www.jped.com.br
ORIGINAL
ARTICLE
Lower
prevalence
and
greater
severity
of
asthma
in
hot
and
dry
climate
夽
Marco
Aurélio
de
Valois
Correia
Junior
a,b,∗,
Emanuel
Sávio
Cavalcanti
Sarinho
b,c,
José
Angelo
Rizzo
b,c,
Silvia
Wanick
Sarinho
baUniversidadedePernambuco(UPE),Petrolina,PE,Brazil
bUniversidadeFederaldePernambuco(UFPE),ProgramadePós-graduac¸ãoemSaúdedaCrianc¸aedoAdolescente,
Recife,PE,Brazil
cUniversidadeFederaldePernambuco(UFPE),DepartamentodeMedicinaClínica,CentrodePesquisaemAlergiaeImunologia
Clínica,Recife,PE,Brazil
Received11December2015;accepted30May2016 Availableonline5August2016
KEYWORDS
Asthma; Riskfactors; Allergicrhinitis; Adolescent; Epidemiology; Prevalence
Abstract
Objective: Toestimateasthmaprevalence,severity,andassociatedfactorsinadolescentswho liveinalowrelativehumidityenvironment.
Methods: Inthiscross-sectionalstudy,adolescentsaged13---14yearsfromthecityofPetrolina locatedintheBraziliansemiaridregionansweredtheInternationalStudyofAsthmaand Aller-giesinChildhood(ISAAC)questionnaire.Thepossibleexplanatoryvariablesofthestudywere gender, family income, mother’s education, smokers in the household, parental historyof asthma,personalhistoryofallergicrhinitisoratopicdermatitis,andphysicalactivitylevel. Pois-sonregressionanalysiswasusedtoassesstheassociationbetweenasthmaandtheexplanatory variables.
Results: A total of1591 adolescentsparticipated inthe study,of whom49.7% were male. Theprevalenceofactiveasthma,severeasthma,andphysician-diagnosedasthmawere14.0%, 10.4%,and17.8%,respectively.Adolescentswithasthmamissedmoreschooldaysthantheir peers(33vs.22days/year;p<0.03).Associatedfactorsthatremainedsignificantafter adjust-mentwerehistoryofasthmainparents(PR=2.65,p<0.001)andpersonaldiagnosisofallergic rhinitis(PR=1.96,p<0.001)and/oratopicdermatitis(PR=2.18,p<0.001).
夽
Pleasecitethisarticleas:CorreiaJuniorMA,SarinhoES,RizzoJA,SarinhoSW.Lowerprevalenceandgreaterseverityofasthmainhot
anddryclimate.JPediatr(RioJ).2017;93:148---55.
∗Correspondingauthor.
E-mail:[email protected](M.A.CorreiaJunior).
http://dx.doi.org/10.1016/j.jped.2016.05.006
Conclusion: Asthmaprevalenceinthislow-humidityenvironmentwaslower,butmoresevere thanthosereportedinotherBrazilian cities.Thedry climatemighthamperdisease control andthismayhavecontributedtothehigherschoolabsenteeismobserved.Theassociationof asthmawith allergicrhinitisandatopicdermatitisaswellasahistoryofasthmainparents suggeststhatatopyisanimportantriskfactorforasthmainthispopulation.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
PALAVRAS-CHAVE
Asma;
Fatoresderisco; Rinitealérgica; Adolescente; Epidemiologia; Prevalência
Menorprevalênciaemaiorgravidadedaasmaemclimaquenteeseco
Resumo
Objetivo: Estimaraprevalência,agravidadeeosfatoresassociadosàasmaemadolescentes quevivememumaregiãodebaixaumidaderelativadoar.
Métodos: Estudotransversalemadolescentesde13e14anosdosemiáridobrasileiro.Os partic-ipantesresponderamaoquestionárioInternationalStudyofAsthmaandAllergiesinChildhood (ISAAC).Asvariáveisexplanatóriasdoestudoforamsexo,rendafamiliar,escolaridadedamãe, fumantenaresidência,antecedentedeasmanosgenitores,antecedentesderinitealérgica, dermatiteatópicaeníveldeatividadefísica.AanálisederegressãodePoissonfoiutilizada paraavaliaraassociac¸ãoentreaasmaeasvariáveisexplanatórias.
Resultados: Participaramdapesquisa1.591adolescentes,sendo49,7%dosexomasculino.As prevalências para asma em atividade,asma grave e diagnóstico médico deasma foramde 14,0%,10,4%e17,8%,respectivamente.Adolescentesasmáticosfaltarammaisasaulasdoque seuspares(33vs22aulas/ano;p<0,03).Fatoresassociadosquepermaneceramsignificantes apósajuste foramantecedentesdeasmanosgenitores(RP=2,65, p<0,001),rinitealérgica (RP=1,96,p<0,001)e/oudermatiteatópica(RP=2,18,p<0,001).
Conclusão: Nesteambientedebaixaumidadeforamobservadasmenorprevalência,masmaior gravidadedaasmaqueaquelas relatadasem outrascidadesbrasileiras.Oclimasecotalvez possadificultarocontroledadoenc¸aeissopodetercontribuídoparaomaiorabsenteísmo esco-larnosdoentes.Aassociac¸ãoentrerinitealérgica,dermatiteatópicaeantecedentesdeasma nosgenitoressugeremqueaatopiaéimportantefatorderiscoparaaasmanestapopulac¸ão. ©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
Asthmaisacommonchronicinflammatoryairwaydiseasein childhood,clinicallycharacterizedbyrecurrentepisodesof wheezing,breathlessness,andcoughing.1Itisquite
preva-lent worldwide and climatic factors, especially humidity, canhaveanimportantroleindiseasedevelopment, consid-ering the low prevalence found in desert regions when comparedtoregionswherehumidityandrainfallarehigher, asintropicalregions.2---7
This characteristicmay be relatedto the proliferation ofhousedustmites,whichcannotsurvivein low-humidity environments and are a major determinant of allergic sensitization.4---10Inthiscase,indryclimateregions,other
agents rather than mites can be responsible for trigger-ingasthma; they includeother airborne allergens suchas pollen, air pollution, small particles present in soils, and animal epithelia, in addition tothe use of humidifiers in homes.4,8,9
In Brazil there is still scarce research on asthma and risk factors in differentregions of the country, especially regarding the different ecosystems.2,11 This fact makesit
difficult to plan and carry out public policies aimed at
prevention,astheexistingstudiesweremainlyperformed inlargermunicipalities,especiallyincapitalcities,mostof whicharelocatedonthecoastorinsubtropicalregionsin theSouth/Southeaststates.2,11
Thus,the aimof the studywastoevaluate the preva-lence, severity, and factors associated with asthma in adolescents aged 13---14 years residing in low-humidity regions,with hot anddry climate. The study wascarried outin a municipality whose climate is classified as semi-arid,characterizedbyscarceandirregularrainfallandhigh temperatures.
Methods
Thiswasacross-sectional, population-basedstudycarried outwithstudentsaged13 and14 years,enrolledin state publicschoolsin2014inthemunicipalityofPetrolina(state ofPernambuco)locatedinnortheasternBrazil,whichhasa populationofapproximately294,000inhabitants,12
occupy-inganareacorrespondingto4561.872km2.This studywas
Data werecollected through questionnairesapplied at schools and informationwas recorded in forms consisting ofpre-coded questions,containingquestionsonage, gen-der,allergicdiseases,physicalactivitylevel(PAL),maternal education, family income, presence of a smoker in the household,andhistoryofasthmaintheparents.The ques-tionnairesfilled outby the adolescentswere reviewed at the end of the day for identification and opportune cor-rectionofcompletionerrors;incomplete,questionable,or inconsistent datawere subsequently verifiedthrough new visits.
The ISAAC questionnaire, translated and validated for Brazil, was used for the evaluation of allergic diseases.2
This questionnaire has three modules (asthma, rhinitis, andeczema)withuptoeightquestionseach, andis self-applicableandeasytounderstand.Theauthorsconsidered for classification of asthma prevalence or active asthma those who answered ‘‘yes’’ to the question ‘‘In the last 12 months, have you had wheezing?’’. For the diagnosis of asthma, the authors considered those who answered ‘‘yes’’tothequestion‘‘Haveyoueverhadasthmainyour life?’’andforthediagnosisofsevereasthma,those adoles-centsclassifiedashavingactiveasthmawhoreportedchest wheezingthatwasstrongtothepointofaffectingspeech. Thisquestionnairedoesnotcontainquestionsregardingthe useofmedication.Thoseadolescentswhoanswered‘‘yes’’ tothefollowingquestionswereconsideredashavingrhinitis andatopicdermatitis,respectively:‘‘Inthelast12months, have youhad a problemwithsneezing, rhinorrhea(runny nose),andnasalobstruction,whenyoudidnothavetheflu oracold?’’and‘‘Inthelast12months,haveyouhadskin spots(eczema)?’’.
To assess the impact of asthma on the adolescents’ dailyactivities,absenteeismandoverallschoolperformance wereevaluated, aswellasactivity inthe physical educa-tionclasses.Schoolabsenteeismwasevaluatedbyobserving thetotal numberof missedschooldaysin each discipline throughtheschool attendancerecord relatedtothe year priortothestudy.Schoolperformance wasassessed using theaverageofthegradesobtainedduringtheyearpriorto thestudyincompulsorysubjects(mathematics,Portuguese, science,social sciences, and arts education), common to allschools.Thematernallevelofschoolingwas character-izedas0---9years,10---13years,andgreaterthan14 years ofschooling,whereasfamilyincomewascharacterizedas uptotwo minimumwagesand higherthan twominimum wages.
The level of physical activity was assessed using the InternationalPhysicalActivity Questionnaire(IPAQ--- short version)validated forBrazil,13 whichclassifiesthe
individ-ualasveryactive,active,irregularlyactive,or sedentary, according to the frequency, duration, and intensity of weekly physical activities. Individuals were considered active when they met the following criteria: (a) vigor-ous physical activity on ≥3 days/week, with a duration of at least 20min/session; (b) moderate physical activity or walking on ≥5 days/week, with duration of at least 30min/session; (c) any physical activity whose frequency was≥5days/week,withdurationofatleast150min/week. Subjects who did not meet the abovementioned criteria wereclassifiedasinactive.Writtenquestionnaireswere dis-tributed in classrooms and filled out by the adolescents
themselves,underthesupervisionofthepreviouslytrained researchers.
Samplesizeandstatisticalanalysis
The WinPepi program (PEPI-for-Windows)14 was used to
quantify thesample size accordingtothe following crite-ria: estimated population of 31,555 students; confidence interval of 95%;sampling error of five percentagepoints; estimatedprevalenceof50%,asthereweremorethantwo variablesofinterest;sampledesigneffectsetatthreetimes the minimumsizeof thesample; and sample lossof 20%, thereforetotalingaminimumsamplesizeof1425students. The sample selection procedure followed a sequence of steps in an attempt toobtain a representative sample of students from state schools regarding the distribution accordingtoschoolsize.Inordertoassistsampleplanning, schoolswereorganizedintothreecategories:small(upto 200students),medium-sized(201---499students)andlarge (morethan500students),andastratificationcriterionwas applied,consideringproportionalitybysize.
Afterallsteps,atotalnumberof18schoolsand57classes wasobtained,representing42%ofstateschoolsinPetrolina. Consideringaminimumof25studentsperclassroom,1425 students were expectedto beevaluated. As somegrades hadmore than25students perclassroom, atotalof 1591 studentswereevaluated.Theschoolswerechosenby draw-inglotsafterrandomizationcarriedoutusingtheWinPepi program.14
Data were processed and analyzed using SPSS, ver-sion20.0andStata 7.0(StataCorp.2015.StataStatistical Software:Release 7. CollegeStation, USA).Initially, data were entered into the statistical package SPSS using double entry and inconsistencies were compared. The Kolmogorov---Smirnov test wasappliedtotest the normal-ityassumption.The comparisonbetweenthemedianswas performedusingtheMann---Whitneytestfornon-parametric variables.Toassessthedifferencesbetweentheproportions ofasthmaandassociatedfactors,thechi-squaredtestand chi-squared test with Yates’s correction were used when appropriate. All conclusions were based on a significance levelof5%.
Prevalence ratios (PR) for asthma were calculated for each exposure variable by Poisson regression. The varia-bles with p-value<0.20 in the bivariate analysis were selected for the multivariate regression model, aimed to assesstheimpactoftheexplanatoryvariables.Theresults were expressed as adjusted prevalence ratios (PR) with their respective 95% confidence intervals (95% CI) and p -values<0.05wereconsideredstatisticallysignificant.
Results
Atotalof1591adolescentsaged13---14yearsparticipatedin thestudy,ofwhom791(49.7%)weremaleand800(50.3%) female;67.2%oftheirfamiliesearneduptotwominimum wagesandonly17.8%ofthemothershadcollege/university levelofschooling.
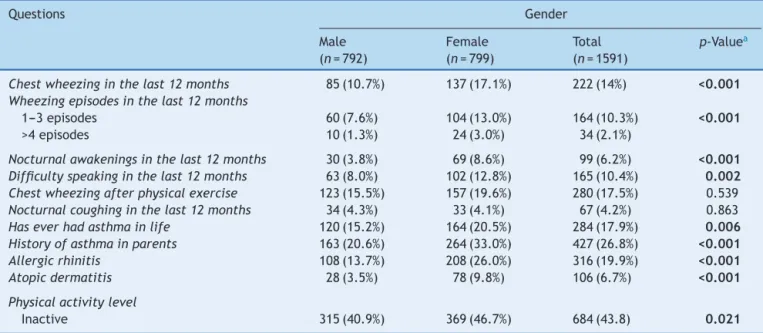
Table1 Distributionofstudentsbygenderandfactorsrelatedtoallergicdiseases.
Questions Gender
Male (n=792)
Female (n=799)
Total (n=1591)
p-Valuea
Chestwheezinginthelast12months 85(10.7%) 137(17.1%) 222(14%) <0.001 Wheezingepisodesinthelast12months
1---3episodes 60(7.6%) 104(13.0%) 164(10.3%) <0.001
>4episodes 10(1.3%) 24(3.0%) 34(2.1%)
Nocturnalawakeningsinthelast12months 30(3.8%) 69(8.6%) 99(6.2%) <0.001 Difficultyspeakinginthelast12months 63(8.0%) 102(12.8%) 165(10.4%) 0.002 Chestwheezingafterphysicalexercise 123(15.5%) 157(19.6%) 280(17.5%) 0.539 Nocturnalcoughinginthelast12months 34(4.3%) 33(4.1%) 67(4.2%) 0.863
Haseverhadasthmainlife 120(15.2%) 164(20.5%) 284(17.9%) 0.006
Historyofasthmainparents 163(20.6%) 264(33.0%) 427(26.8%) <0.001
Allergicrhinitis 108(13.7%) 208(26.0%) 316(19.9%) <0.001
Atopicdermatitis 28(3.5%) 78(9.8%) 106(6.7%) <0.001
Physicalactivitylevel
Inactive 315(40.9%) 369(46.7%) 684(43.8) 0.021
Valuesareexpressedinabsolutenumbersandpercentagesbetweenparentheses.Boldvaluesindicatestatisticaldifference.
a Chi-squaredtest.
asthma were 14.0%, 10.4%, and 17.8%, respectively, and thatfemaleadolescentshadahigherprevalenceofasthma, allergicrhinitis,anddermatitis(Table1).
The bivariate analysisof theactiveasthma prevalence andpossibleinterveningfactors(Table2)showedthe impor-tance of the association with allergic rhinitis and atopic dermatitis, as well as the history of asthma in the par-ents(28.2%vs.10.4%,35.8%vs.12.4%,and27.3%vs.8.3%, respectively,allwithp<0.001).
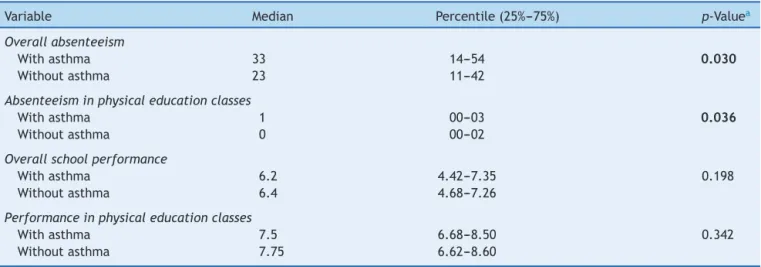
Adolescents with asthma missed more school days, including physical education classes, than their non-asthmatic peers (p<0.05). However, lower academic performancewasnotdetectedamongstudentswithasthma (Table3).
At the Poisson regression analysis, which included the femalegenderandalowerlevelofphysicalactivity,itwas observedthattheonlyvariablesthatremainedinthefinal modelwereallergicrhinitisandatopicdermatitis,aswell asahistoryofasthmaintheparents(Table4).
Discussion
The prevalence of asthma, severe asthma, and physician-diagnosed asthma in this study in the Brazilian semiarid regionwere14.0%,10.4%,and17.8%,respectively.The fac-torsassociatedwithasthmawereallergicrhinitisandatopic dermatitis, aswell asahistory of asthma in theparents; additionally,adolescentswith asthma missedmore school daysthantheirpeerswithoutasthma.
Climaticdifferencescanhaveasignificant influenceon asthmaprevalence,whichisdemonstratedbytheobserved higherprevalencein regionswithhigherrelativehumidity andrainfallandlowerprevalenceinregionswithhotanddry climates.2---6Whencomparingthesefindingswithstudies
car-riedoutinotherBrazilianlocations,2,11 alowerprevalence
of asthma was observed, possibly related to the specific climaticcharacteristicsofthestudiedregion.2---6Thedry
cli-matehindersthesurvivalofdustmites,themainhousehold allergens,whichrequirehydrationobtainedfromthe humid-ityoftheairtosurviveand,thus,environmentswithrelative humiditybelow55%arelethaltothem.6,9
However, as in this study, asthma is still detected in theseregions,andonepossibleexplanationisthepresence of other allergens, such as pollen and spores of plants,4
or contact withanimal epithelia and substances found in the soil that can be found suspended in the air, which, whenprocessedintosmallerparticles,canbetransportedby windsoverlongdistances.8Therehavebeenreportsof
aller-gic sensitizationin areas closeto pistachio plantations in thedesertinIran4andspeciesoffungihavebeendescribed
asthe agent with the highest association withasthma in semiaridclimatesinthedesert.15---17Allergicrespiratory
dis-easescausedbyplantsmayalsoexist,whichhavenotbeen yetidentified,inthisareainnortheasternBrazil,asoneof thecharacteristicsofthisresearchareaconsistsofirrigated fruitcropswithlargeplantationfields.
Another interesting fact is that although asthma is less prevalent in this locality, the asthmatic adolescents reportedahigherdegreeofdiseaseseverity,whichappears todirectlyaffectthelivesoftheseindividuals.Rabeetal.
18 describea negativeeffectof asthma withconsiderable
lossof work andschool daysinthe most severe cases,in additiontothefactthatcurrentcontrolaroundtheworldis farfromtheobjectivesestablishedintherecommendations ofinternationalguidelines.1
Infact,thehigherdegree ofschool absenteeismfound inthepresent study(33vs. 22schooldays/year;p<0.03) seems to be related to the severity of asthma, as the majority(74%)ofadolescentswithactiveasthma reported symptoms that were consistent with severe disease.8,18,19
Table2 Prevalenceofasthmainadolescentsaccordingtogender,familyincome,maternallevelofeducation,smokingstatus, historyofasthma,allergicrhinitis,atopicdermatitis,andlevelofphysicalactivity(totalnumberofassessedadolescents:1591).
PrevalenceofasthmaISAACquestionnaire
n % [95%CI] p-Valuea
Gender
Male 85 10.7 08.7---13.0 <0.001
Female 137 17.1 14.4---19.9
Familyincome
Uptotwominimumwages 147 13.8 11.8---15.8 0.388
Morethantwominimumwages 52 15.8 11.9---19.8
Maternallevelofschooling
0---9yearsofschooling 80 15.8 12.6---18.9 0.726
10---13yearsofschooling 72 12.5 09.8---15.3
>14yearsofschooling 44 15.6 11.7---19.9
Smokerinthehousehold
No 194 13.9 12.2---15.7 0.454
Yes 9 18 08.0---30.0
Historyofasthmainparents
No 105 9.0 07.5---10.6 <0.001
Yes 117 27.4 23.2---31.8
Allergicrhinitis
No 133 10.4 08.7---12.2 <0.001
Yes 89 28.2 23.7---33.5
Atopicdermatitis
No 184 12.4 10.7---13.9 <0.001
Yes 38 35.8 27.4---45.3
Physicalactivitylevel
Active 133 15.2 12.8---17.7 0.084
Inactive 83 12.1 09.8---14.8
CI,confidenceinterval.Boldvaluesindicatestatisticaldifference.
aChi-squaredtest.
Table3 Overallabsenteeism,absenteeisminphysical educationclasses,overall schoolperformance, andperformancein physicaleducationclassesbythestudents.
Variable Median Percentile(25%---75%) p-Valuea
Overallabsenteeism
Withasthma 33 14---54 0.030
Withoutasthma 23 11---42
Absenteeisminphysicaleducationclasses
Withasthma 1 00---03 0.036
Withoutasthma 0 00---02
Overallschoolperformance
Withasthma 6.2 4.42---7.35 0.198
Withoutasthma 6.4 4.68---7.26
Performanceinphysicaleducationclasses
Withasthma 7.5 6.68---8.50 0.342
Withoutasthma 7.75 6.62---8.60
Boldvaluesindicatestatisticaldifference.
Table4 Poissonregressionforasthmaprevalencebygender,historyofasthmainparents,allergicrhinitis,atopicdermatitis, andlevelofphysicalactivity.
Variable Unadjustedprevalenceratio Adjustedprevalenceratio
PR (95%CI) p PR (95%CI) p
Gender
Male 1 1
Female 1.60 1.22---2.09 <0.001 1.08 0.80---1.47 0.603
Historyofasthmainparents
No 1 1
Yes 3.28 2.47---34.34 <0.001 2.65 1.97---3.55 <0.001
Allergicrhinitis
No 1 1
Yes 2.70 2.06---3.53 <0.001 1.96 1.45---2.65 <0.001
Atopicdermatitis
No 1 1
Yes 2.89 2.04---4.10 <0.001 2.18 1.48---3.22 <0.001
Physicalactivitylevel
Active 1 1
Inactive 0.80 0.61---1.05 0.084 0.86 0.64---1.15 0.318
CI,confidenceinterval;PR,prevalenceratio.Boldvaluesindicatestatisticaldifference.
controlofthediseaseand,moreover,itispossiblethatin thehot,dryclimate, patientshaveamoresevere disease phenotype.Modelsshowingasthmatriggeringafterexercise withpatientsbreathingdryairsuggestthatbronchospasms maybemoresevereundertheseconditions.21,22
Evenwithalowerprevalenceofasthmathanthenational average(14%vs.19%),2thediseaseinthislocationseemsto
have a more severe presentation (10.4%) when compared totherestofBrazil(4.7%)2andtheworld(6.9%).11Studies
indesert regionsof Saudi Arabia5,23 haveshown agreater
numberofvisitstotheemergencyroominindividualswith asthma when compared to individuals living in European cities(62%vs.24%),24indicatinganassociationwithgreater
diseaseseverityintheseareas,whichmayberelatedtothe availabilityofcare,aswellastotheclimaticcharacteristics oftheregion.
Data fromthe InformaticsDepartment of theBrazilian UnifiedHealthSystem(DepartamentodeInformáticado Sis-temaÚnicodeSaúde[DATASUS])showthatthenumberof hospitaladmissionsforasthmaduringtheseven-yearperiod inPetrolinaishigherthaninmunicipalitieslocatedonthe coastandinthehinterlandsofthestateofPernambucowith asimilarpopulationsize.Thestandardized hospitalization rateper100,000inhabitants was509.4 inPetrolina (semi-aridregion),259.58inCaruaru(hinterlands),and180.53in Paulista(coastalregion).12 Thisisanalarmingscenariofor
asthmainthisregion,whichseemstobeeffectivelymore severeandpredominantly allergic,asit isstrongly associ-ated with other characteristics of atopy, such as allergic rhinitisandatopicdermatitis.
Inthisstudy,afteradjustmentofvariables,the associa-tionofasthmawithallergicrhinitis(prevalenceratio=1.96) was lower than that found in other Brazilian studies (reported valuesbetween 2.19 and 4.36)25; nevertheless,
together withatopic dermatitis,it was stillan important
factorforthediagnosisofasthmainthispopulation.These findingssuggestthatevenina dryandhotclimate,atopy appearstobepresentasamajorfactor.Anadditionalfact, besidesthisassociation withotherallergicdiseases,isthe reportofahistoryofasthmaintheparentsasaconsistent factorassociatedwiththeprevalenceofdisease,which con-tributedtoaprevalenceratioof2.65.Thismaysuggestthe need toalert adults withasthma to identifysigns of this diseaseintheirchildrenandcontribute,togetherwiththe healthcarestaff,toearlyandadequatecare.19,20,26
Itisimportanttoconsidersomelimitationsofthisstudy. Theuseofquestionnairescanresultinsomerecalland/or interpretationbias,andtherearetemporalgapsthatexist betweenmulticentricISAACtrialsinBrazil.27,28Studies
car-riedoutalmosttenyearsagointhesamestate,usingsimilar methodology,butinplaceswithverydifferentclimatic con-ditions,showeddifferencesinprevalencebetweenthemore humidregionofthecoast(19.1%),theintermediateregion oftheBrazilianhinterlands(17.9%),andthecurrentstudy, carriedoutinthesemiaridregion(14%).2
Additionally,variablesnotincludedinthestudy---suchas eatinghabits, atopic sensitization, andpsychological fac-tors--- can influence the occurrenceof asthma.26,29,30 The
factthattheISAACquestionnairedoesnotcontainquestions abouttreatmentdoesnotallowformakinginferencesabout apossibleassociationbetweentheprevalenceofasthmaor evenobserved severeasthma andtheuseof medications, eventhoughtheyhavebeenprescribed,mightnothavebeen objectivelyused.However,theresultsdescribedhereincan helptounderstandtheprevalenceofasthmaanditsseverity inhot,dryclimates.
callingattentiontothehighproportionofreportsofmore severediseasesymptoms.2,27,28Consideringtheresponsesto
theISAACquestionnaire,itcanbeinferredthatasthma,at leastforthephysicians,isnotaneglecteddisease,asthe frequencyofphysician-diagnosedasthma ishigher(17.9%) tothat of wheezing in the last year (14%); however, this isnoguaranteethatpatientswillbetreatedappropriately. The low airhumidity andlack ofclinical control are pos-sible explanations for this finding. These data should be usedtoguidehealthpoliciesundersimilarconditions,and furtherstudiesshouldbeconductedtoassesswhetherthe improvementinmedicalcarewillreducethenumberof hos-pitalizationsandvisits toemergencyroomsduetoasthma thatwerefoundinthisstudy.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
TheauthorswouldliketothankProfessorDirceuSoléforhis invaluablecontributionsinreviewingthetext.
References
1.GlobalStrategyforAsthmaManagementandPrevention.Global
InitiativeforAsthma(GINA)2015.[Cited2015Nov08].Available
from:http://www.ginasthma.org
2.Solé D,WandalsenGF,Camelo-NunesIC,Naspitz CK,ISAAC -BrazilianGroup.Prevalenceofsymptomsofasthma,rhinitis, and atopiceczemaamongBrazilianchildrenandadolescents identified bytheInternational StudyofAsthma andAllergies in Childhood (ISAAC) --- Phase 3. J Pediat (Rio J). 2006;82: 341---6.
3.LimFL,HashimZ,ThanLT,MdSaidS,HishamHashimJ,Norbäck D.Asthma,airway symptomsandrhinitisinofficeworkersin Malaysia:associationswithHouseDustMite(HDM)allergy,cat allergyandlevelsofhousedustmiteallergensinofficedust. PLoSOne.2015;10:1---21.
4.Farajzadeh S, Esfandiarpour I, Sedaghatmanesh M, Saviz M. Epidemiology and clinical features of atopic dermatitis in kerman, a desert area of Iran. Ann Dermatol. 2014;26: 26.
5.Moradi-LakehM,ElBcheraouiC,DaoudF,TuffahaM,Kravitz H, AlSaeedi M,etal. PrevalenceofasthmainSaudiadults: findingsfromanationalhouseholdsurvey,2013.BMCPulmMed. 2015;15:77.
6.PortnoyJ,MillerJD,WilliamsPB,ChewGL,MillerJD,Zaitoun F, et al. Environmental assessment and exposure control of dustmites:apracticeparameter.AnnAllergyAsthmaImmunol. 2013;111:465---507.
7.BarretoBA,SoleD.Prevalenceofasthmaandassociatedfactors inadolescentslivinginBelem (Amazonregion), Para,Brazil. AllergolImmunopathol(Madr).2013;42:427---32.
8.D’AmatoG,HolgateST,PawankarR,LedfordDK,CecchiL, Al-AhmadM,etal.Meteorologicalconditions,climatechange,new emergingfactors,and asthmaand relatedallergicdisorders. AstatementoftheWorldAllergyOrganization.WorldAllergy OrganJ.2015;8:25.
9.ArlianLG,MorganMS.Biology,ecology,andprevalenceofdust mites.ImmunolAllergyClinNAm.2003;23:443---68.
10.Andiappan AK, PuanKJ, Lee B,Nardin A, PoidingerM, Con-nolly J, et al. Allergic airway diseases in a tropical urban
environmentaredrivenbydominantmono-specificsensitization againsthousedustmites.Allergy.2014;69:501---9.
11.Lai CK, Beasley R, Crane J, Foliaki S, Shah J, Weiland S, et al. Global variation in the prevalence and severity of asthmasymptoms:phasethreeoftheInternational Studyof Asthmaand Allergies inChildhood (ISAAC). Thorax.2009;64: 476---83.
12.Brasil.MinistériodaSaúdeBancodedadosdoSistema Único deSaúde-DATASUS.2015.[cited08Nov2015].Availablefrom:
http://www.datasus.gov.br
13.Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, AinsworthBE,et al. International physicalactivity question-naire:12-countryreliabilityandvalidity.MedSciSportExerc. 2003;35:1381---95.
14.AbramsonWINPEPIupdated:computerprogramsfor epidemiol-ogists,andtheirteachingpotential.EpidemiologicPerspectives &Innovations20118:1.
15.Halonen M, Stern DA, Wright AL, Taussig LM, Martinez FD. Alternaria as a major allergen for asthma in children raised ina desert environment. AmJ RespirCritCare Med. 1997;155:1356---61.
16.KanataniKT,AdachiY,SugimotoN,NomaH,OnishiK,Hamazaki K,etal.Birthcohortstudyontheeffectsofdesertdust expo-sureonchildren’shealth:protocolofanadjunctstudyofthe JapanEnvironment&Children’sStudy.;Children’sStudy.BMJ Open.2014;4:1---8.
17.Mulitza S, Heslop D, Pittauerova D, Fischer HW, Meyer I, StuutJB,et al.IncreaseinAfrican dustfluxat theonsetof commercialagricultureintheSahelregion.Nature.2010;466: 226---8.
18.RabeKF,AdachiM,LaiCK,SorianoJB,VermeirePA,WeissKB, etal.Worldwideseverityandcontrolofasthmainchildrenand adults:theglobalasthmainsightsandrealitysurveys.JAllergy ClinImmunol.2004;114:40---7.
19.Shendell DG, Alexander MS, Sanders DL, Jewett A, Yang J. Assessing the potential influence of asthma on student attendance/absenceinpublicelementaryschools.JAsthma. 2010;47:465---72.
20.Tsakiris A, Iordanidou M, Paraskakis E, Tsalkidis A, Rigas A, ZimerasS,etal.Thepresenceofasthma,theuseofinhaled steroids, and parental education level affect school perfor-manceinchildren.BiomedResInt.2013;2013:1---7.
21.ParkHK,JungJW, ChoSH,Min KU,KangHR. Whatmakesa differenceinexercise-inducedbronchoconstriction:an8year retrospectiveanalysis.PLoSOne.2014;9:e87155.
22.EschenbacherWL,MooreTB,LorenzenTJ,WegJG,GrossKB. Pulmonaryresponsesofasthmaticandnormalsubjectsto differ-enttemperatureandhumidityconditionsinanenvironmental chamber.Lung.1992;170:51---62.
23.Al-Moamary MS, Alhaider SA, Al-Hajjaj MS, Al-Ghobain MO, IdreesMM,ZeitouniMO,etal.TheSaudiinitiativeforasthma --- 2012 update: guidelines for the diagnosis and manage-ment of asthma in adults and children. Ann Thorac Med. 2012;7(4):175---204.
24.PriceD,FletcherM,VanderMolenT.Asthmacontroland man-agementin8,000Europeanpatients:theREcogniseAsthmaand LInktoSymptomsandExperience(REALISE)survey.NPJPrim CareRespirMed.2014;24:14009.
25.SoléD,Camelo-NunesIC,WandalsenGF,RosárioNA,SarinhoEC. Isallergicrhinitisatrivialdisease?Clinics.2011;66:1573---7.
26.Cantani A, Micera M. A study on 300 asthmatic children, 300 controls and their parents confirms the genetic trans-mission of allergy and asthma. Eur Rev Med PharmacolSci. 2011;15:1051---6.
28.Garcia-MarcosL,Pacheco-GonzalezR.Asequelofthe Interna-tionalStudyofAsthmaandAllergiesinChildhoodoraprelude to the Global Asthma Network? J Pediatr (Rio J). 2015;91: 1---3.
29.DanansuriyaMN,RajapaksaLC,WeerasingheA.Genetic, famil-ial and environmental correlates of asthma among early
adolescentsinSriLanka:a casecontrolstudy.WorldAllergy OrganJ.2015;8:19.