REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
REVIEW
ARTICLE
Analgesic
efficacy
of
the
ultrasound-guided
blockade
of
the
transversus
abdominis
plane
---
a
systematic
review
Javier
Ripollés
a,∗,
Sandra
Marma˜
na
Mezquita
b,
Alfredo
Abad
c,
José
Calvo
aaServiceofAnesthesiologyandReanimation,HospitalUniversitarioInfantaLeonor,Madrid,Spain
bServiceofAnesthesiologyandReanimation,HospitalUniversitarioMoisésBroggi,SantJoanDespí,Barcelona,Spain
cServiceofAnesthesiologyandReanimation,HospitalUniversitarioLaPaz,Madrid,Spain
Received23July2013;accepted31October2013 Availableonline25October2014
KEYWORDS
TAPblock; Transversus abdominisplane; Ultrasoundguided; Sistematicreview
Abstract
Background: Thetransverseabdominalplanblockadeisablockofabdominalwallthathas
diff-usedrapidlyintheclinicalpracticeaspartofamultimodalanalgesiaforabdominalsurgery.
The performanceoftheultrasound-guided techniquehasallowed thelowering ofpotential
complications, aswell as new approachesthat were carried out according to the
descrip-tions,andtheprospectivestudieswouldmakeitpossibletoutilizethetransverseabdominal
planblockadeindifferentsurgicalinterventions;however,theresultsobtainedinrandomized
clinicaltrialsareinconsistent.
Objectives: Toprepareasystematicreviewaimingtodeterminetheefficacyofthe
ultrasound-guidedtransverseabdominalplanblockadefordifferentsurgicalinterventions,aswellasthe
indicationsaccordingtotheapproachesandtheirinfluences.
Methods:Tworesearchapproaches,onemanual,andtheotherinPubmedreturned28
ran-domizedclinicaltrialswhereinterventionwithultrasound-guidedtransverseabdominalplan
blockadeswasperformedtocomparetheanalgesicefficacyincontrasttoanothertechniquein
adults,publishedbetween2007andOctober2013,inEnglishorSpanish,withJadadscore>1,
accordingtotheinclusioncriteriaforthisreview.Theauthorsanalyzedindependentlyallthe
randomizedclinicaltrials.
Conclusions: Thetransverseabdominalplanblockadeshavebeenshowntobeaneffective
tech-niqueincolorectalsurgery,cesareansection,cholecystectomy,hysterectomy,appendectomy,
donornephrectomy,retropubicprostatectomy,andbariatricsurgery.However,thedatafound
inrandomizedclinicaltrialarenotconclusive,andasaresult,itisnecessarytodevelopnew
andwelldesignedrandomizedclinicaltrial,withenoughstatisticalpowertocomparedifferent
approaches,drugs,doses,andvolumesforthesameintervention,aimingtoanswerthecurrent
questionsandtheireffectsinthehabitualclinicalpractice.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights
reserved.
∗Correspondingauthor.
E-mails:[email protected],[email protected](J.Ripollés).
0104-0014/$–seefrontmatter©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
BloqueioTAP; Planotransversodo abdome;
Ecoguiada;
Revisãosistemática
Eficáciaanalgésicadobloqueioecoguiadodoplanotransversodoabdome---revisão sistemática
Resumo
Justificativa:Obloqueiodoplanotransversoabdominal(TAP)éumbloqueiodaparede
abdom-inalquesedifundiurapidamente napráticaclínicacomo partedeanalgesiamultimodalem
cirurgiaabdominal.Atécnicaecoguiadapermitiureduziraspossíveiscomplicac¸ões,assimcomo
asnovasabordagens,que,deacordocomasdescric¸õesfeitaseosestudosprospectivos,
per-mitiramusaroTAPemváriosprocedimentoscirúrgicos;noentanto,osresultadosobtidosem
ensaiosclínicosrandomizados(ECR)sãoinconsistentes.
Objetivos: Revisão sistemáticapara determinar aeficácia analgésica do TAPecoguiado em
diversosprocedimentoscirúrgicos,assimcomodeterminarasindicac¸õesdeacordocom
abor-dagensesuainfluência.
Métodos: FoifeitaumapesquisanoPubMedeoutralivreeforamencontrados28ECRemque
intervenc¸ãocomoTAPecoguiadoerafeitaesecomparavasuaeficáciaanalgésicacomoutra
técnicaemhumanosadultos,publicadosentre2007eoutubrode2013comescoredeJadad
>1,eminglêsouespanhol,deacordocomoscritériosdeinclusãoparaestarevisão.Todosos
ECRforamanalisadosdeformaindependentepelosautores.
Conclusões:OTAPmostrouserumatécnicaeficazemcirurgiacolorretal,cesárea,
colecistec-tomia,histerectomia,apendicectomia,nefrectomiaemdoador,prostatectomiaretropúbicae
cirurgiabariátrica.Noentanto,osdadosencontradosnosECRsãoinconclusivos,demodoque
maisECRbemdesenhadossãonecessáriosecompoderestatísticosuficientenacomparac¸ãode
diferentesabordagens,drogas,dosesevolumesparaumamesmaintervenc¸ão,afimderesolver
ostemasdaatualidadeeseuimpactonapráticaclínicahabitual.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos
direitosreservados.
Introduction
Theblockofthetransversusabdominisplane(TAP)hadbeen firstdescribed asa blockof the abdominalwallbased on anatomical references to introduce local anesthetic (LA) inthe TAPthroughthePetittriangle byloss ofresistance technique.1In2007thefirstdescriptionofthe ultrasound-guidedTAPappeared,2anditsusehasbecomepopularsince theninhighandlowabdominalsurgeries,althoughithasnot beenfullyintegratedintheregularclinicalpractice.3 The apparitionoftheultrasound-guidedtechniquehasallowed the reduction of block failure risk, unacceptably high in theanatomicaltechnique4aswellasreductionofpossible complicationsassociatedwiththistechnique5 eventhough they have been described6 but probably underestimated becauseofpublicationbias.
Theuseofultrasonographyhasallowedthedevelopment ofnewapproaches, likethesubcostal, theposterior,7 the obliquesubcostal,8 or combinations like the dual TAP9 in whichthepossibilitiesofTAPhavebeenincreased.However, currently there is no recommendation for the use of the ultrasound-guidedTAPincomparisontotheclassicTAP10due toalackofrandomizedclinicaltrials(RCTs)thattestboth techniques.11
Potentially,theinjectionofLAatthislevelprovides anal-gesia in the skin, muscles and parietal peritoneum from T7toL1, onceit blocksthe afferentneuronal endingsof theabdominalwalls.However,currentlythereisa contro-versy inthe specialized literaturein relation tothe level ofdistributionof the localanesthetic withasingle injec-tion, since some studies demonstrate an extension from
T7 to L112 and others, an extension from T10 to L1.13 The greatestextensiondemonstratedwiththe ultrasound-guided technique is T7 with oblique subcostal TAP, T9 with the classic mid-axillary approach, and paravertebral extension from T4 to L1 with the posterior approach.14 Thereby, themid-axillaryTAPshouldbeusedfor infraum-bilical surgeries, the subcostal for periumbilical, and the oblique subcostal in supraumbilical incisions between T7 and T9.15 In fact, the RCTs are poorly correlated to the expectedextensionandnotalwaysconclusive.Considering studies of contrastdistribution15 it is possible tosuppose thatthediffusionoftheinjectedsubstancewillvary accord-ingtotheapproach,withdifferentresultsthatmayaffect theanalgesia.Thecurrentliteratureshowsthatnotallthe blockades are equal, and that the approach significantly alterstheblockade’s pharmacodynamicsandtheresultant analgesia characteristics. Currently, it is recognized that themoreposteriorapproaches,inotherwords,the instal-lation of the needle closer to the traditional approach, based on non-ultrasound-guided original, gives rise to a wider analgesia in terms of dermatomes and the tempo-ral block probably due to the block of the sympathetic ganglia in the thoracic paravertebral space.16 The more anterior approaches provide an analgesia in the abdom-inal wall in line with the pharmacokinetics of the LA used.
in prospective studies in liver transplantation45 and in prostatectomy.46
ItisimportanttonotethatinspiteofTAPproviding anal-gesiaintheskin,subcutaneousandparietalperitoneum,it should bealways executed asan extra component in the multimodalanalgesia,becauseitisnoteffectiveinthe con-trolofvisceralpain.47,48
Due to the fact that diverse techniques and interven-tions in which the ultrasound-guided TAP has been used, itsindicationsarenotdetermined.49 The objectiveof this reviewistodeterminetheefficacyoftheultrasound-guided TAPfordifferentsurgicalinterventionsinthoseRCTswhere ultrasound-guidedTAPhasbeen executed, andtoobserve howit affectsthe analgesia.It alsoinvestigates the indi-cations according to the approaches, their influence, the influenceofTAPduration,andthedoseandtypeoftheused LA,inadditiontocomplicationsandtheassessment,orits lack,oftheblockade’ssensitivelevel.
Methods
A systematic review about the analgesic efficacy of the ultrasound-guided TAPis performed according to the rec-ommendationestablishedbyPreferredReportingItemsfor SystematicreviewsandMeta-Analysis(PRISMA).50
The authors searched in the US National Library of Medicine database (MEDLINE) for the terms «TAP block», «Transversus Abdominal Plane Block», «Transversus Abdo-minis Plane Block», «Bloqueo del Plano Transverso del Abdomen» and «Bloqueo TAP», as well as manually. The searchwasrestricted toprospectiveRCTinhumans, pub-lishedbetweenJanuary2007andOctober 2013,inEnglish or Spanish. The found RCTs were evaluated in order to identifythoseinwhichultrasound-guidedTAPiscompared to another analgesic modality in adult patient. The RCTs withJadadscore<251 (Fig.1)werenotincluded.TheRCTs selectedforthesystematicreviewweretheonesinwhichan interventionisperformedwithultrasound-guidedTAPsthat comparetheanalgesicefficacyinrelationtoanother tech-niqueinadulthumans,publishedbetween2007andOctober 2013,inEnglishorSpanish,withJadadscore>1.Thereare RCTsinwhichtheanalgesicefficacyisevaluatedaccording totheapproachbasedonreferencesorattendedbya sur-geon.However,inthisreview,theauthorslimitedthesearch toRCTwithultrasound-guidedTAPsincetheyconsiderthat currentlythistechniqueshouldbethetechniqueofelection, becauseof the diminution of blockfailure, the avoidable complications with the ultrasound-guided technique, and thegreaterpossiblevarietyofapproaches.
Two independent investigators (J. Ripollés and S. Marma˜na)reviewedeacharticleinordertodeterminethe
eligible ones. The investigators have extracted the data independentlybymeansoftablesmadeforthispurposeand solved discrepancies before analyzing the results. Demo-graphic data, which included author,year of publication, participant,intervention,outcomes,designandJadadscore wereextracted fromthe included RCT (Table 1). Forthe analysisoftheanalgesicefficacy,thedataextractedwere: painscoreatrestandinearlyandlatemovement,earlyand lateconsumptionofanalgesic(bymeansof<12hasearlyand >12h aslate),timeuntilrescue analgesia,and secondary effectsofopioids:postoperativenauseaandvomit(PONV), sedationanditching(Table2).Ananalysisofthetechnique usedfortheTAPwasperformed,including:typeofsurgery, typeof block, duration, laterality of the block, the nee-dle used, drug, doses and volume utilized, supplemental analgesiaadministered,identificationofsensitiveleveland complicationsassociatedwiththeTAP(Table3).Theuseof mid-axillaryapproachisassumedinthosetrialsinwhichit hasnotbeenspecified.
TheprobabilityofmethodologicalbiasofeachRCTwas independentlyevaluatedbytwoauthors,adoptingtheJadad score.
Results
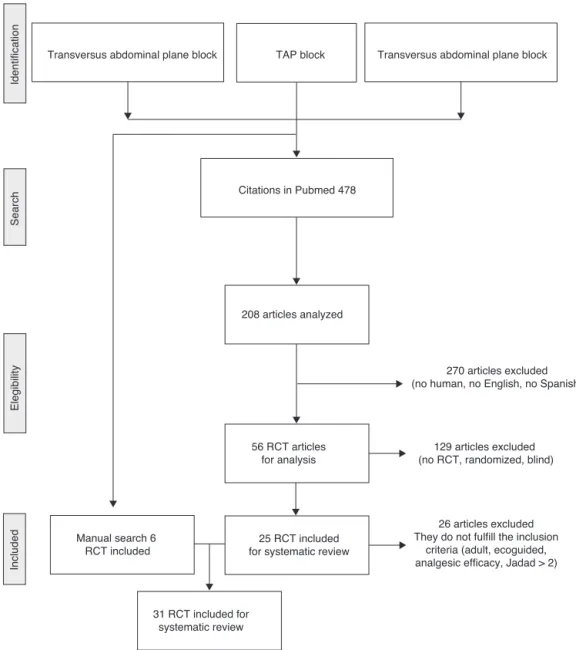
Thirty-oneRCTswereobtained,whichalignedwiththe inclu-sioncriteriaforthesystematicreview,17---44A,D,C,including 2193patients.TheflowdiagramoftheselectionoftheRCT isshowninFig.2.
The RCTswere dividedintosubgroupsaccordingtothe typeofthesurgeryinwhichTAPwasusedforitsanalysis: colorectal,17,18 cesarean,19---28 cholecystectomy,28---33 hyste-rectomy,34---37 inguinal herniorrhaphy,38---40 appendectomy,41 nephrectomy,42,43bariatric,44,45gastrectomy46 and retropu-bicprostatectomy.47 Ofthearticlesincluded, 93.5%hada goodqualityaccordingtoJadadscore.
ThecharacteristicsoftheRCTincludedinthesystematic reviewareshowninTable1.
Interventionandsurgery
Theultrasound-guided TAPincolorectalsurgerywas eval-uated in 2 RCTs,17,18 in which the TAP was compared to TAP vs. epidural anesthesia17 and TAP vs. placebo TAP18; inthefirstcase,itisspecifiedforhighabdominalsurgery, whereasinthesecondRCT,ananalysisofsubgroupsis per-formed distinguishing in left(supraumbilical incision) and right (infraumbilical incision). In the first RCT,17 a sub-costalpostoperativeapproachisutilized,andnodifferences were found between visual analog scale (VAS) score for painat rest or in movement in the first 72h withTAP or
Does the study describe itself as randomized? Yes = 1 point; No = 0 points
Is the method utilized for producing the sequence of randomization described? and Is this method appropriate? Yes = 1 point; No = 0 points; the method is not appropriate = - 1 point
Does the study describe itself as double-blind? Yes = 1 point; No = 0 points
Is the blinding method described? and Is this method appropriate? Yes = 1 point; No = 0 points; the method is not appropriate = - 1 point Is there a description of withdrawals and dropouts?
Yes = 1 point; No = 0 points This questionnaire returns a punctuation in a scale that goes from 0 to 5, so that the higher punctuation means that the evaluated RCT has a better methodological quality. Rigorous 5 points; low quality < 3 points.
J.
Ripollés
et
Table1 PICOs(Patient,Intervention,Comparison,Outcome).
Surgery
Author,year
N Intervention Comparison Outcome Design JadadScore
C.colorectal
Nirajetal.,201117 62 BilateralTAPwithcatheter
inhighabdominalsurgery
TAPvs.epidural VASpainscoreatrestandin movementinthefirst72h
Randomizeddouble-blind trial
5
Walteretal., 201318
68 BilateralTAPinc.colorectal TAPvs.noTAP Consumptionofopioidsin thefirst24h
Randomizeddouble-blind trial
5
Cesarean Belavyetal., 200919
57 BilateralTAPincesarean withspinalanesthesia
TAPvs.placebo TAP
Consumptionofopioidsin thefirst24h
Randomizedblindtrial 5
Costelloetal., 200920
96 BilateralTAPincesarean withspinalanesthesiawith ITM
TAPvs.placebo TAP
VASpainscoreatrestandin movementinthefirst24h
Randomizeddouble-blind trial
5
Baajetal.,201021 40 BilateralTAPincesarean withspinalanesthesia
TAPvs.placebo TAP
Consumptionofopioidsin thefirst24h
Randomizeddouble-blind trial
3
Kanazietal., 201022
57 ITMincesarean TAPvs.
ITM+placeboTAP
Timeuntiltheopioidrescue Randomizeddouble-blind trial
4
Loaneetal.,201223 66 BilateralTAPincesarean underspinalanesthesia
TAPvs.
ITM+placeboTAP
Consumptionofopioidsin thefirst24h
Randomizeddouble-blind trial
5
Tanetal.,201224 40 BilateralTAPincesarean withgeneralanesthesia
TAPvs.placebo TAP
Consumptionofopioidsin thefirst24h
Randomizeddouble-blind trial
5
Bollagetal., 201225
90 BilateralTAPwithclonidine incesareanwithspinal anesthesia
clonidineTAPvs. TAPvs.placebo TAP
Hyperalgesiaindexofthe woundfollowingTAP
Randomizeddouble-blind trial
5
Eslamianetal., 201226
50 BilateralTAPincesarean withgeneralanesthesia
TAPvs.noTAP VASpainscoreatrestandin movementinthefirst24h
Randomizeddouble-blind trial
5
Cánovasetal., 201327
90 BilateralTAPincesarean withspinalanesthesia
TAPvs.placebo TAPvs.
ITM+placeboTAP
VASpainscoreatrestandin movementinthefirst24h
Randomizeddouble-blind trial
5
Leeetal.,201328 51 BilateralTAPincesarean withspinalanesthesiawith ITM
TAPvs.placebo TAP
VASpainscoreinmovement inthefirst48h
Randomizeddouble-blind trial
5
Cholecystectomy El-Dawlatlyetal., 200929
42 BilateralTAPinlaparoscopic cholecystectomy
TAPvs.noTAP Consumptionofopioidsin thefirst24h
Randomizeddouble-blind trial
3
Raetal.,201030 54 BilateralTAPinlaparoscopic cholecystectomy
TAPvs.placebo TAP
Numericalandverbalpain scoreinthefirst24h
of
ultrasound-guided
transverse
abdominal
plan
blockade
259
Table1(Continued)
Surgery
Author,year
N Intervention Comparison Outcome Design JadadScore
Petersenetal.,
201231
80 BilateralTAPinlaparoscopic cholecystectomy
TAPvs.placebo TAP
VASpainscoreinmovement inthefirst24h
Randomizeddouble-blind trial
5
Ortizetal.,201232 80 BilateralTAPinlaparoscopic cholecystectomy
TAPvs.infiltration VASpainscoreinthefirst 24h
Randomizedblindtrial 3
Tolchardetal., 201233
43 BilateralTAPinlaparoscopic cholecystectomy
TAPvs.infiltration Consumptionofopioidsin thefirst24h
ReductionofVAS
Randomizeddouble-blind trial
5
Gynecological Griffithsetal., 201034
65 BilateralTAPinoncologic gynecologicalsurgery
TAPvs.placebo Consumptionofopioidsin thefirst24h
ReductionofVAS
Randomizeddouble-blind trial
5
Atimetal.,201135 55 BilateralTAPin hysterectomy
TAPvs.TAP placebovs.local infiltration
VASpainscoreatrestandin movementinthefirst24h
Randomizeddouble-blind trial
2
DeOliveiraetal., 201136
75 BilateralTAPin gynecologicalc. laparoscopic
TAPvs.placebo TAP
QoR-40satisfactionscore Randomizeddouble-blind trial
5
Kaneetal.,201237 56 BilateralTAPin
laparoscopichysterectomy
TAPvs.noTAP SatisfactionscoreQoR-40 Randomizedblindtrial 3
H.inguinal Avelineetal., 201138
275 UnilateralTAPininguinal herniorrhaphy
TAPvs.b. ileoinguinal-ileohipogastric
VASpainscoreatrestandin movementinthefirst24h
Randomizedblindtrial 3
LópezGonzález etal.,201339
41 UnilateralTAPininguinal herniorrhaphy
TAPvs.infiltration VASpainscoreatrestand immovementinthefirst 24h
Randomizedblindtrial 2
Petersenetal., 201340
90 UnilateralTAPininguinal herniorrhaphy
TAPvs.Placebo TAPvs.
IIB+infiltrationLA
VASpainscoreatrestandin movementinthefirst24h
Randomizeddouble-blind trial
5
Appendectomy
Nirajetal.,200941 52 UnilateralTAPinopen appendectomy
TAPvs.noTAP Consumptionofopioidsin thefirst24h
Randomizeddouble-blind trial
J.
Ripollés
et
Table1(Continued)
Surgery
Author,year
N Intervention Comparison Outcome Design JadadScore
Nephrectomy
Hosgoodetal.,
201242
46 TAPindonornephrectomy TAPvs.placebo TAP
Consumptionofopioidsin thefirst48handVASpain score
Randomizeddouble-blind trial
5
Parikhetal., 201343
60 TAPindonornephrectomy TAPvs.placebo TAP
Consumptionofopioidsin thefirst24h
Randomizeddouble-blind trial
5
Bariatric
Sinhaetal.,201344 100 TAPinbariatricsurgery (laparoscopicY-Roux anastomosis)
TAPvs.placebo TAP
Consumptionofopioidsin thefirst24h
Randomizeddouble-blind trial
5
Albrechtetal., 201345
70 TAPinbariatricsurgerywith localinfiltrationLA
TAPvs.noTAP Consumptionofopioidsin thefirst24h
Randomizeddouble-blind trial
5
Gastrectomy
Wuetal.,201346 90 TAPinradicalgastrectomy TAPvs.epidural vs.nointervention
Consumptionofopioidsin thefirst24handVASpain score
Randomizeddouble-blind trial
5
Elkassabanyetal., 201347
52 BilateralTAPinretropubic radicalprostatectomy
TAPvs.placebo TAP
VASpainscoreand consumptionofopioidsin thefirst24h
Randomizeddouble-blind trial
5
of
ultrasound-guided
transverse
abdominal
plan
blockade
261
Table2 Analgesicefficacy.
Author,year N Groups(n) Painscore
---atrest
Painscore
---inmovement
Consumption
ofanalgesics
Opioid
rescuetime
Adverseeffects
relatedtoopioids
Conclusions
Early Late Early Late Early Late NVPO Itching Sedation
Nirajetal.,
201117
62 1--- TAPn27 2--- TAPn31
NA − NA NA Thereisnodifference
betweenVASscorein restandduring movementsinthe first72hwithTAPor epidural
Walteretal., 201318
68 1--- TAPn33 2--- NoTAPn 35
NA NA TAPreducesaround
33%themean consumptionof opioidsinthefirst 24h(20mg);p<0.05 Belavyetal.,
200919
57 1--- TAPn23 2--- placebo TAPn24
NA + − TAPreducesthe
meanconsumptionof opioidsinthefirst 24h(13.5mg); p<0.05 Costelloetal.,
200920
96 1---TAPn47 2---placebo TAPn49
ND No NA NA NA TAPdoesnotreduce
theVASscoreinthe first24h
Baajetal., 201021
40 1---TAPn20 2---placebo TAPn20
+ + + + NA NA + NA NA TAPreducesthe
meanconsumptionof opioidsinthefirst 24h(25.89mgvs. 62mg;p<0.05) Kanazietal.,
201022
57 1--- ITMn28 2---TAPn29
− − NA − + + TAPextendsaround
50%(TAP8h,MIT4h) thetimesincethe firstopioidrescue (p<0.05) Loaneetal.,
201223
66 1--- TAPn33 2
---ITM+placebo TAPn33
− − − − NA + + TAPincreasesthe
J.
Ripollés
et
Table2(Continued)
Author,year N Groups(n) Painscore
---atrest
Painscore
---inmovement
Consumption
ofanalgesics
Opioid
rescuetime
Adverseeffects
relatedtoopioids
Conclusions
Early Late Early Late Early Late NVPO Itching Sedation
Tanetal.,
201224
40 1---TAPn20 2---placebo TAPn20
NA NA TAPreducesthe
meanconsumptionof opioidsinthefirst 24h(12.3mgvs. 31.4mg;p<0.01) Bollagetal.,
201225
90 1---TAP placebon30 2---TAPn25 3---TAP clonidinen 26
− − + + NA NA NA NA Toaddclonidineto
TAPwithbupivacaine doesnotimprovethe injurieshyperalgesia rate,anditdoesnot improvetheVAS scoreatrestandin movement
Eslamianetal., 201226
50 1---TAPn23 2---NoTAPn 25
+ + + + + + NA NA NA TAPreducestheVAS
scoreatrestandin movement,aswellas theconsumptionof opioidsinthefirst 24h(50mgtramadol vs.150mgtramadol; p=0.0001)
Cánovasetal., 201327
90 1
---ITM+placebo TAPn30 2---placebo TAP 3---TAP
+ + + + + + + + + TAPreducestheVAS
scoreatrest,12/24h (p<0.05),andin movement(p≤0.02)
Leeetal., 201328
51 1---TAPn26 2---placebo TAPn25
+ + + + TAPreducesthepain
of
ultrasound-guided
transverse
abdominal
plan
blockade
263
Table2(Continued)
Author,year N Groups(n) Painscore
---atrest
Painscore
---inmovement
Consumption
ofanalgesics
Opioid
rescuetime
Adverseeffects
relatedtoopioids
Conclusions
Early Late Early Late Early Late NVPO Itching Sedation
El-Dawlatly etal.,200929
42 1--- TAPn21 2--- NoTAPn 21
NA NA NA NA + + NA NA NA NA TAPreducesthe
intraoperative consumptionof sufentanyl(p<0.01), andalsoreducesthe consumptionof morphineinthefirst 24h(12.3mg; p<0.05) Raetal.,
201030
54 1--- TAP0.5% n18 2--- TAP 0.25%n18 3---NoTAP
+ + + + + + NA NA NA + TAP0.25%andTAP
0.5%reduce
verbal-numericalpain scoreinthefirst24h (p<0.001).Thereare nodifferences betweenTAP0.25% andTAP0.5%.TAP reducesthe consumptionof intraoperative remifentanylandalso reducesthe
consumptionof analgesicsin postoperative (p<0.001).Thereare nodifferences betweenTAP0.25% andTAP0.5% Petersenetal.,
201231
80 1--- TAPn37 2--- placebo TAPn37
+ + + NA NA TAPreducestheVAS
painscorein movement,
J.
Ripollés
et
Table2(Continued)
Author,year N Groups(n) Painscore
---atrest
Painscore
---inmovement
Consumption
ofanalgesics
Opioid
rescuetime
Adverseeffects
relatedtoopioids
Conclusions
Early Late Early Late Early Late NVPO Itching Sedation
Ortizetal.,
201232
80 1---TAPn39 2---local infiltrationn 35
NA NA NA NA NA TAPdoesnotreduce
theVASscoreinthe first24h
Tolchardetal., 201233
43 1---TAPn21 2---local infiltrationn 22
+ NA + NA − NA NA NA NA TAPreducesVASin
thefirst8h(p<0.01) TAPreducesthe consumptionof opioidsinthefirst8h (9.2mgvs.16.8mg; p<0.01)
Griffithsetal., 201034
65 1---TAPn32 2---placebo TAPn33
NA TAPdoesnotreduce
theconsumptionof opioidsinthefirst 24h.TAPdoesnot reduceVASinthefirst 2postoperative hours.
Atimetal., 201135
55 1---TAPn18 2---placebo TAPn18 3---local infiltrationn 19
+ + + + + NA NA TAPandinfiltration
of
ultrasound-guided
transverse
abdominal
plan
blockade
265
Table2(Continued)
Author,year N Groups(n) Painscore
---atrest
Painscore
---inmovement
Consumption
ofanalgesics
Opioid
rescuetime
Adverseeffects
relatedtoopioids
Conclusions
Early Late Early Late Early Late NVPO Itching Sedation
DeOliveira
etal.,201136
75 1--- TAP 0.25%n23 2--- TAP0.5% n24 3--- placebo TAPn23
+ + + + + + NA NA NA NA TAPimprovesthe
QoR-40satisfaction score;averageof16 ropivacaine0.5%and 17ropivacaine0.25% vs.saline(p<0.05). Thereareno differencesbetween ropivacaine0.5%vs. ropivacaine0.25% Kaneetal.,
201237
56 1--- TAPn28 2--- NoTAPn 28
NA NA NA TAPdoesnotreduce theQoR-40scoreor VASscale.Itdoesnot reduceorincrease theconsumptionof opioids
Avelineetal., 201138
275 1---TAPn132 2---IHBn139
+ + + + NA NA NA NA TAPreducesthepain
scoreatearly (average11vs.15; p=0.04)andlate (average29vs.33; p=0.013)rest.TAP reducesthemean consumptionof opioidsinthefirst 24h;p=0.03 LópezGonzález
etal.,201339
41 1---TAPn20 2---local infiltrationn 21
+ + a Significant
J.
Ripollés
et
Table2(Continued)
Author,year N Groups(n) Painscore
---atrest
Painscore
---inmovement
Consumption
ofanalgesics
Opioid
rescuetime
Adverseeffects
relatedtoopioids
Conclusions
Early Late Early Late Early Late NVPO Itching Sedation
Petersenetal.,
201340
90 1---TAPn30 2--- Infiltra-tion/IIB30 3---placebo TAPn30
− − − TAPdoesnotreduce
thepainscoreatrest orinmovementin thefirst24h
Nirajetal., 200941
52 1---TAPn25 2---NoTAPn 26
+ + + + NA + NA NA TAPreducesthe
meanconsumptionof opioidsinthefirst 24h(28mgvs.50mg; p<0.002)
Hosgoodetal., 201242
51 1---TAPn25 2---placebo TAPn25
+ + + + + + + NA TAPreducesthe
meanconsumptionof opioidsinthefirst24 postoperativehours (12.4mgvs.21.6mg; p=0.015).Thereisno significantdifference inthecumulative consumptionof opioidsinthefirst 48h
Parikhetal., 201343
60 1---TAPn30 2---placebo TAPn30
+ + + + + NA TAPreducesthe
meanconsumptionof opioidsinthefirst 24h
(103.8±32.18mgvs. 235.8±47.5mg) Sinhaetal.,
201344
100 1---TAPn50 2---placebo TAPn50
+ + + + + + NA + TAPreducesthe
of
ultrasound-guided
transverse
abdominal
plan
blockade
267
Table2(Continued)
Author,year N Groups(n) Painscore
---atrest
Painscore
---inmovement
Consumption
ofanalgesics
Opioid
rescuetime
Adverseeffects
relatedtoopioids
Conclusions
Early Late Early Late Early Late NVPO Itching Sedation
Albrechtetal.,
201345
70 1--- TAPn25 2--- NoTAPn 28
Thereareno differencesbetween theconsumptionof opioidsTAPand controlinthefirst4 postoperativehours (32.2mgvs.35.6mg; p=0.41)
Wuetal., 201346
90 1--- TAPn29 2--- Epidural n27
3--- Controln 26
−/+ −/+ NA TAPisbetterthan
generalanesthesia regardingthe consumptionof opioidsinthefirst 24h.Epiduralis betterthanTAP regardingthe consumptionof opioidsinthefirst 24h
Elkassabany etal.,201347
52 1--- TAPn16 2--- placebo TAPn16
+ − + − + − + − NA NA TAPreducesthe
meanconsumptionof opioidsinthefirst 24h(22.1mgvs. 45.5mg,)
IHB,iliohypogastricblock;IIB,ilioinguinalblock;VAS,visualanalogscale;ITM,intrathecalmorphine;NA,notavailable;TAP,transverseabdominisplan;+,favorabletoTAP;−,favorable tocomparator.
J.
Ripollés
et
Author,year Typeof
block
Technique Time Needle Anesthetic
usedby
injection
Complications Sensitivelevel
oftheblock
Block duration
Additional analgesia
Conclusions
Nirajetal.,
201117
Bilateral Subcostal Postoperative 16G80mm 1mgkg−1 bupivacaine 0.375%
No No NA Paracetamol
1g Tramadol 50---100mg
Therearenodifferences betweenVASpainscore atrestorinmovement inthefirst72h,withTAP orepidural
Walteretal., 201318
Bilateral ND Preoperative ND 40ml. Levobupiva-caine 2mgkg−1 (maximum 150mg)
No No NA Paracetamol
1g
TAPreducesin33%the meanconsumptionof opioidsinthefirst24h (20mg),p<0.05
Belavyetal., 200919
Bilateral Mid-axillary Postoperative 20G150mm 20ml ropivacaine 0.5%
No No NA Paracetamol
1g Diclofenac 100mg
TAPreducesthemean consumptionofopioids inthefirst24h (13.5mg),p<0.05 Costelloetal.,
200920
Bilateral Mid-axillary Postoperative 20G64mm 20ml ropivacaine 0.375%
No No No Ketorolac
30mg Paracetamol 1.3grectal
TAPdoesnotreduceVAS scoreinthefirst24h
Baajetal., 201021
Bilateral Mid-axillary Preoperative 20G100mm 20ml bupivacaine 0.25%
No No NA No TAPreducesthemean
consumptionofopioids inthefirst24h, (25.89mgvs.62mg; p<0.05)
Kanazietal., 201022
Bilateral Mid-axillary Postoperative 21G100mm 20ml levobupiva-caine 0.375+ adrenaline
No No NA Paracetamol
1g Diclofenac 100mg
TAPextends50%(TAP 8h,MIT4h)ofthetime untilthefirstopioid rescue,p<0.05
Loaneetal., 201223
Bilateral Mid-axillary Postoperative 22G80mm Ropivacaine 1.5mgkg−1 maximum 20ml
No No NA Naproxen
500mg Paracetamol 1g
TAPincreasesthemean consumptionofopioids inthefirst24h,(7.5mg vs.2.7mg;p=0.03) Tanetal.,
201224
Bilateral Mid-axillary Postoperative 22G70mm 20ml levobupiva-caine 0.25%
No No NA Morphine
chloride 0.15mgkg−1
of
ultrasound-guided
transverse
abdominal
plan
blockade
269
Table3(Continued)
Author,year Typeof
block
Technique Time Needle Anesthetic
usedby
injection
Complications Sensitivelevel
oftheblock
Block duration
Additional analgesia
Conclusions
Bollagetal.,
201225
Bilateral Mid-axillary Postoperative 20G 20ml ropivacaine 0.375%
No No NA Paracetamol
1g Diclofenac 75mg Tramadol
ToaddclonidinetoTAP withbupivacainedoes notimprovethewound hyperalgesiarate,andit doesnotimprovethe VASscoreatrestandin movement
Eslamianetal., 201226
Bilateral Mid-axillary Postoperative 22G50mm 15ml bupivacaine 0.25%
No No NA Diclofenac
100mg
TAPreducestheVAS scoreatrestandin movement,aswellas theconsumptionof opioidsinthefirst24h (50mgtramadolvs. 150mgtramadol; p=0.0001) Cánovasetal.,
201327
Bilateral Mid-axillary Postoperative 20G 20ml levobupiva-caine 0.5%
No No NA Morphine
chloride
TAPreducesVASatrest, 12/24h(p<0.05),andin movement(p≤0.02)
Leeetal., 201328
Bilateral Mid-axillary Postoperative 21G90mm 20ml ropivacaine 0.5%
No No NA Paracetamol
1g Ketorolac 50mg Morphine chloride
TAPreducesthepain scoreatrestandin movementinthefirst2 postoperativehours(0.5 and1.9vs.2.8and4.9; p<0.001)
El-Dawlatly etal.,200929
Bilateral Mid-axillary Preoperative 21G90mm 15ml bupivacaine 0.5
No No NA NA TAPreducesthe
J.
Ripollés
et
Table3(Continued)
Author,year Typeof
block
Technique Time Needle Anesthetic
usedby
injection
Complications Sensitivelevel
oftheblock
Block duration
Additional analgesia
Conclusions
Raetal.,
201030
Bilateral Mid-axillary Preoperative 22G50mm 15ml bupivacaine 0.25%o 15ml bupivacaine 0.5%
No No NA Ketorolac
30mg Fentanyl
TAP0.25%andTAP0.5% reducethe
verbal-numericalpain scoreinthefirst24h (p<0.001).Thereareno differencesbetweenTAP 0.25%andTAP0.5%.TAP reducestheconsumption ofintraoperative remifentanylaswellas theuseofpostoperative analgesics(p<0.001). Therearenodifferences betweenTAP0.25%and TAP0.5%
L.Petersen etal.,201231
Bilateral Mid-axillary Preoperative 22G80mm 20ml ropivacaine 0.5%
No No 24h Paracetamol
1g Ibuprofen 600mg Morphine chloride
TAPreducestheVASpain scoremovement, calculatedasthearea underthecurveinthe first24h(26mmvs. 34mm;p=0.04) Ortizetal.,
201232
Bilateral Mid-axillary Preoperative 21G100mm 15ml bupivacaine 0>,5%
No No NA Ketorolac
30mg
TAPdoesnotreducethe VASscoreinthefirst24h
Tolchardetal., 201233
Bilateral Subcostal Preoperative 22G100mm Bupivacaine 1mgkg−1 (average 22ml)
No No NA Codeine TAPreducesVASinthe
first8h(p<0.01) TAPreducesthe consumptionofopioids inthefirst8h,(9.2mg vs.16.8mg;p<0.01) Griffithsetal.,
201034
Bilateral Mid-axillary Postoperative 90mm 20ml ropivacaine 0.5%
No No NA Paracetamol
1g, parecoxib 40mg
of
ultrasound-guided
transverse
abdominal
plan
blockade
271
Table3(Continued)
Author,year Typeof
block
Technique Time Needle Anesthetic
usedby
injection
Complications Sensitivelevel
oftheblock
Block duration
Additional analgesia
Conclusions
Atimetal.,
201135
Bilateral Medial armpit
Preoperative 20G100mm 20ml bupivacaine 0.25%
No No NA Diclofenac
75mg Tramadol 0.5mgkg−1
TAPandinfiltration reducethepainscoreat restandinmovementat thehours1,2,4,6,24 (p<0.0001).TAPreduces thepainscoreatrest andinmovementatthe hours6and24regarding theinfiltration
(p<0.001) DeOliveira
etal.,201136
Bilateral Mid-axillary Preoperative 21G90mm 15ml ropivacaine 0.25%o0.5%
No No NA Ketorolac
30mg
TAPimprovestheQoR-40 satisfactionscore; average16ropivacaine 0.5%and17ropivacaine 0.25%vs.saline; p<0.05.Thereareno differencesbetween ropivacaine0.5%vs. ropivacaine0.25% Kaneetal.,
201237
Bilateral NA Postoperative NA 20ml ropivacaine 0.5%+ adrenaline
No No NA NA TAPdoesnotreduce
QoR-40scoreorVAS score.Itdoesnotreduce orincreasethe
consumptionofopioids Avelineetal.,
201138
Unilateral Mid-axillary Preoperative 22G 1.5mgkg−1 levobupiva-caine 0.5%
No No NA Paracetamol
1g Ketoprofen 100mg
J.
Ripollés
et
Table3(Continued)
Author,year Typeof
block
Technique Time Needle Anesthetic
usedby
injection
Complications Sensitivelevel
oftheblock
Block duration
Additional analgesia
Conclusions
LópezGonzález
etal.,201339
Unilateral Mid-axillary Preoperative NA 30ml bupivacaine 0.25%
No No NA Paracetamol1g
Dexketoprofen 50mg
Morphinechloride
Significantdifferences werenotdetectedinVAS painscorebetweenat restandinmovement. TAPreducesthemean consumptionofopioids inthefirst24h(0.3mg vs.1.05mg;p<0.05) Petersenetal.,
201340
Unilateral Mid-axillary Preoperative 22G80mm 25ml ropivacaine 0.75%
No No NA Ketebidona TAPdoesnotreducethe painscaleatrestorin movementinthefirst 24h
Nirajetal., 200941
Unilateral Mid-axillary Postoperative 23G60mm 20ml ropivacaine 0.5%
No No NA Paracetamol1g
Diclofenac50mg
TAPreducesthemean consumptionofopioids inthefirst24h(28mg vs.50mg;p<0.002) Hosgoodetal.,
201242
Unilateral Mid-axillary Preoperative 22G 20ml ropivacaine 0.375%
No No NA Paracetamol1g
Morphinechloride
TAPreducesthemean consumptionofopioids inthefirst6
postoperativehours (12.4mgvs.21.6mg; p=0.015).Thereisno significantdifferencein thecumulative consumptionofopioids inthefirst48h Parikhetal.,
201343
Unilateral Mid-axillary Postoperative 18Gtohuy 25ml bupivacaine 0.375%
No No NA Diclofenac
1.5mgkg−1 Tramadol
TAPreducesthemean consumptionofopioids inthefirst24h (103.8±32.18mgvs. 235.8±47.5mg) Sinhaetal.,
201344
Bilateral Modified mid-axillary
Postoperative NA 20ml ropivacaine 0.375%
No No No NA TAPreducesthemean
of
ultrasound-guided
transverse
abdominal
plan
blockade
273
Table3(Continued)
Author,year Typeof
block
Technique Time Needle Anestheticusedby
injection
Complications Sensitivelevel
oftheblock
Block duration
Additional analgesia
Conclusions
Albrechtetal.,
201345
Bilateral Oblique subcostal
Preoperative 22G80mm 30mlbupivacaine 0.25%+adrenaline
No No No Paracetamol
1g Oxycodone 5---10mg
Therearenodifferences intheconsumptionof opioidsbetweenTAPand controlinthefirst24 postoperativehours (32.2mgvs.35.6mg; p=0.41)
Wuetal., 201346
Bilateral Oblique subcostal
Preoperative ND 20mlropivacaine 0.375%
No No No Morphine
chloride
TAPisbetterthan generalanesthesia regardingthe
consumptionofopioids inthefirst24h.Epidural isbetterthanTAP regardingthe
consumptionofopioids inthefirst24h Elkassabany
etal.,201347
Bilateral Mid-axillary Postoperative22G 20mlbupivacaine 0.5%
No No No Morphine
chloride
TAPreducesthemean consumptionofopioids inthefirst24h(22.1mg vs.45.5mg)
Transversus abdominal plane block TAP block
Citations in Pubmed 478
208 articles analyzed
270 articles excluded (no human, no English, no Spanish)
129 articles excluded (no RCT, randomized, blind) 56 RCT articles
for analysis
25 RCT included for systematic review Manual search 6
RCT included
31 RCT included for systematic review
26 articles excluded They do not fulfill the inclusion
criteria (adult, ecoguided, analgesic efficacy, Jadad > 2) Transversus abdominal plane block
Identification
Search
Elegibility
Included
Figure2 Flowdiagramoftheselectionofthearticlesincluded.
epidural.Inthe second RCT,18 apreoperative mid-axillary approach was performed and a reduction of 33% in the meanconsumptionofopioidswasobservedinthefirst24h (20mg)(p<0.05),mainlyduetotheinfraumbilicalsurgery, althoughtheconsumptionofopioidsinthefirst24hinthe supraumbilical-surgerysubgroup also decreased. Decrease ofPONV, sedation or itching wasobserved in noneof the cases.
The ultrasound-guided TAP in cesarean was evaluated in 10 RCTs. Among those, cesarean with spinal anesthe-sia was evaluated in 8 RCTs19---23,25,27; of which 420,22,23,27 comparedTAP vs. spinal morphine (ITM),2 comparedvs. placebo TAP,19,21 and in one the addition of clonidine in TAPvs. TAP vs. placebo TAP,26 andrecently the analgesic effectTAPincesareanwithspinalanesthesiawithITMwas evaluated.28
In 2 RCTs, TAP with cesarean was compared to gen-eralanesthesia.24,26 Inallcases,theblockwascarriedout afterthecesarean,throughbilateralmid-axillaryapproach;
thesensitive level neithertheduration oftheblock were altered.19---28
thegroupC,at12h1.9±1.1,andat24h2.3±1.2(p<0.05). Wheninmovement,theanalgesiawasbetterinthegroupC (p≤0.02).Thetimeuntiltheanalgesicrescuewasinferior inthe groupB:in thegroupA,9.3±4.9 (p=0.02in com-parisontothegroupC);inthegroupB,2±1.8(p<0.001in comparisontothegroupC);andinthegroupC,13.2±2.1h. Theconsumptionofopioidsinthefirst24hwas:inthegroup B38±5,inthegroupA,10±2(p<0.05),andinthegroup C,5±2(p<0.001).Theincidenceofnauseawassuperiorin thegroupB(36.6%),andtheitchingwasgreateringroupA (36.6%).
Bollagetal.25studiedtheeffectoftheadditionof cloni-dineandropivacaineintheexecutionoftheTAPinpatients undergoing cesarean under spinal anesthesia with ITM to measure wound hyperalgesia. There were no differences betweenITM,ITMwithTAPandITMwithTAPandclonidine. NodifferencesintheconsumptionofopioidsorinVASwere found.
In the RCTs that compared TAP vs. placebo TAP in cesareanwithspinalanesthesiawithoutITM,Belavyetal.19 foundadecreaseintheconsumptionofopioidsinthefirst 24h (18mg vs. 13.5mg; p<0.05) and in the timefor the firstopioidrescue(2h vs.3h;p=0.019). However,no sig-nificantdifferencesinVASatrestormovementwerefound, aswellasfortheincidenceofsecondaryeffectsofopioids. Baajetal.21demonstratedasignificantreductioninthe con-sumption of opioidsin the first 24h (25.89mg vs. 62mg; p>0.05), aswell asa lessening of 25% in theVAS at rest andinmovementforthefirst24h,andadecreaseinPONV. Theseresults,however,werenotsignificant.
Leeetal.28demonstratedthattheexecutionofbilateral TAPinpatientsscheduledtocesareanwithspinalanesthesia withITM lessens significantly the painscore at rest or in movementwithinthefirst2hafterthesurgery(0.5and1.9 vs.2.8and4.9;p<0.001).Italsodecreasestheconsumption of analgesics(0vs. 25%;p=0.01).However,nosignificant differences were found in reducing the painscore in the first24horinPONV.
IntheRCTthatcompareTAPvs.placeboTAPincesarean undergeneral anesthesia, Tanetal.24 concludedthat the TAPreducesthemeanconsumptionofopioidsinthefirst24h (12.3mg vs. 31.4mg; p<0.01). In addition, nosignificant differenceswerefoundintheVASatrestorinmovementor intheapparitionofsecondaryeffectsofopioids. Eslamian etal.26 demonstratedadecreaseintheVASatrest andin movement,areductionintheconsumptionofopioidsinthe first24h(50mgvs.250mg;p=0.001)andanincreaseforthe opioidrescue(210minvs.30min;p=0.0001);theincidence ofsecondaryeffectsofopioidswasnotevaluated.
The ultrasound-guided bilateral TAP in laparoscopic cholecystectomywasstudied in 5RCTs,29---33 amongwhose placebo wascompared within 3,29,30 andno intervention in one28; and in 2 of the RCTs to the LA infiltration in laparoscopicwounds.32,33 Inallthecases,itwasexecuted bilaterally and after the operation. In four cases,29,32 a mid-axillary approach was used, and in one, subcostal.33 In the RCT where TAP is comparedto placebo TAP or no intervention,29---31El-Dawlatlyetal.29comparedtheeffectof theTAPinlaparoscopiccholecystectomyvs.nointervention and demonstrated a lower consumption of intraoperative opioids(8.6mcg vs.23mcg;p<0.01),and of morphinein thefirst24h(10.5mgvs.22.8mg;p<0.05).NeitherVASnor
secondaryeffectsofopioidswereevaluated.Raetal.30 com-paredTAPwithbupivacaine0.25%vs.TAPwithbupivacaine 0.5%vs.placeboTAP,demonstratingthatTAP,atboth con-centrationsincomparisonwithplaceboreducedthenumeric verbalpainscoreinthefirst24h(p<0.001),regardlessthe bupivacainedosesof 0.25%and0.5%. Theconsumption of intraoperativeopioidsand analgesicsin thepostoperative periodwaslowerinthegroups withTAPwithbupivacaine (p<0.001),withnoinfluencefromdifferentLA concentra-tions used. The control group presented higher sedation scorein thepostoperative period in comparison withthe groupofTAPplusbupivacaine0.5%.Petersenetal.,31when comparingTAPvs.placeboTAPfoundareductionforVASin movement (calculatedasan areaunderthe curve)in the first24h (26mm vs. 34mm; p=0.04); aswell asa lower consumption of opioidsin the first 2 postoperative hours (7.5mgvs. 5mg; p<0.001).There werenodifferences in PONVor in sedation between the twogroups. In theRCT thatcompareTAPvs.LAinfiltrationinlaparoscopicwounds inthelaparoscopiccholecystectomy,31,32Ortizetal.32 per-formedamid-axillaryapproachanddidnotfinddifferences in the VAS, in the consumption of analgesics in the first 24h,andinPONV.However,recentlyTolchardetal.,33from asubcostalapproach,demonstratedthatthe TAPlowered the early VAS in movement (8h; p<0.01) as well as the consumptionofopioidsinthefirst8h(9.2mgvs.16.8mg; p<0.01).Thesecondaryeffectsofopioidswerenot evalu-ated.
terectomy.
The use of ultrasound-guided TAP in inguinal hernior-rhaphywithgeneral anesthesiawasstudiedin 3 RCT38---40; in the 3 it wasperformed in unilateral, mid-axillary, and preoperative. Aveline et al.38 compared TAP vs. ilioin-guinal/iliohypogastricblock demonstrating, withina large series of 275 patients, that the TAP decreased the pain scoreat early(average11 vs.15; p=0.04)andlate (aver-age29vs.33;p=0.013)rest,andthemeanconsumptionof opioidsinthefirst24h(p=0.03).RecentlyLópez-González etal.39comparedTAPvs.LAlocalinfiltrationfindingno sig-nificantdifferencesinVASpainscoreatrestorinmovement. Althoughthemeanconsumptionofopioidsdecreasedinthe first24h(0.3mgvs.1.05mg;p<0.05),evenwithoutclinical relevance,thedifferenceislowerandtherewereno differ-encesinthesecondaryeffectsofopioids.Petersenetal.40 comparetheuseofTAPvs.placeboTAPandvs.ilioinguinal blockattendedbyasurgeonfortheinfiltrationofsurgical wound,demonstratingthattheexecutionofTAPininguinal herniorrhaphybringsnobenefitstotheanalgesiaobtained fromparacetamolandibuprofen.
Nirajet al.41 demonstrated that theTAPs diminish the mean consumption of opioids in the first 24h (28mg vs. 50mg;p<0.002),theVASatrestorinmovementinthefirst 24handPONVwhenitiscomparedtointravenousanalgesia inpatients thatunderwentopen appendectomy,andhave notfoundcomplicationsassociatedwiththeTAP.41
Two RCTs compared TAP vs. placebo in donor nephrectomy.42,43 In bothRCTsa lowermeanconsumption ofopioidsinthefirst24h(12.4mgvs.21.6mg;p=0.015in the first6h42 and 103.8±32.18mg vs. 235.8±47.5mg in thefirst 24h)43 aswell as a lowerpostoperative VAS was demonstrated. In none there were differences in PONV, sedationoritching.
The ultrasound-guided TAP in laparoscopic bariatric surgerywasevaluatedin2RCTs.44,45 Sinhaetal.44 demon-strated theutility of bilateral TAP vs. placebo by usinga modification of the classical mid-axillary approach in the reduction of opioids consumption in the first 24h (8mg vs. 48mg; p=0.000), and in VAS at rest or movement in the first 24h, as well as all for the secondary effects of opioids. However,Albrecht et al.45, comparingTAP vs. no TAP in patients receiving LA infiltration, did not find anybenefits in theexecution of TAPby obliquesubcostal approach.
Wuetal.46comparedthepreoperativeobliquesubcostal bilateral TAP in radical gastrectomy to thoracic epidural andnointervention(generalanesthesia), findingthatTAP is superiorto thegeneral anesthesiafor the consumption ofopioidsinthefirst24h,butinferiortothoracicepidural inthisconsumption. TAPdidnotdiminish VASin compari-sontogeneralanesthesia, aswell astheepiduraldidnot diminishVASincomparisontotheTAP.Wuetal.46conclude thattheepiduralis superiortotheTAPinradical gastrec-tomy.
Recently, the bilateral mid-axillary TAP7 in retropu-bicradicalprostatectomy hasbeenused,demonstratinga diminutionin the consumption of opioidsin the first 24h (22.1mgvs.45.5mg;p<0.05),aswellasanincreaseinthe timeuntilthefirstopioidrescue(p=0.001)andalowerearly
Twenty-eightRCTswerefoundwheremid-axillaryapproach wascarriedout,18---44,47onesubcostal,17and2RCTsinwhich theobliquesubcostalapproachwasexecuted.44,46
The blockade was carried out preoperatively in 15,18,21,28---32,34,35,37,38,40,43,44 and postoperatively in 1617,19,20,22---27,34,37,40---43,47;obtainingfavorableresultsin11of the15RCTscarriedoutpreoperatively,18,21,29---31,33,35,36,38,39,42 and in 11 of the 16 RCTs in those carried out postoperatively.19,24---27,40---43,47 However, none of the RCTs compared the preoperative vs. postoperative TAP or differentapproachesforthesameintervention.
Drugs,volumeanddoses
SeveralLAsandtheirconcentrationswereusedinTAP: bupi-vacainein10(0.25%in421,30,35,39;0.375%in217,43;and5%in 426,29,30and1mgkg−1inone33)levobupivacainein5(0.25%in one24;0.375%inone22;0.5%in228,38and2mgkg−1inone)18; andropivacainein15(0.25%in236,45;0.375%in620,25,42---46; 0.5%in520,36,37,39---41;0.75%inone28;and1mgkg−1inone23). Adrenalinewasaddedin3,22,37,45andclonidineinone.25Only in 2 therewas a comparison for different concentrations ofLA.30,36Innoneofthemtheuseofdifferentvolumesor differentLAforthesameinterventionwerecompared.
Sensitivelevel,durationoftheblockand
complications
None oftheRCTsreviewedanalyzed thesensitivelevel of theblockoritsduration.Innoneofthecasescomplications werereported.17---47
Discussion
The execution of the ultrasound-guided TAP in colorec-tal surgery demonstratedits usefulnessfor surgerieswith infraumbilical incision by mid-axillary approach.18 Mean-while, in surgery with supraumbilical incision, despite reducingtheconsumptionofopioidsinthefirst24h,itdid notshowthesameperformancesignificantlybymid-axillary approach when compared to placebo,18 or by subcostal approachwhenitiscomparedtoepiduralanesthesia.17The epiduralanesthesiawillcontinuetobethe‘‘goldstandard’’ or technique of election for this intervention until more evidencewithTAPisavailable.
concen-ofthelevobupivacaine.IntheRCTscarriedoutbyCanovas etal.27complicationsrelatedtotheTAPwerenotreported, althoughitisimportanttorememberthatgestationbringsa highervascularizationthatincreasestherisktoreachtoxic concentrationsofLA,52andthepossibilityoftransferenceof theLAtothebreastmilkhastobetakenintoaccount.53,54
In case of cesarean withspinal anesthesiawithout ITM theexecutionoftheTAPdemonstratedupto60%of reduc-tionintheconsumptionofopioids.21 However,alowerVAS orPONV,itchingorsedationwasnotobtained,therebythe executionoftheTAPcouldbeindicatedforthosecasesof hypersensitivitytoopioid,historyofPONV,orpossibilityof transferenceofopiatetobreastmilk.55Incaseofcesarean withgeneralanesthesia,theexecutionofthebilateralTAP demonstratesreductionintheconsumptionofopioids24,26; althoughthereductioninVASisnotconclusive,itimproved inoneRCT,24andnodifferenceswerefoundinanother26;it equallyoccurswiththeapparitionof secondaryeffectsof opioids.IntheRCTexecutedbyTanetal.24levobupivacaine 0.25%wasused,andinthatcarriedoutbyEslamianetal.,26 bupivacaineat0.25%.
The execution of bilateral TAP is a valid alternative in patients undergoing cesarean without ITM, since it decreases theconsumptionof opioidsandtheirsecondary effects.Theseconclusionsarenotsimilartothoseobtained inrecentmeta-analysiswhereultrasound-guidedTAPisnot specified.52,56 However,in thosecesareansin whichspinal anesthesiawithITM iscarriedout,itdidnotdemonstrate tobebeneficial,40consideringthescarceclinicalrelevance of pain reduction only within the first 2 postoperative hours.
The execution of bilateral mid-axillary TAPfor laparo-scopic cholecystectomy demonstrated that it reduces the postoperative consumption of opioids,30,31 the intraoper-ative consumption of opioids30,31 and VAS30---33 when it is comparedtoplaceboTAPornointervention.However, com-pared with LA infiltration, it obtains just the decreasing of the consumption of opioids and VAS when a subcostal approachis performed.32,33 Ra etal.30 demonstrated that in the execution of TAP there are no differences with bupivacaine0.25% orbupivacaine 0.5%.The infiltrationof laparoscopic wounds aftercholecystectomy is an habitual practice, although it had good results with mid-axillary TAP when TAP vs. placebo TAP or no intervention are compared.29---31WhenitiscomparedtoLAinfiltration,results arenotobtained,32 sothattheexecutionofTAPmaybea validoptionincaseofimpossibilityoflocalLAinfiltration, orasawayofreducingtheconsumptionofintraoperative analgesics. Withthe subcostalapproach, theVAS and the consumption ofopioidsareimproved,33 sothat incase of executionofTAPincholecystectomy,thisapproachshould beelected. MoreRCTsarerequiredin ordertodetermine theoptimaldoseandvolumeinthisintervention.
The studiescarriedoutingynecologicalproceduresare very heterogeneous. The execution of preoperative mid-axillary TAP demonstrated to be useful and superior to the local LA infiltration in total abdominal hysterectomy withPfannenstielincision35andinoutpatientgynecological procedures,36despitenothavingdemonstratedtobe effec-tivein laparoscopic hysterectomy37 or in aheterogeneous groupofprocedureswithmid-laparotomy.34 Giventhe het-erogeneity ofthe RCTsin thegynecological interventions,
newRCTsareneeded,eventhoughithasbeendemonstrated tobeeffectiveintotalabdominalhysterectomy.35
The execution of TAP in inguinal herniorrhaphy is contradictory,38---40 since that, although Aveline et al.38 have demonstrated it was superior to the ilioin-guinal/iliohypogastricblockwhencomparedtoplacebo,no benefits in the diminution in the pain score are found.40 ThereisagradeofevidenceIA,recommendationAforthe executionofblocksof abdominalwall/localLAinfiltration foringuinalherniorrhaphy.57Duetothescarseclinical rele-vancethatitdemonstratedwhencomparedtothelocalLA infiltration,39,40currentlyitisnotpermittedtorecommend itsusefortheintervention,thelocalLAinfiltrationbeinga techniqueofchoice.
The mid-axillary TAP demonstrated to be useful when compared to placebo in patients undergoing laparo-scopic bariatric surgery where local LA infiltration is not executed44. However, it is not the same for patients whoreceive infiltrationoflaparoscopic wounds45 although promisingobliquesubcostalapproachisused8,14 thatcould beduetothepreincisionalexecutionofblockinafull-length intervention,ortothelackofbenefitfortheadditionofTAP tothelocalLAinfiltration.TheresultsoftheTAP,whenthey arecomparedtotheinfiltrationwithLA,arenotconclusive, demonstratingtobesuperiorinsomeRCTs33,35,39andnotin others32 andhavingsimilarresults tothoseof Albrecht et al45whenTAPvs.noTAPiscomparedinpatientsthatreceive localLAinfiltration.58
Theunilateralmid-axillaryTAPdemonstratedtoprovide appropriate analgesia in patients submitted to open appendectomy.40
Recently, Hosgood et al.42 and Parikh et al.43 demon-strated the efficacy of the mid-axillary TAP in donor nephrectomy.Wuetal.46 concludethattheepidural tech-niqueissuperiortoasingle-doseTAPviaobliquesubcostal in radical gastrectomy; however, probably the use of cathetersinTAPwouldimprovetheresults,asNirajetal.17 suggest and in studies carried out in renal and hepato-biliary surgery, not finding differences between TAP with catheterandepiduralanesthesia.TrialscarriedoutwithTAP attendedbysurgeon,in supraumbilicalcolorectalsurgery9 andultrasound-guided18,demonstrateditsefficacy sothat thedebateabouttheappropriateapproachforeach inter-ventionstillremains,andtheTAPcouldbeausefuloptionif itsefficacywasdemonstratedintheseinterventions,mainly those in programs of accelerated recovery where epidu-ralanesthesia,consideredasthe‘‘goldstandard’’forthis intervention,isavoided.17
Due tothe fact thatonly in retropubic radical prosta-tectomytheTAPwasevaluated,47despitethegoodresults obtained,moreRCTsareneededinordertoconfirmthese resultsandtheirclinicalbenefits.
Limitations
ThebibliographicresearchwaslimitedtoMEDLINE-Pubmed and to a manual driven one, aiming to comprise all the RCTspublished, sothat there maybe published RCTsnot evaluated.
approachesthattheultrasound-guidedtechniquepermits, althoughthemultipleRCTsexecutedwithattendedTAPor TAPbasedonreferencesshouldbeequallyconsideredbythe interesttothetechnique.
Conclusions
The execution of bilateral mid-axillary TAP is indicated in patients undergoing cesarean without ITM19---21,24---26; in cholecystectomybysubcostalTAP,33 or mid-axillarywhere theinfiltration is impossible, or as away of reducingthe consumption of postoperative opioids; in total abdomi-nal hysterectomy by bilateral mid-axillary TAP35; in open appendectomy by unilateral mid-axillary TAP40; in donor nephrectomy,mid-axillaryTAP.42,43However,thereare con-troversies in the use of oblique subcostal TAP in radical gastrectomy,17,46intheuseofbilateralmid-axillaryin colo-rectalsurgery18 andin retropubicradicalprostatectomy,47 becauseofthelimitationoftheRCTanalyzed.
It is not possible to recommend its use in inguinal herniorrhaphy.40
Thereisaconsiderabledebateaboutthebestapproach foreachtypeofintervention59sincethatdespitethe demon-strationof metamericextension describedby Lee etal.14 andCarneyetal.,15 thedatafoundinRCTarenot conclu-sive or concordant. New well-designed RCTs with enough statistical power tosolve the current questionsand their consequencesinthehabitualclinicalpracticearerequired. The lack of RCTsthat compare the pre- or postoperative execution of TAP in the same surgical intervention ren-dersit impossible torecommend the appropriatetime to theexecution ofthe block.In comparingTAP with differ-entconcentrations,30,36itwasdemonstratedthatthereare nobenefitsinusingahigherdose,andgiventhepotential toxiceffects of LAin the TAP and the possible overcom-ingoftheirtoxicdose,asdemonstratedbyGriffithsetal.60 withdosesofropivacainehabituallyused,itisnecessaryto studytheeffectiveminimumdosestodecreasethepossible deleteriouseffectsoftheLA.
The use of catheters in the abdominaltransverse plan couldincrease theanalgesicefficacy oftheblock,aswell astheuseofnewLA,liketherecentlyapprovedliposomal bupivacaine(EXPAREL), whichcouldincrease theduration oftheblock,althoughtherearenotrialsabout thesafety ofthisnewdruginperipheralblocks.Ultimately,inthe exe-cutionofnewRCTsitwouldbeconvenienttodeterminethe sensitiveleveloftheblock,aswellasitsdurationandthe plasmaticconcentrationsreachedwithdifferent concentra-tionsandvolumesofLA,inordertodeterminetheoptimal doseofLAforeachintervention.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Theauthorswouldliketoacknowledgethestaffofthe Pro-fessional Library of Hospital Universitario Infanta Leonor Madridfortheinestimablecollaboration.
1.RafiAN.Abdominalfieldblock:anewapproachviathelumbar triangle.Anaesthesia.2011;56:1024---6.
2.Hebbard P, Fujiwara Y, Shibata Y, et al. Ultrasound-guided transversus abdominis plane (TAP) block. Anaesth Intensive Care.2007;35:616---7.
3.Kearns RJ, Young SJ. Transversus abdominis plane blocks; a national survey of techniques used by UK obstetric anaes-thetists.IntJObstetAnesth.2011;20:103---4.
4.McDermott G, Korba E, Mata U, et al. Should we stop doingblindtransversusabdominisplaneblocks?BrJAnaesth. 2012;108:499---502.
5.JankovicZ,AhmadN,RavishankarN,etal.Transversus abdo-minis plane block: how safe is it? Anesth Analg. 2012;107: 1758---9.
6.Farooq M, Carey M. A case of liver trauma with a blunt regionalanesthesianeedlewhileperformingtransversus abdo-minisplaneblock.RegAnesthPainMed.2008;33:274---5.
7.BlancoR. TAPblockunderultrasoundguidance: the descrip-tionofa«nopopstrechnique».RegAnaesthPainMed.2007;32 Suppl.1:130.
8.Hebbard P. Subcostal transversus abdominis plane block underultrasoundguidance.AnesthAnalg.2008;106:674---7675. Réplica675.
9.BorglumJ,MaschmannC,BelhageB,etal.Ultrasound-guided bilateraldualtransversusabdominisplaneblock:anew four-pointapproach.ActaAnaesthesiolScand.2011;55:658---63.
10.NealJM,BrullR,Chan VWS,etal.TheASRAevidence-based medicineassessmentofultrasound-guidedregionalanesthesia andpainmedicine:executivesummary.RegAnesthPainMed. 2010;352Suppl.:S1---9.
11.AbrahamsMS,HornJ-L,NolesLM.Evidence-based medicine: ultrasoundguidancefortruncalblocks.RegAnesthPainMed. 2010;352Suppl.:S36---42.
12.McDonnellJG,O’DonnellBD,FarrellT,etal.Transversus abdo-minisplaneblock:acadavericandradiologicalevaluation.Reg AnesthPainMed.2007;32:399---404.
13.TranTMN,IvanusicJJ,HebbardP.Determinationofspreadof injectateafterultrasound-guidedtransversusabdominisplane block:acadavericstudy.BrJAnaesth.2009;102:123---7.
14.LeeTHW,BarringtonMJ,TranTMN. Comparisonofextentof sensoryblockfollowingposteriorandsubcostalapproachesto ultrasound-guidedtransversusabdominisplaneblock.Anaesth IntensiveCare.2010;38:452---60.
15.Carney J, Finnerty O, Rauf J, et al. Studies on the spread of localanaesthetic solution in transversus abdominis plane blocks.Anaesthesia.2011;66:1023---30.
16.McDonnellJG,FinnertyO,LaffeyJG.Stellateganglion block-ade for analgesiafollowing upperlimbsurgery. Anaesthesia. 2011;66:611---4.
17.NirajG,KelkarA,JeyapalanI,etal.Comparisonofanalgesic efficacyofsubcostaltransversusabdominisplaneblockswith epiduralanalgesiafollowingupperabdominalsurgery. Anaes-thesia.2011;66:465---71.
18.Walter CJ, Maxwell-Armstrong C, Pinkney TD, et al. A ran-domisedcontrolled trialof theefficacyofultrasound-guided transversusabdominisplane(TAP)blockinlaparoscopic colo-rectalsurgery.SurgEndosc.2013;27:2366---72.
19.BelavyD, Cowlishaw PJ,Howes M, et al. Ultrasound-guided transversusabdominisplaneblockforanalgesiaafterCaesarean delivery.BrJAnaesth.2009;103:726---30.