rev bras ortop.2017;52(1):115–118
SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Technical
Note
Modified
axillary
radiograph
of
the
shoulder:
a
new
position
夽
Luís
Filipe
Senna
a,∗,
Rodrigo
Pires
e
Albuquerque
baHospitalEstadualAdãoPereiraNunes,Servic¸odeOrtopediaeTraumatologia,DuquedeCaxias,RJ,Brazil
bUniversidadeFederalFluminense,Servic¸odeOrtopediaeTraumatologia,Niterói,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received18December2015 Accepted28January2016 Availableonline9December2016
Keywords: Shoulder
Shoulderdislocation Shoulderjoint Radiography
a
b
s
t
r
a
c
t
Obtainingaxillaryradiographsoftheshoulderinacutetraumaisnotalwaysfeasible.The authorspresentanewmodificationofthisradiographicview,inordertoassesstheanatomic relationshipbetweenthehumeralheadandtheglenoidcavity.Theincidenceisperformed withthepatientsittingonX-raytable,withtheaffectedlimbsupportedthereon.Theauthors describethecaseofa28-year-oldmalewhosufferedananteriorglenohumeral disloca-tionthatwasclearlyevidencedbythismodifiedradiograph.Theconcentricrelationship betweenthehumeralheadandtheglenoidcavitywasalsoeasilyconfirmedbyobtaining suchradiographafterthereductionmaneuver.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Modificac¸ão
da
incidência
radiográfica
axilar
para
o
ombro:
uma
nova
posic¸ão
Palavras-chave: Ombro
Luxac¸ãodoombro Articulac¸ãodoombro Radiografia
r
e
s
u
m
o
Aobtenc¸ãoderadiografiasemperfilaxilardoombroemsituac¸ãodetraumaagudonem sempreétarefafácil.Osautoresapresentamumamodificac¸ãoinéditadessaincidência radiográfica,comoobjetivodeavaliararelac¸ãoanatômicadacabec¸aumeralcoma cavi-dadeglenoide.Aincidênciaémedidacomopacientesentadosobreamesadeexamesde raiosX,comomembroacometidoapoiadosobreela.Osautoresdescrevemocasodeum pacientede28anosquesofreuumepisódiodeluxac¸ãoglenoumeralanteriorquefoi clara-menteevidenciadapelaradiografiamodificada.Arelac¸ãodeconcentricidadeentreacabec¸a umeraleacavidadeglenoidefoifacilmenteconfirmadapelaobtenc¸ãodareferidaincidência radiográficaobtidaapósamanobradereduc¸ão.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatHospitalMunicipalDr.NelsondeSáEarp,Petrópolis,RiodeJaneiro,RJ,Brazil,andatHospitalEstadualAdãoPereira Nunes,DuquedeCaxias,RJ,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](L.F.Senna). http://dx.doi.org/10.1016/j.rboe.2016.12.001
116
rev bras ortop.2017;52(1):115–118Introduction
Thereisageneralrecommendationforthecareoforthopedic traumapatients,whichistoobtainatleasttworadiographic viewsinorthogonalplanesforproperevaluationofthe trau-matized limb or joint.1 In the case of the shoulder joint, suchrecommendationisparticularly valuable,asfailure to obtainX-raysinorthogonalplanes,especiallyfailuretoobtain axillaryradiographs,isconsidered tobethemaincause of misdiagnosisinglenohumeraldislocations.2Radiographsin anteroposterior,lateralscapula,andaxillaryviewsareknown astheshouldertraumaseries3andmustbeperformedonall patientswithtraumaofsuchjoint.Theaxillaryviewwasfirst describedin1915byLawrenceapudJensenandRockwood,4 and can bedone withthe patient standing or sitting. Ide-ally,itisnecessarytopositiontheshoulderinapproximately 70◦–90◦ofabductiontoobtainthisradiograph.Inpatientswith mildtrauma, this degreeofabductionisfeasible; however, forpatients withmoreseveretrauma, andespeciallythose withglenohumeraljointdislocation,itisextremelydifficult toobtaintheaxialimage,becausepainandjointincongruity greatlylimittheabductioncapacityofthejoint.Thus, modi-ficationsintheclassicalaxillaryviewhavebeenproposed.5,6 TheviewdescribedbyBloomandObata5isperhapsthebest knownmethod,asitallowsforanaxillaryradiography with-outremovingthepatient’sarmfromthesling–whichwould inprinciplebemorecomfortable.Nonetheless, theauthors havefoundthis viewtobedifficulttoobtain, especiallyin the elderly, since it requires leaning the trunk posteriorly withthepatientstanding;maintainingbalanceisdifficultand limbpositioningishindered.TheviewdescribedbyCleaves6 requirestheuseofacurvedchassis,whichisnotwidely avail-able.Facedwiththesedifficulties,theauthorsidentifiedthe needtodevelopamodificationoftheLawrencetechniquein apositionthatwasmorecomfortableforthepatientand eas-iertoreproduce.Thepatient’spositioningfortheradiograph was namedthe Sennaposition, inreference tothe author andcreatorofthetechnique.Theincidencedescribedbelow aimstoshow,inaxialprojection,therelationshipbetweenthe humeralheadandglenoidcavity.
Technique
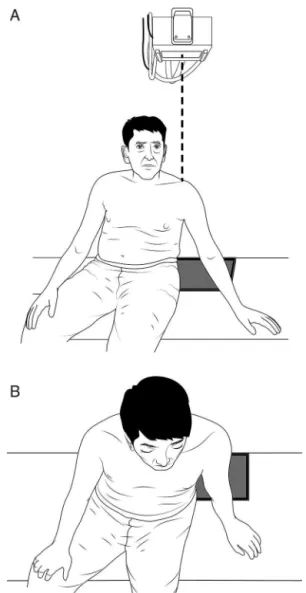
Toobtainthepresentmodificationoftheaxillaryradiograph, the patientis requiredtosit withthe feet hanging onthe radiographic table. Then, the patient is requested to posi-tiontheopenhandoftheaffectedsideonthetable.Onlya smalldegreeofabductionisrequired.Theabductionangle formedbetweenthemedialaspectofthearmandthelateral chestshould beapproximately 30◦. TheX-raysare pointed totheglenohumeraljoint,perpendiculartothetable,60cm fromtheshoulder.Thechassiswithradiographicfilmis pos-itioned on thetable, directly underthe shadowformed by the shoulder contour, with its anterior border just behind thegreater trochanter ofthefemur(Fig. 1). Itisimportant tonotethatthepatient’sbodyshouldslightlylean approxi-mately10◦totheaffectedside.Thetrunkshouldalsobetilted backandthepatientshouldbeaskedtotrytoaccentuatethe
Fig.1–Schematicillustrationrepresentingthefrontal(A) andsuperiorview(B)ofthepatientandthechassis positioning,aswellastheincidenceangleofX-raysforthe modifiedaxillaryradiograph.
thoracickyphosis.Interestingly,thislateralinclinationofthe trunk, withaccentuationofthe thoracickyphosis, is natu-rallyadoptedbymostpatientssufferingfromglenohumeral dislocationwhenseated,whichmakestheexameasierand lesspainfulforthepatientasitrespectsthenaturalantalgic position.
Case
report
rev bras ortop.2017;52(1):115–118
117
Fig.2–Frontal(A)andlateral(B)photographsofthepatient fortheradiographicSennaposition.
reportedseverepainatanymanipulationoftheaffectedlimb. Theneurovascularexaminationoftheupperlimbswas unal-tered.Giventhe suspecteddislocationoftheglenohumeral joint,twoX-raysoftheleft shoulder,inorthogonalplanes, werenecessary.Inadditiontotheanteroposterior radiogra-phy, a modified axillary view (in the Senna position) was alsoobtained(Fig.2).Thelatterclearlyevidencedananterior glenohumeraldislocation.Thepatientunderwentsuccessful closedreductionthroughtractionandcountertraction.After reduction,anewradiographinSennapositionwasobtained,
Fig.3–Radiographsbeforereduction(A)andafterreduction (B)oftheglenohumeraldislocationofthepatientinFig.2.
whichconfirmedtheconcentricjointreduction(Fig.3).The patientwasthenimmobilizedwithaVelpeaushouldersling andreferredtooutpatienttreatment.
Final
remarks
The present modified axillary incidence was shown to be easytoperform,withminimaldiscomforttothepatient.The obtainedimagesclearlyevidenced theanatomical relation-shipbetweenthehumeralheadandglenoidcavityinanaxial view,andallowedforthesafeassessmentofglenohumeral dislocationanditsreduction.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
118
rev bras ortop.2017;52(1):115–1182.RoweC,ZarinsB.Chronicunreduceddislocationofthe shoulder.JBoneJtSurgAm.1982;64(4):494–505. 3.NeerCS2nd.Displacedproximalhumeralfractures.I.
Classificationandevaluation.JBoneJtSurgAm. 1970;52(6):1077–89.
4.JensenKL,RockwoodCAJr.Radiographicevaluationof shoulderproblems.In:RockwoodCAJr,MatsenFA3rd,Wirth
MA,LippittSB,editors.Theshoulder.Philadelphia:Saunders Elsevier;2004.p.188.
5.BloomMH,ObataWG.Diagnosisofposteriordislocationofthe shoulderwithuseofVelpeauaxillaryandangle-up
roentgenographicviews.JBoneJtSurgAm.1967;49(5):943–9. 6.CleavesEN.Anewfilmholderforroentgenexaminationsof