SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Rotator
cuff
injuries
and
factors
associated
with
reoperation
夽
Alexandre
Litchina
Carvalho
a,∗,
Fabrício
Martinelli
b,
Lucas
Tramujas
b,
Marcelo
Baggio
b,
Marina
Spricigo
Crocetta
b,
Rafael
Olivio
Martins
caServiceofOrthopedyandTraumatology,HospitalRegionalSãoJoséHomerodeMirandaGomes,SãoJosé,SC,Brazil
bUniversidadedoSuldeSantaCatarina,Tubarão,SC,Brazil
cOrtoimagemCentrodeOrtopediaeImagem,Tubarão,SC,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received9June2015 Accepted13July2015 Availableonline9April2016
Keywords: Rotatorcufftear Shoulder Reoperation
a
b
s
t
r
a
c
t
Objective:Toevaluatetheprevalenceofrotatorcufftearsanddescribetheprofileof reoper-atedpatients,causesofrepeatedtendontears,tearevolutionandrangeoftimesbetween surgicalprocedures.
Method:Thiswasacross-sectionalstudyinvolving604surgicalproceduresperformedat tworegionalreferralhospitalsbetweenJanuary2006andDecember2012.Afterapprovalby theethicscommittee,datadescribingthepatients’epidemiologicalprofileweregatheredat asingletime,usingCofield’sclassificationtomeasuretheextentofthetears,allofwhich underwentarthroscopicsurgery.ThedatawereenteredintoEpiInfo3.5.3andwereanalyzed usingSPSSversion18.0.
Results:Amongthe604 surgicalprocedures, females wereaffected inmore cases(351; 58.1%).Whenthedominantlimbwastherightlimb,itwasaffectedin90%ofthecases (p<0.05).Thesupraspinatustendonwasaffectedin574cases(95%)andthetearswere ofmediumsizein300cases(49.7%).Eighteenreoperationswereperformed(2.98%)and theupperrightlimbwasthemostaffected(66.6%).Thecausewasnon-traumaticin12 patients.Therepeatedtearsweremostlysmaller(44%),andthelengthoftimebetweenthe twosurgicalproceduresrangedfrom6to298weeks.
Conclusion:Femalegender,smallerextentinthesecondprocedureandnon-traumaticcause werefoundinmostofthecasesanalyzed.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheHospitaleMaternidadeSocimedandHospitalNossaSenhoradaConceic¸ão,Tubarão,SC,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.L.Carvalho).
http://dx.doi.org/10.1016/j.rboe.2015.07.008
Lesões
do
manguito
rotador
e
fatores
associados
à
reoperac¸ão
Palavras-chave:
Lesãodomanguitorotador Ombro
Reoperac¸ão
r
e
s
u
m
o
Objetivo: AvaliaraprevalênciadeLMR,descreveroperfildopacientereoperado,acausa darerrupturatendínea,aevoluc¸ãodalesãoeavariac¸ãodetempoentreosprocedimentos cirúrgicos.
Métodos: Estudocomdelineamentotransversal,queenvolveu604eventoscirúrgicosfeitos entre janeiro de 2006 e dezembrode 2012, em dois hospitais de referência regional. Apósaprovac¸ãopelocomitêdeética,osdadosforamcoletadosemumúnicomomento, descreveu-seoperfilepidemiológicodospacienteseusou-seaclassificac¸ãodeCofieldpara mensuraraextensãodaslesões,asquaisforamoperadasporviaartroscópicaemtodosos pacientes.OsdadosforamdigitadosnoprogramaEpinfoversão3.5.3®,eanalisadosnoSPSS
versão18.0®.
Resultados: Entre os 604 procedimentos, o sexo feminino esteve predominantemente acometidocom351(58,1%)equandoomembrodominantefoiodireitoeleesteveacometido em90%doscasos(p<0,05).Otendãosupraespinhalfoiacometidoem574(95%)casose aslesõesforamdetamanhomédioem300(49,7%)casos.Foram18(2,98%)reoperac¸õese omembrosuperiordireitofoiomaisacometido(66,6%),comcausanãotraumáticaem12 pacientes.Asrelesõesforamemsuamaioriamenores(44%),comotempoentreosdois procedimentoscirúrgicosquevariouentreseise298semanas.
Conclusão: Sexo feminino, extensão menor no segundo procedimento e causa não traumáticaforamencontradosnamaiorpartedoscasosanalisados.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Rotatorcuffinjuries(RCI)arecommoninorthopedicpractice, and account for nearly 70% of the events of shoulder pain.1 Its complete tear is associated to traumatic situ-ations in young individuals, whereas it has the tendon fragilityasanetiologyinoldpatients,withrepetitivemicro traumasassociatedwithacromialanatomyandpoortendon vascularization.2–4
Dependingonthetypeofinjury,asinpatientswithsignsof subacromialimpingement,theclinicaltreatmentwith physi-caltherapyandlifestylechangescanpostponethefunctional impairmentoftherotatorcuff.However,inindividualswho suffered complete rupture of a cuff tendon, clinical treat-mentdoesnotachieve goodresultsandthe surgicalrepair isindicated.5
TheworstcomplicationthatapatientoperatedforRCIcan developisthere-ruptureofthetendon,whichneedsnew sur-gicalintervention.
There are few studies that address reoperations of the rotator cuff. Nevertheless, data available in the literature demonstrate that the obtained results are inferior to the resultsofthe primaryprocedure, withimprovementofthe pain,butnosignificantrecoveryofcufffunction.
Thisstudyaimedtoevidencetheprevalenceofrotatorcuff reoperationsinaestablishedperiodandtheassociatedfactors thatledtothefailureoftheprimarysurgery.
Materials
and
methods
This was an observational, retrospective, cross-sectional study,usingdescriptive andanalyticalstatistics,conducted withpatientswhounderwentsurgeryduetoRCIbetween Jan-uary1,2006andDecember31,2012.Inthereportedperiod, 604surgeriesforthecorrectionofsymptomaticRCIwere con-ducted,allarthroscopically,bythesame specialistsurgeon, accompaniedbythesameorthopedicteam.Ofthese,36 sur-gerieswereconductedinaphilanthropichospitaland568ina privatehospital.Theinclusioncriteriawerepatients undergo-ingshouldersurgeryduetoRCIintheaforementionedperiod andinstitutions.Exclusioncriteriawerepatientswith incom-pletemedicalrecordsandthosewhowerere-operatedbythe team,butunderwenttheirfirstsurgeryinanotherhospital.
non-traumatic.Regardingtheaffectedtendon,injuriesinthe supraspinatus,infraspinatus,teresminor,andsubscapularis were observed.Regarding thesizeofthe injuryinthe sec-ondprocedure, theywereclassifiedaslarger,smaller,orof thesamesizerelativetotheprimarysurgicalprocedure.
Regardingtheassociatedprocedures,acromioplasty, bur-sectomy,andlongheadofbicepstenotomyortenodesis,were eventuallyused.
Thesociodemographic variables recorded were age and gender.Asforcomorbidities,thepresenceofhypertension, diabetes mellitus, smoking,and other co-morbidities were considered.
Inthe statistical analysis, datawere entered inEpinfo®
version3.5.3andanalyzedinSPSSversion18.0.
Thequantitative variables were described as mean and standarddeviation,andthequalitativevariablesasabsolute andrelativefrequency.Tocomparethemeans,Student’st-test wasused.Fisher’schi-squaredorFisher’sexacttestwereused whenappropriate,totestthestatisticalsignificanceofthe dif-ferencesobservedintheproportionsofcategoricalvariables. Two-tailedp-values<0.05% were considered as statistically significant.
ThisstudywassubmittedtoandapprovedbytheResearch EthicsCommitteeundertheProtocolNo.12.416.4.01.III.
Results
Amongthe604surgeriesforRCIcorrections,therewasa pre-dominanceofproceduresinfemalepatients(351;58.1%).The mean age was 55.2 years (SD±10.89years) and 18 (2.98%) patientsunderwentreoperation(Table1).
Thedominantandpredominantlyaffected limbwasthe rightone(Table2).
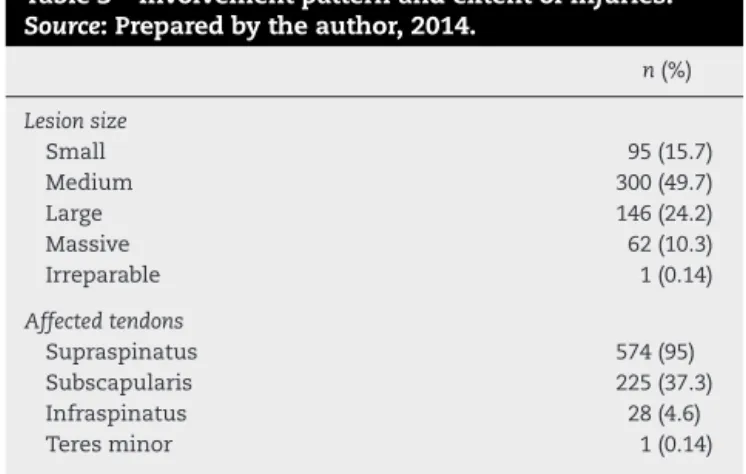
Regardingthepatternofonsetandextentoflesions,most patientspresentedmediumlesionsize.Themostaffected ten-donwasthesupraspinatus(Table3).
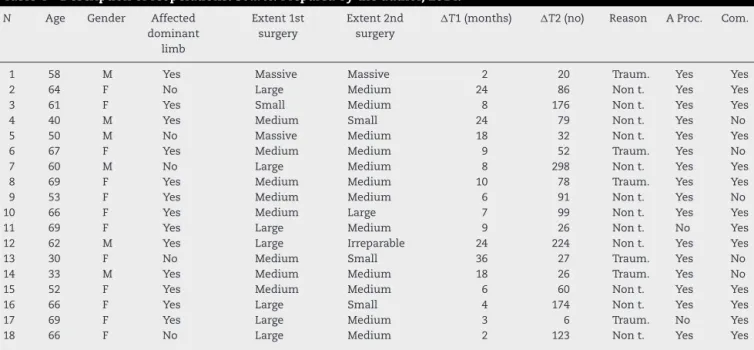
Assessingonlypatientswhounderwentreoperation,itwas observedthatthemeanagewas57.5years(±12.3);13(72.3%) patientshadsomecomorbidity.Theperiodbetweentheonset
Table1–Patientswithrotatorcuffinjuries
characteristics.Source:Preparedbytheauthor,2014.
Variables N(604)
Gender(%)
Male 253(41.9)
Female 351(58.1)
Age(years) 55.2±10.5
Reoperation(%) 18(2.98)
Table2–Relationshipbetweentheaffectedlimband dominantlimb.Source:Preparedbytheauthor,2014.
Dominantlimb Right Left p-Valuea
n(%) n(%)
Right(n=387) 350(90.4) 37(9.6) <0.01 Left(n=217) 67(30.9) 150(69.1) >0.05
a Pearson’schi-squaredtest.
Table3–Involvementpatternandextentofinjuries.
Source:Preparedbytheauthor,2014.
n(%)
Lesionsize
Small 95(15.7)
Medium 300(49.7)
Large 146(24.2)
Massive 62(10.3)
Irreparable 1(0.14)
Affectedtendons
Supraspinatus 574(95)
Subscapularis 225(37.3)
Infraspinatus 28(4.6)
Teresminor 1(0.14)
ofsymptomsanddateofthefirstreconstructivesurgerywas onaverage12.1months,withaminimumoftwoand maxi-mumof36.Inturn,thetimeintervalbetweenthefirstand secondsurgerywasfromsixto298weeks,withamedianof 78.5weeks(approximately20months;Table4).
Regarding the reason for reoperation, non-traumatic causes were the most frequent: 12 (66.6%). Regarding the extentoftheinjury,mediumlesionswerethemostprevalent (Table4).
Discussion
RCIreoperationrateisvaried;dependingonthepopulation studiedandtheapproachusedinthefirstprocedure,itmay rangefrom3%to12%.6–8Insevenyears,theorthopedicteam responsible for the present study obtained a rateof 2.98% patientswithsymptomaticrecurrencesofRCI.9
Isolateimagingexamsarenotsufficienttoindicatea sec-ondsurgery.AccordingtoIannottietal.,10magneticresonance imaging(MRI)oftheoperatedshoulderperformedfourweeks aftersurgeryforrotatorcuffrepairdisclosesfibrousscarring thatwasdifficulttodifferentiatefromaninjury.Considering this information, a detailed history and physical examina-tionareessential,asasymptomaticpatientsdonothavean indicationforsurgery,despitepresenting changesin imag-ing tests.10–12 In line with such reasoning, all 18 cases of reoperation in the present study had some degree ofpain and limitation of movement and, in accordance with the abovementionedparameters,anadequateimagingexamwas requested onlyafterdetailedorthopedicassessmentofthe affectedlimb.
Awidevarietyoffactorscancausefailureoftheprimary repairandre-injury.6–10ThemaincauseoffailureinRCI sur-gicaltreatmentarepreviouslargeandmassiveinjuries.6,7,10 However,it was notpossibletoverify suchrelationinthis study.
Table4–Descriptionofreoperations.Source:Preparedbytheauthor,2014.
N Age Gender Affected
dominant limb
Extent1st surgery
Extent2nd surgery
T1(months) T2(no) Reason AProc. Com.
1 58 M Yes Massive Massive 2 20 Traum. Yes Yes
2 64 F No Large Medium 24 86 Nont. Yes Yes
3 61 F Yes Small Medium 8 176 Nont. Yes Yes
4 40 M Yes Medium Small 24 79 Nont. Yes No
5 50 M No Massive Medium 18 32 Nont. Yes Yes
6 67 F Yes Medium Medium 9 52 Traum. Yes No
7 60 M No Large Medium 8 298 Nont. Yes Yes
8 69 F Yes Medium Medium 10 78 Traum. Yes Yes
9 53 F Yes Medium Medium 6 91 Nont. Yes No
10 66 F Yes Medium Large 7 99 Nont. Yes Yes
11 69 F Yes Large Medium 9 26 Nont. No Yes
12 62 M Yes Large Irreparable 24 224 Nont. Yes Yes
13 30 F No Medium Small 36 27 Traum. Yes No
14 33 M Yes Medium Medium 18 26 Traum. Yes No
15 52 F Yes Medium Medium 6 60 Nont. Yes Yes
16 66 F Yes Large Small 4 174 Nont. Yes Yes
17 69 F Yes Large Medium 3 6 Traum. No Yes
18 66 F No Large Medium 2 123 Nont. Yes Yes
M,male;F,female;T1,timebetweensymptomonsetandfirstsurgery;T2,timeintervalbetweenbothprocedures;Traum,traumatic;Nont., nontraumatic;AProc.,associateprocedure;Com.,comorbidities.
thepresentstudy,sincein18reoperations,acromioplastywas necessaryinthevastmajority(88.9%).
Traumaisanotherreportedcauseofre-injuryofthe rota-torcuff.7,15–17Inastudyassessing63patientsunder50years old,anagegroupinwhichtraumaismoreprevalentasan RCItrigger,Miyazaki et al.18 observedthat traumawasthe causeoftwooutofthefourre-ruptures,withanintervalfrom eightto24weeksafterthefirstsurgery.Inthepresentsample, traumawasinformedbythepatientsasthecausativefactor oftherecurrenceofsymptomsand consequentre-injuryof therotatorcuffinsixcases(33.3%):threeofthem(50%)byfall onthelimbandthree(50%)bymovingthelimbbeyond bear-able.Ofthesesixpatients,asinMiyazakietal.19study,two (33%)wereagedbelow50years,andtheintervalbetweenthe twosurgicalprocedureswas26and27weeks(cases14and13, respectively).Despitethefactthatthesampleinthepresent studywasapproximatelytentimesgreaterthanthatofthe aforementionedSãoPaulo(Brazil)study,similarresultswere obtainedintheagegroupreported.
Inappropriate postoperativecareand infection were not observedasacauseofre-injuryinthepresentstudy.George etal.7found1.9%ofinfectionleadingtore-injuryofthe rota-torcuffin360patients, who were treatedwithantibiotics, debridement, and resuture, and progressed to satisfactory results.
Theinfluenceofco-morbiditiesasindirectcausesof heal-ingimpairmenthasbeenstudied.Almeidaetal.20 analyzed the relationship between smoking and failed arthroscopic sutureinpatientsoperatedforRCIandreportedthat smok-ershaveworseoutcomeswhencomparedtonon-smokers, butonlyincaseoflargeandmassivelesions.Inthepresent study,amongthe18reoperations,onlythree(16.6%)wereon smokers.SimilarlytothedatapresentedbyAlmeidaetal.,20 twohadmassivelesionsandonehadalargelesion(cases1,5, and7,respectively).Case1reportedtraumaasacausalfactor oftherecurrenceofsymptoms.
Patientswithchronicinjuriespresentsubstitutionof mus-cletissuebyfattybands;suchanatomicalchangeiscrucial forprognosis.ThelongerapatienthasanRCI,thehigherthe fattydegeneration,adeterminingfactorontheprognosisand on thepossibility ofreoperation.7 Theintervalfrom RCIto fatty degenerationonset isunclear.However,chroniccases (>sixmonths)haveahighertrend.7Inthepresentstudy,most reoperatedpatientshadchronicinjuries,thereforepresented atleastonepoorprognosticfactortotheattemptedsurgical repair.
Consideringsizeoftheinjurytobereoperated,thepresent dataaresimilartothoseintheliteratureregardingthe ten-dency ofthe secondinjury tobe smallerthan the original injury.6–10
Regarding thesurgicalapproachforarecurrentRCI, the arthroscopictechniquehasdemonstratedgoodpostoperative resultssinceitsappearanceandimprovements.6 Asforthe procedureusedforthesecondoperation,Georgeetal.,7ina revisionstudy,reportedbetterresultswhenthearthroscopic approachwasusedforreintervention.Inthistopic,Miyazaki etal.19observedapproximately80%ofbadresultswhenused anopenapproachforthereoperation.DeOrioetal.,21alsohad highernumberofbadresultsusingtheopenapproach, giv-ingscientificsupporttothearthroscopicapproach,whichwas usedforsurgicalinterventioninthe18casesherereported.
Conclusion
Arateof2.98%ofreoperationsforRCIwasobservedinthe presentstudy.Mostreoperatedpatientswerefemale,witha dominantandpredominantlyaffectedrightlimb,andthevast majoritypresentedasystemiccomorbidity.
wassmallerwhencomparedtothefirstsurgery.Theinterval betweenthetwosurgicalprocedures wasextremelyvaried; nevertheless,itwassmallerwhenthe reasonforthe inter-ventionwastraumatic.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. VeadoMAC,CastilhoRS,MaiaPEC,RodriguesAU.Estudo prospectivoecomparativodosresultadosfuncionaisapós reparoabertoeartroscópicodaslesõesdomanguitorotador. RevBrasOrtop.2011;46(5):546–52.
2. RathbunJB,MacnabI.Themicrovascularpatternofthe rotatorcuff.JBoneJointSurgBr.1970;52(3):540–53.
3. MatsenFA3rd,ArntzCT.Rotatorcufftendonfailure.In: RockwoodCA,MatsenFA3rd,editors.Theshoulder. Philadelphia:Saunders;1990.p.647–77.
4. MarcondesFB,RosaSG,VasconcelosRA,BastaA,FreitasDG, FukudaTY.Forc¸adomanguitorotadoremindivíduoscom síndromedoimpactocomparadoaoladoassintomático.Acta OrtopBras.2011;19(6):333–7.
5. ChecchiaSL,DoneuxSantosP,MiyazakiNA,FregonezeM, SilvaLA,MussiFilhoS,etal.Tratamentocirúrgicodaslesões extensasdomanguitorotadorpelaviadeacesso
deltopeitoral.RevBrasOrtop.2003;38(5):252–60.
6. MiyazakiAN,SantosPD,SilvaLA,SellaGV,SantosRMM, SouzaA,etal.Avaliac¸ãodosresultadosdasreoperac¸õesde pacientescomlesõesdomanguitorotador.RevBrasOrtop. 2011;46(1):45–50.
7. GeorgeMS,KhazzamM.Currentconceptsreview:revision rotatorcuffrepair.JShoulderElbowSurg.2012;21(4):431–40.
8. DjurasovicM,MarraG,ArroyoJS,PollockRG,FlatowEL, BiglianiLU.Revisionrotatorcuffrepair:factorsinfluencing results.JBoneJointSurgAm.2001;83-A(12):1849–55.
9. AinsworthR,LewisJS.Exercisetherapyfortheconservative managementoffullthicknesstearsoftherotatorcuff:a systematicreview.BrJSportsMed.2007;41(4):200–10.
10.IannottiJP,DeutschA,GreenA,RudicelS,ChristensenJ, MarraffinoS,etal.Timetofailureafterrotatorcuffrepair:a prospectiveimagingstudy.JBoneJointSurgAm.
2013;95(11):965–71.
11.GalatzLM,BallCM,TeefeySA,MiddletonWD,YamaguchiK. Theoutcomeandrepairintegrityofcompletely
arthroscopicallyrepairedlargeandmassiverotatorcufftears. JBoneJointSurgAm.2004;86(2):219–24.
12.BernhardJ,MatthiasZ,ChristianWA,PfirrmannCG. Long-termoutcomeafterstructuralfailureofrotatorcuff repairs.JBoneJointSurgAm.2006;88(3):472–9.
13.BiglianiLU,CordascoFA,McIlveenSJ,MussoES.Operative treatmentoffailedrepairsoftherotatorcuff.JBoneJoint SurgAm.1992;74(10):1505–15.
14.MacDonaldP,McRaeS,LeiterJ,MascarenhasR,LapnerP. Arthroscopicrotatorcuffrepairwithandwithout
acromioplastyinthetreatmentoffull-thicknessrotatorcuff tears:amulticenter,randomizedcontrolledtrial.JBoneJoint SurgAm.2011;93(21):1953–60.
15.GodinhoGG,FreitasJMA,Franc¸aFO,AndradeFilhoJS,Schio C,PintoJúniorSC.Estudodavascularizac¸ãodasbordasdas lesõesnasroturascompletasdomanguitorotador.RevBras Ortop.2007;42(6):169–72.
16.ChecchiaSL,DoneuxSantosP,MiyasakiAN,FregonezeM, SilvaLA,IshiM,etal.Avaliac¸ãodosresultadosobtidosna reparac¸ãoartroscópicadaslesõesdomanguitorotador.Rev BrasOrtop.2005;40(5):229–38.
17.BittarES.Arthroscopicmanagementofmassiverotatorcuff tears.Arthroscopy.2002;18(9Suppl2):104–6.
18.MiyazakiNA,FregonezeM,SantosPD,SilvaLA,SellaGV, SantosRMM,etal.Avaliac¸ãodosresultadosdoreparo artroscópicodelesõesdomanguitorotadorempacientes comaté50anosdeidade.RevBrasOrtop.2011;46(3):276–80.
19.MiyazakiAN,FregonezeM,SantosPD,SilvaLA,OrtizECM, ChecchiaSL.Lesõesextensasdomanguitorotador:avaliac¸ão dosresultadosdoreparoartroscópico.RevBrasOrtop. 2009;44(2):148–52.
20.AlmeidaA,ValinMR,ZampieriR,AlmeidaNC,RovedaG, AgostiniAP.Análisecomparativadoresultadodasutura artroscópicadalesãodomanguitorotadorempacientes fumantesenãofumantes.RevBrasOrtop.2011;46(2):172–5.