REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
Publicação Oficial da Sociedade Brasileira de Anestesiologia www.sba.com.brREVIEW
ARTICLE
Is
there
any
benefit
in
associating
neuraxial
anesthesia
to
general
anesthesia
for
coronary
artery
bypass
graft
surgery?
夽
Fabiano
Timbó
Barbosa
a,∗,
Célio
Fernando
de
Sousa
Rodrigues
b,
Aldemar
Araújo
Castro
b,
Rafael
Martins
da
Cunha
c,
Tatiana
Roa
Bezerra
Wanderley
Barbosa
daUniversidadeFederaldeAlagoas,Maceió,AL,Brazil
bUniversidadeEstadualdeCiênciasdaSaúdedeAlagoas,Maceió,AL,Brazil cCentrodeEnsinosSuperioresdeMaceió,Maceió,AL,Brazil
dCentroUniversitárioUnisebInterativo,Maceió,AL,Brazil
Received5July2013;accepted16September2013
Availableonline7March2015
KEYWORDS
Generalanesthesia; Subarachnoid anesthesia; Thoracicepidural anesthesia; Systematicreview; Mortality;
Evidence
Abstract
Backgroundandobjectives: Theuseofneuraxialanesthesiaincardiacsurgeryisrecent,but thehemodynamiceffectsoflocalanestheticsandanticoagulationcanresultinrisktopatients.
Objective:ToreviewthebenefitsofneuraxialanesthesiaincardiacsurgeryforCABGthrough asystematicreviewofsystematicreviews.
Content: ThesearchwasperformedinPubmed(January1966toDecember2012),Embase(1974
toDecember 2012),The Cochrane Library(volume10, 2012)andLilacs (1982to December
2012)databases,insearchofarticlesofsystematicreviews.Thefollowingvariables:mortality, myocardialinfarction,stroke,in-hospitallengthofstay,arrhythmiasandepiduralhematoma
wereanalyzed.
Conclusions:The use of neuraxialanesthesia in cardiacsurgeryremains controversial. The greatestbenefit found bythisreview wasthepossibility ofreducingpostoperative arrhyth-mias,butthisresultwascontradictoryamongtheidentifiedfindings.Theresultsoffindings regardingmortality,myocardialinfarction,strokeandin-hospitallengthofstaydidnotshow greaterefficacyofneuraxialanesthesia.
©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
夽 StudyconductedatUniversidadeFederaldeAlagoas,Maceió,AL,Brazil.
∗Correspondingauthor.
E-mail:[email protected](F.T.Barbosa).
http://dx.doi.org/10.1016/j.bjane.2013.09.015
PALAVRAS-CHAVE
Anestesiageral; Anestesia subaracnoidea; Anestesiaepidural torácica;
Revisãosistemática; Mortalidade; Evidências
Existealgumbenefícioemassociaraanestesianeuroaxialàanestesiageralpara revascularizac¸ãomiocárdica?
Resumo
Justificativaeobjetivos: Ousodaanestesianeuroaxialemcirurgiacardíacaérecente,porém osefeitos hemodinâmicosdos anestésicoslocais eaanticoagulac¸ãopodemtrazerriscosaos pacientes.
Objetivo: Revisar os benefícios da anestesia neuroaxial em cirurgia cardíaca para revascularizac¸ãomiocárdicapormeiodeumarevisãosistemáticaderevisõessistemáticas.
Conteúdo: FoifeitapesquisanasbasesdedadosPubmed(dejaneirode1966adezembrode 2012),Embase(1974adezembro2012),TheCochraneLibrary(volume10,2012)eLilacs(1982a dezembrode2012)embuscadeartigosderevisõessistemáticas.Foramanalisadasasseguintes variáveis:mortalidade,infartodomiocárdio,acidentevascularcerebral,tempodeinternac¸ão hospitalar,arritmiasehematomaperidural.
Conclusões: Ousodaanestesianeuroaxialpararevascularizac¸ãomiocárdicapermanece con-troverso.Omaiorbenefícioencontradopormeiodestarevisãofoiapossibilidadedereduc¸ão dasarritmiaspós-operatórias,porémesseresultadofoicontraditórioentreasevidências iden-tificadas.Osresultados das evidênciasencontradas referentes àmortalidade,ao infartodo miocárdio,aoacidentevascularcerebraleaotempodeinternac¸ãohospitalarnãomostraram maiorefetividadedaanestesianeuroaxial.
©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
The technologicaland pharmacological advances in anes-thesia and surgery over the past decades, as well as betterworkingconditionsinintensivecareunitsdecreased complicationsinpatientsundergoingcardiacsurgery.1,2
Neuraxial anesthesia (NA) causes sympathectomy and can improvethe coronaryperfusion andbalancebetween supply and demand of myocardial oxygen andreduce the incidence of postoperative arrhythmias and perioperative heartattack.3---5Thecombinationofgeneralanesthesia(GA) andNAmay bringbenefits topatientsundergoing cardiac surgery.3,4
Thesystematicuseofanticoagulationincardiacsurgery withcardiopulmonarybypassincreasestheriskofhematoma andspinalcordcompressionwhenanesthesiaisperformed onspinalcordornerves.6Themajorproblemwithneuraxial administration of local anesthetics is systemic hypoten-sion,whichmaybeaccompaniedbydecreasesincoronary blood flow, as the safe level of hypotension in patients undergoing cardiac surgery is not known.7 If we take into account the physiological effects of local anesthetic neuraxial administration and NA management in patients with anticoagulation, it is noticed that the use of NA, i.e., thoracic epidural anesthesia (TEA) and spinal anes-thesia (SA), in cardiac surgery remains controversial.6,7 It is necessary to analyze the existing data in the lit-erature to identify benefits of the NA administration in cardiac surgery for coronary artery bypass grafting (CABG).
The aim of this article wasto review the NA benefits incardiacsurgeryforCABGthroughasystematicreviewof systematicreviews.
Methods
Thestrategytoaccomplishthissystematicreviewfollowed the Cochrane Collaboration guidelines.8 This is a system-aticreviewofsystematicreviews.Theitemsforsystematic reviewspublicationsofPrismastatementwerefollowedto reporttheresultsofthisreview.9
Inclusion criteria were systematic review articles of randomizedcontrolled trials (RCTs) evaluating the use of neuraxialanesthesiaincardiacsurgeryforCABG.Therewas no language restriction. Other types of research articles wereexcludedfromtheanalysis.
The identification of systematic review articles was performed by searching in electronic databases. The sourcesused were: Medlinevia PubMed(January 1966 to December 2012), Embase (1974 to December 2012), The Cochrane Library (volume 10, 2012), and Lilacs (1982 to December 2012). The search strategy used for PubMed is shown in Table 1. The search strategy for Embase was: systematic review/exp and general anesthesia/exp or spinal anesthesia/exp or epidural anesthesia/exp and cardiacsurgery/expandembase/lim.‘Anesthesia’and ‘car-diac surgery’ terms were used for Lilacs and Cochrane Collaboration.
Thepublishedarticlesidentifiedbythesearchstrategy wereselectedbyanalysisoftitles andabstracts,or both. This selection wasindependently made by two reviewers (BarbosaF.T.andCastroA.A.)andfollowedbymeetingsto resolvedisagreementsbetweentheauthors.Thepublished systematic review articles that met the inclusion criteria werefullyreviewed.
Table1 SearchstrategyforMedlineviaPubmed.
Database Termsused
Pubmed systematic[sb]
and
thoracicsurgery[MeshTerms]or(thoracic [allfields]andsurgery[allfields])or
thoracicsurgery[allfields]or(cardiac[all fields]andsurgery[allfields])orcardiac surgery[allfields]orcardiacsurgical procedures[MeshTerms]or(cardiac[all fields]andsurgical[allfields]and
procedures[allfields])orcardiacsurgical procedures[allfields]or(cardiac[all fields]andsurgery[allfields])
and
generalanaesthesia[allfields]or
anesthesia,general[MeshTerms]or
(anesthesia[allfields]andgeneral[all fields])orgeneralanesthesia[allfields]or
(general[allfields]andanesthesia[all fields])
variablesofinterest.10Itisa10-itemquestionnaire,inwhich thefirstninequestionswereusedtoassessthesearch strat-egy, selection strategy, quality used in the review, data analysis performed, and outcomes. These questions were answeredwithyes,no,or partial/indeterminate.Thelast question focused on the systematic review overall scien-tificqualityconsists of a 7-point scale: 1---2 for extensive flaws,2---4formajorflaws,4---6forminorflaws,and6---7for minimalflaws.
Onlyonereviewerassessedthemethodologicalqualityof systematicreviews.Accordingtootherauthorsandto facil-itateinterpretationofOQAQscores,wegroupedthescores asfollows:1---2forextensiveflaws,3---4formajorflaws,5---6 forminorflaws,and7forminimalflaws.11,12Scores5---6were consideredassystematicreview ofacceptablequalityand ascoreof7asgoodquality.
The variables of interest to this systematic review were:mortality,myocardialinfarction,stroke,hospitalstay, arrhythmia,andepiduralhematoma.
This review was not submitted to the Ethics Research Committee because it is a secondary data analysis. The method used was a convenience sample. The agreement betweenreviewerswasassessedusingthekappastatistic.A qualitativeapproachwasusedtoevaluatethevariablesof interestdatareportedinthesystematicreviewsfound.
Results
The searchfor systematic reviewsthroughthe analysisof titlesandabstractsidentified1469articles:622inPubmed, 651 in Embase, 53 in Cochrane Collaboration, and 143 in Lilacs. We excluded 1463 articles for not meeting inclu-sion criteria. Two articles were excluded during the full textreviewfornotbeingsystematicreviews.Four system-aticreviewswereselectedforanalysisof thevariablesat theendof theprocess.13---16 The kappaconcordance index was0.75.
Table2showsthefrequencyofresponsestoOQAQ.After the methodological quality assessment, three systematic reviewswereclassifiedashavingminorflaws13,15,16andone ashavingminimalflaws.14
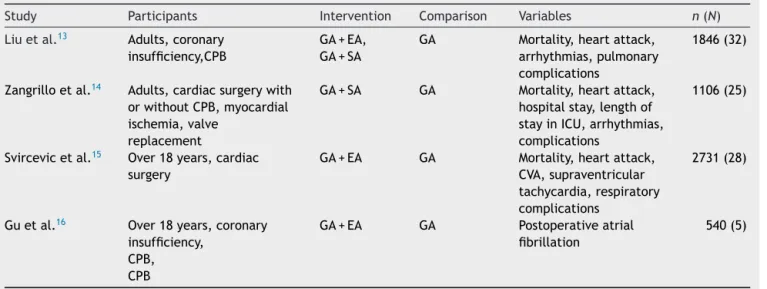
Table3showsthecharacteristics ofsystematicreviews includedforanalysisofvariables.Therewasplanningto ana-lyzetheepiduralhematomavariableinsystematicreviews, butthisvariablewasnotreportedintherandomizedclinical trialsincludedinthesereviews.
Mortalitywasassessed inthreesystematicreviews.Liu etal.13reportedthatoddsratiowas1.56(95%CI:0.35---6.91; p=0.56)forepiduralanesthesiaand0.88(95%CI:0.13---5.72; p=0.89) for spinal anesthesia. Zangrillo et al.14 reported thattheriskdifferenceforspinalanesthesiawas0.00(95% CI:−0.02to+0.02;p=1.0).Svircevicetal.15reportedthat relativeriskforepiduralanesthesiawas0.81(95%CI:0.40 to−1.64;pnotprovided).
Myocardialinfarction wasassessed in three systematic reviews.Liu etal.13 reportedthat oddsratiofor epidural anesthesiawas0.74(95%CI:0.34---1.59;p=0.44)and0.75 (95%CI:0.24---2.31;p=0.61)forspinalanesthesia.Zangrillo et al.14 reportedthat the risk differencefor spinal anes-thesiawas0.00(95%CI:−0.03to+0.02;p=0.77).Svircevic etal.15 reportedthatrelativerisk for epiduralanesthesia was0.80(95%CI:0.52to−1.24;pnotprovided).
Strokewaseassessedinonesystematicreview.Svircevic etal.15 reportedthatrelativerisk for epiduralanesthesia was0.59(95%CI:0.24to−1.46;pnotprovided).
Hospitalstaywasassessedinonesystematicreview. Zan-grilloet al.14 reportedthatweighted mean differencefor spinal anesthesiawas−0.28days(95% CI:−0.68 to0.13; p=0.18).
Arrhythmiawasassessedinthreesystematicreviews.Liu etal.13reportedthatoddsratioforepiduralanesthesiawas 0.52 (95% CI:0.29---0.93; p=0.03) favorableto the epidu-ralanesthesiagroup.Thesamebenefitwasnotobservedin studiesconsidering spinalanesthesiawithanoddsratioof 0.81(95%CI:0.42---1.53;p=0.51).Svircevicetal.15 demon-strated thatrelativerisk for epiduralanesthesiawas0.68 (95%CI:0.50to−0.93;pnotprovided).Guetal.16 demon-strated thatrelativerisk for epiduralanesthesiawas0.61 (95%CI:0.33---1.12;p=0.11).
Discussion
Inadequate pain control in patients undergoing cardiac surgery may increase morbidity due to adverse hemody-namiceffects,increasedmetabolicandimmuneresponseto trauma,andhemostaticabnormalities.17Aggressive postop-erativepainmanagementmayimproveclinicaloutcomesin highriskpatientsundergoingcardiacsurgery.18Althoughthe adverse effectsandthelikelihoodof prolongedintubation andmechanicalventilationofopioidsareknown,theuseof intravenousopioidsisatraditionalchoice.17Duringthelast decades,SAandTEAaregainingspaceinthisscenariofor providingadequateanalgesia,evenwiththeknowledgethat theseanesthetictechniquesarenotwithoutrisks.7
Table2 FrequencyoftheOQAQanswers.
Topicforanalysis Liuetal.13 Zangrilloetal.14 Svircevicetal.15 Guetal.16
1.Reportedsearchmethods No Yes Yes No
2.Comprehensivesearch Undetermined Yes Yes Undetermined
3.Inclusioncriteriareported Yes Yes Yes Yes
4.Avoidedselectionbias Undetermined Yes Yes Undetermined
5.Validitycriteriareported Undetermined Yes Undetermined Undetermined
6.Adequatelyassessedvalidity Undetermined Yes Undetermined Yes
7.Reportedcombinedmethods Yes Yes Yes Yes
8.Combiningresultsproperly Yes Yes Yes Yes
9.Conclusionssupportedbydata Yes Yes Yes Yes
sympatheticactivationisconsideredasacentralmechanism fortheemergenceofpostoperativemyocardialinfarction.19 The blockade of sympatheticfibers T1to T5 reduces the surgicalstress response,increasesthediameterof epicar-dial stenotic segments of coronary circulation, decreases myocardialoxygenconsumption, andimprovesleft ventri-cularfunction.17
SA can adequatelyreduce thesurgical stress response, but the hemodynamic changes, such as the emergence of systemic hypotension and bradycardia associated with other effects of total sympathectomy,may bring harmto patients undergoing CABG.17 Two double-blind, placebo-controlledRCTsattractedtheattention ofresearchersfor adequateanalgesiaachievedwiththeisolateduseof neu-raxial opioids.20,21 One of the RCTsreported that theuse ofmorphine0.5mgbeforeinductionofgeneralanesthesia canreducethetimeoftrachealintubationanddecreasethe durationofmechanicalventilation.20 Although this benefi-cialeffect may have occurred, it was not found in other studiesandwasconsideredcontroversial.21---23
TEAcanadequatelyreducethesurgical stressresponse andhemodynamicchanges,suchastheemergence of sys-temichypotensionandbradycardia,didnotseemtobring harm topatients undergoingmyocardial revascularization
withreportsintheliteratureofbeta-blockersdose reduc-tion in patients undergoing CABG.17 Three RCTs reported that postoperative analgesia is effective with this tech-nique;however, therewasdivergenceregardinganalgesia duration,which wasdifferent between thesestudies.24---26 ThecommonbenefitamongtheseRCTswasthereduced tra-chealintubationtimeanddecreasedmechanicalventilation time.
Systematicreviewsusetheavailable literaturedataby combiningresultsfromstudiesinordertoresolveconflicts inmedicalknowledge.12 Asystematicreview camimprove theanalysisstatisticalpower,whichcannotbeachievedin primaryisolatedstudiesandthus helptochoosethemost appropriateinterventionsforpopulationsofinterest.8Four systematicreviewsassessingtheuseofNAinpatients under-goingCABGwereidentified.13---16
Asystematicreviewpublishedin2004assessedtheuse ofepiduralanalgesia comparedwithintravenousopioid.13 The authors concluded that the use of NA is favorable, considering the time to tracheal extubation, postopera-tive pulmonary complications, and postoperative cardiac arrhythmias.Thatreviewexaminedstudies thatcombined resultsofpatientswhowereandwhowerenotundergoing cardiopulmonarybypass(CPB).Thesurgicalstresscannotbe
Table3 Characteristicsofsystematicreviewsincludedforanalysisofvariables.
Study Participants Intervention Comparison Variables n(N)
Liuetal.13 Adults,coronary
insufficiency,CPB
GA+EA,
GA+SA
GA Mortality,heartattack,
arrhythmias,pulmonary
complications
1846(32)
Zangrilloetal.14 Adults,cardiacsurgerywith
orwithoutCPB,myocardial
ischemia,valve
replacement
GA+SA GA Mortality,heartattack,
hospitalstay,lengthof
stayinICU,arrhythmias,
complications
1106(25)
Svircevicetal.15 Over18years,cardiac
surgery
GA+EA GA Mortality,heartattack,
CVA,supraventricular
tachycardia,respiratory
complications
2731(28)
Guetal.16 Over18years,coronary
insufficiency, CPB, CPB
GA+EA GA Postoperativeatrial
fibrillation
540(5)
n,numberofparticipants;N,numbersofincludedstudies;CPB,cardiopulmonarybypass;GA,generalanesthesia;EA,epiduralanesthesia;
thesameamongpatientswhounderwentCPBandthosewho werenotsubmittedtoCPBandthismayinfluencetheresults whencombinedinmeta-analysis.Therefore,itwouldhave beenmoreprudentiftheauthorshadanalyzed datafrom twotypesofpatientsseparately.Theanalysisregardingthe qualityofincludedstudieswasnotdescribed.Studieswith dubiousqualitymayhavebeenanalyzedtogetherwithgood qualitystudiesandaffectedmeta-analysisresults.
Asystematicreviewpublishedin2009assessedtheuse SA in cardiac surgery.14 The authors concluded that the useofNAis unfavorableconsidering mortality,myocardial infarction,and hospitalstay.That review evaluated stud-iesinthesettingofcardiacsurgeryandnotindividualized formyocardialrevascularization.Patientsundergoingheart valve surgery may have a different postoperative course thanthoseundergoingCABGandit isdifficult to individu-alizetheresults.
Asystematicreviewpublishedin2011assessedtheuseof epiduralanalgesiacomparedwithgeneralanesthesia.15The authorsconcludedthattheuseofNAisfavorableconsidering thereducedriskofpostoperativesupraventricular arrhyth-miasandrespiratorycomplications.Thatreviewevaluated studiesincardiacsurgerysettingandnotindividualizedfor myocardialrevascularization.Theauthorscreatedtheirown toolto assess the methodological quality of the included studiesanddidnotdescribetheprocessofvalidationofthis tool.Anon-validatedtoolmaynotaccuratelyreproducethe variableofinterest.Quality analysisoccurred foritemsof internalvalidityof randomizedcontrolledtrials;however, theanalysiscouldhavebeenmorecompleteiftheitemsof externalvalidityandstatisticaldatawerealsoevaluated.
The most recent systematic review was published in 2012 and assessed the use of TEA compared with gen-eralanesthesia,16 The authorsassessed only thepresence ofpostoperative atrial fibrillation andconcluded thatthe use of NA is not favorable. They reported the existence ofstatisticalheterogeneity,butdidnotidentifyitsorigin. Methodologicalqualityanalysiswasdone properly,butdid nothelp toidentify the heterogeneity source. The result ofmeta-analysiswithheterogeneityshouldbeviewedwith cautionandmay notevenbeconsidered; however, itcan guideauthorsoffutureresearchaboutthepresenceoffaulty pointstobeavoided.8
The implicationsfor clinicalpracticeafterthis system-atic review is that the results in the literature to date should be viewed with reservations and the anesthesiol-ogist should consider his clinical practice and the care offered by the health service in decision making regard-ing the patientundergoing cardiac surgery. The variables thatshowedpositiveresultsdidnotcontributetoimprove importantclinicaloutcomes,suchasmortality,myocardial infarction, stroke, hospital stay, and even the degree of patientsatisfaction.Theidentifiedsystematicreviewresults werecontradictory.
Theriskofneuraxialhematomawasestimatedby math-ematicalmethodsinastudyconductedin2000.27Maximum riskafter fullheparinizationwasestimated at 1:2400and neuraxialinstrumentationat1:1000.Someprecautionsare suggested, such as using neuraxial technique when there islaboratory indicationofnormalityfor coagulationtests, delayingprocedureswhenpunctureistraumatic,and wait-ingatleast60minafterNAtoperformfullheparinization.17
Themainclinicalimplicationforfutureresearchinthis clinical setting referstothe needfor newRCTswith ade-quatestatistical power andfocusingonimportantclinical variables,suchasmortality,myocardialinfarction,stroke, hospitalstay,arrhythmias,andepiduralhematoma.Sample size: 284participants areneeded in each group consider-ing1%mortalityinneuraxialanesthesiagroup,5%mortality ingeneral anesthesiagroup,80% statisticalpower, and5% significancelevel.
Conclusion
Theuseofneuraxialanesthesiaincardiacsurgeryremains controversial.Thegreatestbenefitfoundbythisreviewwas thepossibilityofreducingpostoperativearrhythmias; how-ever,thisbenefitwascontradictorybetweentheidentified outcomes.Theoutcomesfoundregardingmortality, myocar-dial infarction, stroke, and hospital stay were not more effectivethanneuraxialanesthesia.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.ManganoDT.Assessmentofthepatientwithcardiacdisease:an anesthesiologist’sparadigm.Anesthesiology.1999;91:1521---6.
2.CoriatP,BeaussierM.Fast-trackingaftercoronaryarterybypass graftsurgery.AnesthAnalg.2001;92:1081---3.
3.NygårdE,KofoedKF,FreibergJ,etal.Effectsofhighthoracic epiduralanalgesiaonmyocardialbloodflow inpatientswith ischemicheartdisease.Circulation.2005;111:2165---70.
4.BeattieWS,Badner NH,ChoiPT.Meta-analysisdemonstrates statisticallysignificantreduction inpostoperativemyocardial infarctionwiththeuseofthoracicepiduralanalgesia.Anesth Analg.2003;97:919---20.
5.LagunillaJ, Garcia-Bengochea JB,FernandezAL, etal. High thoracicepiduralblockadeincreasesmyocardialoxygen avail-abilityincoronarysurgerypatients.ActaAnaesthesiolScand. 2006;50:780---6.
6.HoAM,ChungDC,JoyntGM.Neuraxialblockadeandhematoma incardiacsurgery:estimatingtheriskofarareadverseevent thathasnot(yet)occurred.Chest.2000;117:551---5.
7.ChaneyMA.Intrathecalandepiduralanesthesiaandanalgesia forcardiacsurgery.AnesthAnalg.2006;102:45---64.
8.HigginsJPT,GreenS,editors.CochraneHandbookfor
System-atic Reviews of Interventions Version 5.1.0 [updated March
2011]. The Cochrane Collaboration; 2011. Available from:
www.cochrane-handbook.org[accessed12.01.13].
9.MoherD,LiberatiA,TetzlaffJ,etal.Preferredreportingitems for systematicreviews and meta-analyses:the Prisma state-ment.AnnInternMed.2009;151:264---9.
10.OxmanAD,GuyattGH.Validationofanindexofthequalityof reviewarticles.JClinEpidemiol.1991;44:1271---8.
11.KellyKD,TraversA,DorganM,SlaterL,RoweBH.Evaluating thequalityofsystematicreviewsintheemergencymedicine literature.AnnEmergMed.2001;38:518---26.
13.LiuSS,BlockBM,WuCL.Effectsofperioperativecentral neurax-ialanalgesiaonoutcomeaftercoronaryarterybypasssurgery: ameta-analysis.Anesthesiology.2004;101:153---61.
14.ZangrilloA,BignamiE,Biondi-ZoccaiGG,etal.Spinalanalgesia incardiacsurgery: ameta-analysis ofrandomizedcontrolled trials.CardiothoracVascAnesth.2009;23:813---21.
15.SvircevicV,vanDijkD,NierichAP,etal.Meta-analysisof tho-racicepiduralanesthesiaversusgeneralanesthesiaforcardiac surgery.Anesthesiology.2011;114:271---82.
16.GuWJ,WeiCY,HuangDQ,etal.Meta-analysisofrandomized controlledtrialsontheefficacyofthoracicepidural anesthe-siainpreventingatrialfibrillationaftercoronaryarterybypass grafting.BMCCardiovascDisord.2012;12:67.
17.ChaneyMA.Shouldthoracicepidural/spinalanalgesiabeused for CABG? In: Fleisher L, editor. Evidence-based practice of anesthesiology.2nded.Philadelphia:Saunders;2009.p.424---7.
18.ManganoDT, SilicianoD, Hollenberg M, et al. Postoperative myocardialischemia:therapeutictrialsusingintensive analge-siafollowingsurgery.Anesthesiology.1992;76:342---53.
19.LiuS, CarpenterRL, Neal MJ.Epiduralanesthesia and anal-gesia: their role in postoperative outcome. Anesthesiology. 1995;82:1474---506.
20.VanstrumGS, Bjornson KM, Ilko R. Postoperative effects of intrathecalmorphineincoronaryarterybypasssurgery.Anesth Analg.1988;67:261---7.
21.ChaneyMA,SmithKR,BarclayJC,etal.Large-dose intrathe-calmorphineforcoronaryarterybypassgrafting.AnesthAnalg. 1996;83:215---22.
22.ChaneyMA,FurryPA,FluderEM,etal.Intrathecalmorphinefor coronaryarterybypassgraftingand earlyextubation.Anesth Analg.1997;84:241---8.
23.Chaney MA, Nikolov MP, Blakeman BP, et al. Intrathe-cal morphine for coronary artery bypass graft procedure and early extubation revisited. J Cardiothorac Vasc Anesth. 1999;13:574---8.
24.PriestleyMC,CopeL,HalliwellR,etal.Thoracicepidural anes-thesiafor cardiacsurgery:theeffectsontrachealintubation timeandlengthofhospitalstay.AnesthAnalg.2002;94:275---82.
25.RoyseC,RoyseA,SoedingP,etal.Prospectiverandomizedtrial ofhighthoracicepiduralanalgesiaforcoronaryarterybypass surgery.AnnThoracSurg.2003;75:93---100.
26.Hansdottir V, Philip J, Olsen MF, et al. Thoracic epidural versus intravenous patient-controlled analgesiaaftercardiac surgery: a randomizedcontrolled trialon length of hospital stayandpatient-perceivedqualityofrecovery.Anesthesiology. 2006;104:142---51.