80 shoulders.JBoneJointSurgBr.2004;86(3):388–95.
21.YoungSW,EvertsNM,BallCM,AstleyTM,PoonPC.TheSMR reverseshoulderprosthesisinthetreatmentofcuff-deficient shoulderconditions.JShoulderElbowSurg.2009;18(4):622–6. 22.BoileauP,WatkinsonDJ,HatzidakisAM,BalgF.Grammont
reverseprosthesis:design,rationale,andbiomechanics.J ShoulderElbowSurg.2005;14(Suppl1):147S–61S.
23.WernerCM,SteinmannPA,GilbartM,GerberC.Treatmentof painfulpseudoparesisduetoirreparablerotatorcuff dysfunctionwiththeDeltaIIIreverse-ball-and-sockettotal shoulderprosthesis.JBoneJointSurgAm.2005;87(7):1476–86. 24.FrankleM,SiegalS,PupelloD,SaleemA,MighellM,VaseyM.
TheReverseShoulderProsthesisforglenarthritisassociated withsevererotatorcuffdeficiency:aminimumtwo-year follow-upstudyofsixtypatients.JBoneJointSurgAm. 2005;87(8):1697–705.
25.Sanchez-SoteloJ,CofieldRH,RowlandCM.Shoulder hemiarthroplastyforglenohumeralarthritisassociatedwith severerotatorcuffdeficiency.JBoneJointSurgAm.
2001;83(12):1814–22.
26.ZuckermanJD,ScottAJ,GallagherMA.Hemiarthroplastyfor cuffteararthropathy.JShoulderElbowSurg.2000;9(3):169–72.
27.HawkinsRJ,BokorDJ.Clinicalevaluationofshoulder problems.In:RockwoodCA,MatsenFA,editors.Theshoulder. 2nded.SaintLouis:Saunders;1998.p.164–98.
28.VieiraS.Bioestatística:tópicosavanc¸ados.3rded.Riode Janeiro:Elsevier;2010.
29.EllmanH,KaySP.Arthroscopicsubacromialdecompression forchronicimpingement.Two-tofive-yearresults.JBone JointSurgBr.1991;73(3):395–8.
30.NeerCS2nd,WatsonKC,StantonFJ.Recentexperiencein totalshoulderreplacement.JBoneJointSurgAm. 1982;64(3):319–37.
31.TrailI.Earlyresultswithaspecifichemiarthroplastyforcuff teararthropathy.PersCommun.2007.
32.BasamaniaC.Hemiarthroplastyforcuffteararthroplasthy. In:ZuckermannJD,editor.Advancedreconstruction: shoulder.Rosemont:AmericanAcademyofOrthopaedic Surgeons;2007.p.567–78.
33.ChecchiaSL,SantosPD,MiyazakiNA,FregonezeM,SilvaLA, LeiteFSF,etal.Avaliac¸ãodosresultadosdaartroplastia parcialdeombroparatratamentodaartroplastiaporlesãodo manguitorotador.RevBrasOrtop.2008;43(6):
232–9.