SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
report
Malignant
Triton
tumor:
a
rare
cause
of
sciatic
pain
and
foot
drop
夽
Maribel
R.
Gomes
a,∗,
Alexandre
M.P.
Sousa
b,
Roberto
J.A.
Couto
a,
Marco
M.B.
Oliveira
a,
João
L.M.
Moura
a,
Carlos
A.
Vilela
aaHospitaldaSenhoradaOliveira,Servic¸odeOrtopediaeTraumatologia,Guimarães,Portugal
bInstitutoPortuguêsdeOncologia,Servic¸odeCirurgiaGeral,Porto,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received13June2016 Accepted21July2016 Availableonline10June2017
Keywords: Tritontumor Nervesheathtumors Sciaticnerve
a
b
s
t
r
a
c
t
Malignantperipheralnervesheathtumors(MPNST)areveryrareandarefrequently local-izedinthebuttocks,thigh,arm,orparaspinalregion;onevariantisthemalignantTriton tumor,withrhabdomyosarcomatousdifferentiation.Theauthorspresentachallenging dif-ferentialdiagnosisofasciaticpainandfootdropinawomanwithhistoryoflumbardisk herniation,whichwasfoundtobecausedbyaTritontumorofthesciaticnerve.She under-wentsurgicalexcision,followedbyradiationandchemotherapy.MalignantTritontumor caseshaverarelybeendescribedandreportedintheliterature.Therecommendedtreatment isradicalexcisionfollowedbyhigh-doseradiotherapyandchemotherapy.Theprognosis, althoughpoor,dependsonthelocation,grade,andcompletenessofsurgicalmargins.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Tumor
de
Triton
maligno:
uma
causa
rara
de
dor
ciática
e
pé
pendente
Palavras-chave: TumordeTriton
Neoplasiasdabainhaneural Nervociático
r
e
s
u
m
o
Ostumoresmalignosdabainhadosnervosperiféricos(TMBNP)sãomuitorarose localizam-semaisfrequentementenaregiãonadegueira,paraespinal,coxaoubrac¸o;umavarianteé otumordeTritonmaligno,comumadiferenciac¸ãorabdomiosarcomatosa.Apresentamos umdiagnósticodiferencialdesafiantededorciáticaepépendenteemumapacientecom antecedentesdehérniadiscallombar,quesedescobriuqueeracausadaporumtumorde Tritondonervociático.Apacientefoisubmetidaaexcisãocirúrgica,seguidaderadioe
夽
StudyconductedattheHospitaldaSenhoradaOliveira,Servic¸odeOrtopediaeTraumatologia,Guimarães,Portugal. ∗ Correspondingauthor.
E-mail:[email protected](M.R.Gomes).
http://dx.doi.org/10.1016/j.rboe.2017.06.001
quimioterapia.PoucoscasosdetumoresdeTritonmalignosforamdescritoserelatadosna literatura.Otratamentorecomendadoéaexcisãoradical,seguidaderadioterapiaemalta doseequimioterapia.Oprognóstico,emboramau,dependedalocalizac¸ão,dograuedas margenscirúrgicasdaexérese.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Malignanttumorsthatoriginateordifferentiatefromthe var-iousnervesheathlineagesarecollectivelytermedmalignant peripheralnerve sheath tumors(MPNST); they represent a smallpercentageofsofttissuesarcomas,andmaybesporadic orassociatedwithneurofibromatosistype1.1,2
Theyareoftenlocatedinthebuttocks,thighs,arms,orthe paraspinalregion.Mostarehigh-gradesarcomas,whichoften metastasizetothelungsorbone;avariantofthisraretypeis themalignanttritontumor,whichhas rhabdomyosarcoma-tousdifferentiation.1,3
Case
report
Thisstudyreportsthecaseofa45-year-oldfemalepatientwho hadahistoryoflowbackpainandsciaticpainwithprogressive aggravationinthelastsixmonths.AxialCTscanindicatedleft L5-S1diskherniation(Fig.1).Herphysicianreferredhertoan OrthopedicSurgeryspecialistandwaswhileawaitingforthe visitshegotintramuscularnon-steroidalanti-inflammatory drugs(NSAIDs)prescriptions.
However,intheprevioustwoweeks,thepatientdeveloped apainfulswellingintheleftbuttockthatshebelievedtobe relatedto the NSAIDsinjections, attendingthe Orthopedic EmergencyRoom.
Physicalexaminationindicatedahardswellingintheleft buttock,hypoesthesiaoftheleftlegwithnospecificterritory, apositiveLasèguesign,footdropgait,andabsenceofAchilles reflex.
Anultrasoundexaminationofthebuttockwasperformed, whichindicatedavascularizedmassintheleftglutealregion. Magnetic resonance imaging (MRI) confirmed a heteroge-neouslesionof10.5×4.5cm,deepintheglutealmuscles,that
entered the pelviccavity throughthe greater sciatic notch (Figs.2and3).
Thepatient underwent tru-cut biopsy,which revealed a malignanttritontumor;onemonthlater,sheunderwenten blocresectionofthetumorandsciaticnerveroots.Twomonths aftersurgery,adjuvantradiotherapy(RT)andchemotherapy (doxorubicin)wereinitiated.
Histopathologyindicatedthatthesurgicalresectionwas complete; together with the imagingdata, the lesion was stagedasagrade-IIIpT2bN0M0tumor.
Four months after surgery, hypoesthesia and drop foot persisted; electromyography confirmed neurotmesis of the sciatic nerve. She was referred for physical medicine and
Fig.1–SagittalsectionofaT2-weightedlumbarspineMRI disclosingofL5-S1diskherniation.
rehabilitation,followedthephysiotherapyplan,andwalked withananti-equinusorthosis.
Ateightmonthspostoperatively,shepresented dysesthe-siaandcomplainedofpainatthelevelofthepelvis,irradiating tothe left lower limband refractorytoanalgesia.Shealso presentedfever,dyspnea,constipation,andurinaryretention. Thepatientwasadmitted;anewlumbarspineandhipMRI wererequested,aswellasathoracicCT.
Fig.2–CoronalsectionofaT2-weightedpelvicMRIdisclosingthelesionintheleftglutealregion.
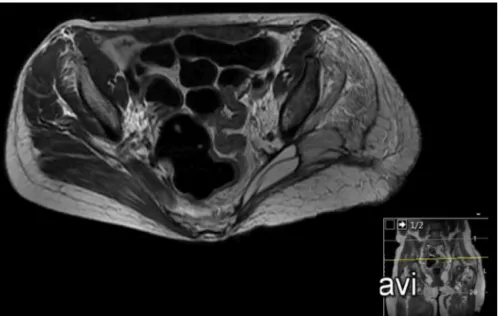
Fig.3–AxialsectionofaT2-weightedpelvicMRIidentifyingthelesionintheleftglutealregion.
Atninemonthspost-operatively,shediedofprogressive respiratoryfailureandamine-refractoryshock.
Discussion
Traditionally,thediagnosisofMPNSThasbeendifficultamong softtissuetumorsduetothelackofstandardizeddiagnostic andhistologicalcriteria.Todate,therearenospecific biomark-ersthatcanhelpestablishthediagnosis.Thedivergenceinthe
diagnosticcriteriahasalsocontributedtothevariabilityofthe incidenceofsuchlesiondescribedintheliterature.3
MPNSToccurmostlybetweentheagesof20and50, affect-ingbothgendersequally.Inpatientswithneurofibromatosis type1,thesetumorstendtooccurinmales,atanearlierage, andtohavelargerdimensions.1–3
Fig.4–AxialsectionofaT2-weightedpelvicMRIinthepostoperativeperiod.
Fig.5–AxialcutofthoracicCTinthepostoperativeperiod.
swelling. The association of MPNST with the main nerve trunksexplainsitsgreaterincidenceintheproximalregions ofthelimbsandthetrunk(sciaticnerve,brachialplexus,and sacralplexus).3
Histologically,thesetumorsarecomposedof hyperchro-matic fusiform cells arranged in a fasciculated pattern. High-grade tumors usually contain areas of necrosis and increasedmitoticactivity.2,3
Thecapacity ofMPNSTtoundergo mesenchymal differ-entiation is well known. The malignant triton tumor is a rarevariantwithrhabdomyosarcomatousdifferentiation,first describedin1938byMassonandMartin.Itconsistsofastroma
typical ofMPNST, with additionalrhabdomyoblasts, which usuallyarisesphericallyandwitheosinophiliccytoplasm.2,3
Fewcasesofmalignanttritontumorshavebeendescribed intheliterature.Asthesearelesionswithahighprobability oflocalanddistantrecurrence,therecommendedtreatment isradical excisionfollowed byhigh-dose radiation therapy, although more recent studies suggest that chemotherapy mayeradicatemicrometastasesandextendsurvival.1,3
Dur-ingfollow-up,CTandpositronemissiontomographyarethe examsofchoiceintheevaluationofrelapses.2,3The
Thepresentcasehassomeparticularitiesthatmayhave causedadelayindiagnosisandmadeitevenmore challeng-ing.ThehistoryoflowbackpainwithadocumentedleftL5-S1 diskherniationcouldperfectlyexplainthesymptoms,leading theattendingphysiciantoreferthepatienttoanorthopedic surgeon.
Thedistinctivefeatureofthisclinicalcasewastheswelling intheleftbuttock,whichmayhaveraisedtheclinical suspi-cionofanothercauseforclinicalpresentation.
Enblocresectionofthetumoraswellasthesciaticnerve and its rootscontributed to postoperative motor and sen-sorydeficits,butwasanecessaryprocedure,sincethetumor invadedthenerve.Completesurgicalresectionandabsenceof nodularordistantmetastaseswouldrepresentgood prognos-ticfactors.However,thistypeoftumorhasagenerallypoor prognosis,whichwasconfirmedinthiscase.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.Fanburg-SmithJC.Nervesheathandneuroectodermaltumors. In:FolpeAL,InwardsCY,editors.Boneandsofttissue pathology.Philadelphia:Saunders;2010,193-23.8.
2.GoldblumJR,WeissSW,FolpeAL.Malignantperipheralnerve sheathtumors.In:EnzingerandWeiss’ssofttissuetumors.6th ed.Philadelphia:Elsevier;2014.p.855–79.