Arq. Gastroenterol. vol.47 número1
Texto
Imagem
Documentos relacionados
We conclude that: 1 – the professionals evaluated feel com- fortable in addressing the most prevalent and low complexity rheumatic diseases; 2 – The knowledge of clinical
In the GAgP group, individuals were categorized according to the IL-6 and IL-10 genotype distribution, and then changes in clinical and biochemical parameters were evaluated
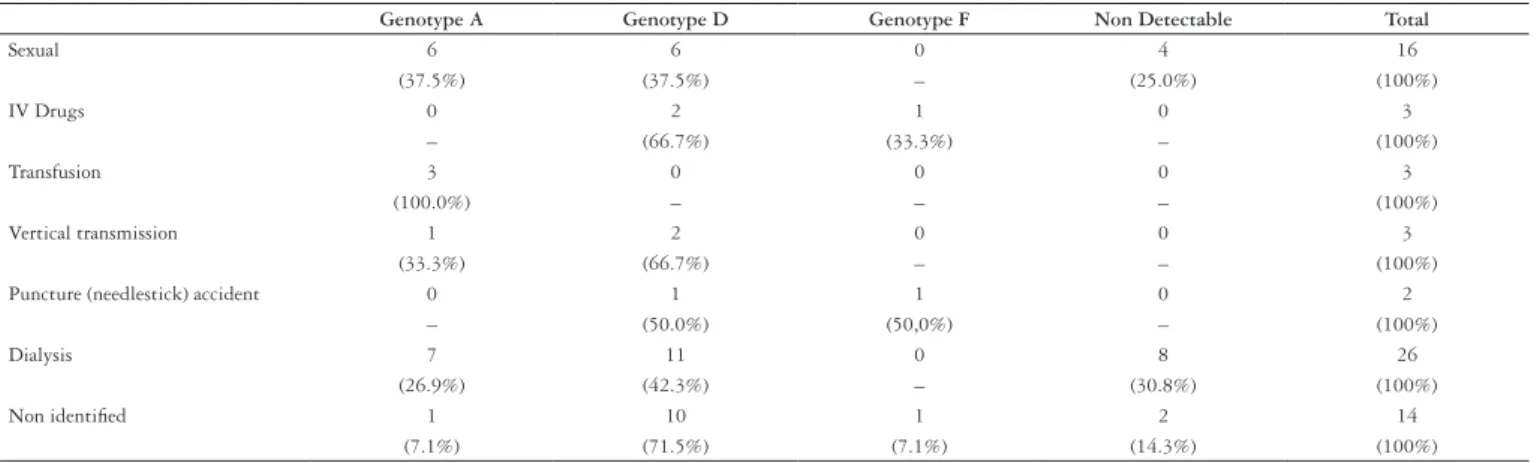
In this study, we evaluated the hepatitis B virus (HBV) genotype distribution and HBV genomic mutations among a group of human immunodeficiency virus-HBV co-infected patients from
For leaf nitrogen content (NC), a significant interaction was seen between the methods for supplying nitrogen and genotype, suggesting that the responses of the evaluated genotypes
Table 3 - Response to grain yield of 20 cowpea genotypes evaluated in 47 locations and three years, according to the overall average, genotypic values free from the interactions,
We observed that the pattern of load distribution and the objectives outlined in the mesocycles (Table 1) are similar to the concepts of block periodization, which proposes
When we analyzed the pondero-statural growth of these children, we observed, in our statistics, that the majority of the children studied had a z score > -2, when the breastfed
When using a difference of d” 2 mm between the right and left forearm readings as a criterion, we observed that concordance was achieved in only 40.5% (17/42), and that the
