jcoloproctol(rioj).2015;35(4):212–216
w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Vermiform
appendix:
positions
and
length
–
a
study
of
377
cases
and
literature
review
Sandro
Cilindro
de
Souza
a,b,∗,
Sérgio
Ricardo
Matos
Rodrigues
da
Costa
c,d,
Iana
Gonc¸alves
Silva
de
Souza
baInstitutoMédico-LegaldeFeiradeSantana,SecretariadeSeguranc¸aPúblicadoEstadodaBahia,Salvador,BA,Brazil
bDepartmentofAnatomy,FaculdadesAdventistasdaBahia,Capoeiruc¸u,BA,Brazil
cInstitutoMédico-LegalNinaRodrigues,SecretariadeSeguranc¸aPúblicadoEstadodaBahia,Salvador,BA,Brazil
dCenterforHealthSciences,UniversidadeFederaldaBahia,Salvador,BA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received21June2015 Accepted15August2015
Availableonline25September2015
Keywords:
Vermiformappendix Cecum
Anatomicalvariation Appendicitis
a
b
s
t
r
a
c
t
Objective:Evaluation ofthefrequencyoftherelativepositionsandlengthofvermiform appendixinagroupofcorpsesexaminedbytheauthors.
Method:Dissectionof377adultcadaversautopsied.
Resultsandconclusions:Retrocecal: 43.5%; subcecal:24.4% post-ileal:14.3%, pelvic:9.3%; paracecal:5.8%;andpre-ilealappendices:2.4%,otherpositions:0.27%,meanlength:11.4cm. ©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Apêndice
vermiforme:
posic¸ões
e
comprimento
–
estudo
de
377
casos
e
revisão
de
literatura
Palavras-chave:
Apêndicevermiforme Ceco
Variac¸ãoanatômica Apendicite
r
e
s
u
m
o
Objetivo:Avaliac¸ãoda frequênciadas posic¸õesrelativasedocomprimentodoapêndice vermiformeemumgrupodecadáveresexaminadospelosautores.
Método:Dissecc¸ãode377cadáveresadultosnecropsiados.
Resultadose conclusões:Apêndices retrocecais:43,5%, subcecais:24,4%, pós-ileais:14,3%, pélvico:9,3%,paracecais:5,8%,pré-ileais2,4%,outrasposic¸ões:0,27%.Comprimentomédio: 11,4cm.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
∗ Correspondingauthor.
E-mail:[email protected](S.C.deSouza).
http://dx.doi.org/10.1016/j.jcol.2015.08.003
Introduction
Vermiform appendix (from the Latin appendix: “dan-gling”+“vermis”+‘form”,i.e.:“danglingworm-shapedthing”) isadiverticulumofthececumandmarksthebeginningofthe colonintheconfluenceoftaenias.Theappendixis posterior-mediallyattachedtothececum,about2cmbelowtheileocecal junction.1–6
Thepositionoftheappendixisextremelyvariable–more thananyotherorgan–andifitistoolong,theappendixmay extendtoanypartoftheabdomen.1,3,7,8 Thus,asstatedby Maingot,9theappendixistheonlyorganinthebodythathas nofixedanatomy.Althoughnowadaysthis traditional prin-cipleis being questioned, it has its value,by emphasizing thefactthat oftenthe appendixisoneofthemostmobile viscera,althoughits lackofnormalpositionisnotin him-self so extraordinary.10 Taking into account that often the appendixisamobilestructure,themedicalimportanceofits relativepositionhasbeenquestionedbysomeauthors.10In general,however, someauthors describea significant rela-tionship between its location and acute appendicitis.11,12 Signs and symptomsmay show varyingdegree of discrep-ancywiththeexpectedsymptomatology,dependingonthe positionoftheappendix.Forexample,apelvicappendicitis canreachthewalloftheureterandbladder,resultingin uri-narysymptoms.Ontheotherhand,aretrocecalappendicitis canpromote inflammationofthepsoas majormuscle and causelowbackpain,lamenessandpainwithhipextension.A peri-ilealappendicitis,inturn,cantriggeradiarrhealpicture indistinguishableofthatstemmedfromgastroenteritis. Occa-sionally,thepictureissoatypicalthatonecanmakeamistake with respect to a myriad of non-surgical intra-abdominal disorders11,13 and taking into account the great anatomi-calvariabilityofthe appendix,inthefaceofanepisodeof acuteabdominalpainthedoctormustregardappendicitisat leastas a second suspicion.11 In aretrocecal position, the bloodvesselsmaybecompressedandfoldedbythececum. Thus,whenaninflammationoftheappendixoccursinthis position,its blood supply may becompromised.8 Finally, a strongassociationhasbeenestablishedbetweenhidden loca-tionsoftheappendix(post-ileal,pelvic,retroperitoneal)and the developmentof anadvanced appendicitis, resulting in longerhospitalstaysandinhighincidenceofgangreneand perforation.2,14,15 The knowledge of all these nuances can facilitatetheestablishmentofadiagnosis,allowinganearly treatment and minimizing the rate of complications from appendicitis.Therefore,thestudyofappendixpositionshas provenuseful,eveninourdays.12
Theaimof this study isto determinethe position and lengthofthevermiformappendixinagroupofcorpses exam-inedbytheauthors.
Materials
and
methods
ThisstudywasconductedfromJuly5,2007toFebruary6,2014 inthe ForensicMedicineInstitutesofthecitiesofSalvador (NinaRodrigues)andFeiradeSantana(Bahia).
Inthisstudy,alladultcadaversexamineddirectlybythe authorsduringtheusualnecropsyevaluationswereincluded. Thestudyexcludedcorpseswithoneormoreofthe follow-ingconditions:agedunder18years,pregnancy(atnecropsy), scars or sutures of laparotomy, intra-abdominal infection (localizedordiffuse),partialorcompleteintestinal obstruc-tion, gaseous distension of bowel loops, and decomposing corpses.
Theabdomenwasopenedbyaxifopubicmidlineincision. Thevermiformappendixwaslocatedbysimpleexposureof the lowerileocecalrecess or,indifficultcases,wefollowed theteniaetotheirjunctionattheapexofthececumandbase oftheappendix.1,8,12Theappendixpositionsweredefinedas follows:1,8,12,16
• Retrocecal/retrocolic: the appendix courses upwardly
behindthececum,andmayreachtheinitialportionofthe ascendingcolon;
• Pelvic:theappendixisdirecteddownward,overthepsoas
major,withitstipsurpassingtheupperedgeofthelower pelvis.
• Post-ileal:thedistalportionoftheappendixisinaposition
posterior-superiortotheterminalileumanddirectedtothe spleen;
• Subcecal:theappendixislocatedunderthececum,resting
ontherightiliacfossaandseparatedfromtheiliacmuscle byalocalperitoneallining;
• Pre-ileal: the distalportion ofthe appendixislocatedin
a position anterior-superior to the terminal ileum and directedtothespleen;
• Paracecalposition:theappendixissituatedlaterallytothe
cecumandascendingcolon;
• Other(ectopic)positions:theappendixdoesnotfitinany
ofthepositionsabovedescribed.
Results
377appendiceswerestudied.Ofthewholegroupofcorpses, 87.8%(N=288)weremaleand12.2%(N=46),female.Theage rangedfrom18to89years(mean=33.6years).
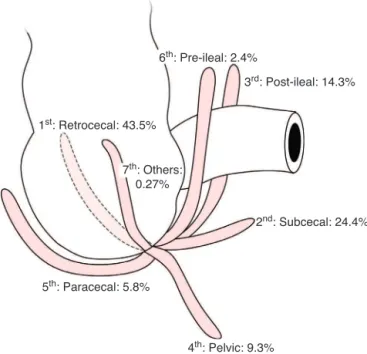
The corpses’ weight ranged from 46.5 to 90.5kg (mean=69.5kg). Their height ranged from 1.67 to 1.82m (mean=1.71m).Indescendingorder,thepositionsfoundfor theappendixwereasfollows(Fig.1):retrocecal:43.5%(164), subcecal: 24.4% (92), post-ileal: 14.3% (54), pelvic: 9.3%(35) paracecal: 5.8%(22), pre-ileal:2.4%(9), andother positions: 0.27%(1).
Mostretrocecalappendices(98.8%–162)wererestingfreely ontheretrocecalrecess.Inonlytwocases(1.2%),the mesoap-pendixwasabsentandtheappendixwascompletelyadhered totheposteriorwallofthececumorascendingcolon.
The appendix length ranged from 1.0 to 20.0cm (mean=11.4cm).
Discussion
214
jcoloproctol(rioj).2015;35(4):212–2164th: Pelvic: 9.3%
2nd: Subcecal: 24.4%
5th: Paracecal: 5.8%
3rd: Post-ileal: 14.3%
1st: Retrocecal: 43.5%
6th: Pre-ileal: 2.4%
7th: Others:
0.27%
Fig.1–Positionsofthevermiformappendix.
severalauthorshaverecordedhundredsofreferencesunder theirappropriatesubdivisions.Nousefulpurposehasbeen achievedbyrepeatingthishugeamountofdata.19Therefore, thereferencesreviewedinthecurrentstudywerepurposely limited,andaresummarizedinTable1.
Thelargest series documentedin the literature studied were 4680,19 10,0001 and40,00013 appendices. Inthe study byWakeley (10,000 cases),1 theappendix wasinretrocecal (65.28%),pelvic(31.01%),subcecal(2.26%),pre-ileal(1%)and post-ileal(0.4%)position.Subsequentanatomicaland surgi-calstudies in theliterature (11series until 1993) and data obtainedbyourgroup(Table1)showconsiderable contradic-tionwithrespecttothisclassicstudy.Probablytheauthors haveuseddifferentdefinitionsanddatacollection methodol-ogy,ordemographicvariationsoccurred.Thus,comparisons between reports may be challenging or even impossible, thankstolackofcriteria uniformity.Giventhese disagree-ments, currently we are not sure yet about the defined percentages.5,17 However,inmostreportsthe valuesofthe mostcommonpositions(retrocecalandpelvic)provide rea-sonableapproximations.12
Inthemostpart,therecordsarebasedonautopsy find-ings.Inthesestudies,thepositionmostcommonlyfoundhas beentheretrocecalone,withanoccurrencerangingfrom18 to65%ofspecimens.1,13–16,19,20Consistentwiththesefindings, inthisstudy,weobservedmoreoftenappendicesina retro-cecalposition(43.5%),andthisfindingwaswithintherange reportedbyotherresearchers(18–65%).Whenpreviousreports werereviewed,itwasfoundthattheretrocecalpositionhas beenlessfrequentinAfricanversusCaucasianpopulations.12 Thepositionoftheappendixiscloselyrelatedtothe devel-opment of the cecum. Although initially with its location underthe liver,afterthe 10thweekofintrauterinelifethe fetalintestine returnstotheabdominalcavity, causingthe cecumtograduallydescendintotherightiliacfossa,witha
counterclockwise twisting motion around its longitudinal axis. Simultaneously, the anterolateral wall of the cecum stretches and grows faster than the other parts, and this resultsindisplacementoftheappendixfromitsoriginal posi-tion attheapexofthececum,toananteromedialposition. Duringthisprocessofcecaldescent,theappendixcanbend behindthececum,andifatthattimethedevelopmentof perit-onealliningisoccurring,theappendixwillremainfixedinthis retrocecalposture.Ontheotherhand,iftheappendixremain freeanddirecteddownwardduringthedescentofthececum, thentheappendixwillremainpermanentlyasanorganwith freemobilityafteritsfixationtothecolon.1,2,10,15,16Inadults, theappendixmaybefixedinaretrocecalpositionbythe fibro-sisresultingfrompreviousepisodesofacuteappendicitis.14,15 Therefore,inviewoftheextrememobilityoftheappendix, andtakingintoaccountthefastandextensivechangesinthe surroundingparts,andalsoconsideringthepositionchanges sufferedbytheappendixwhenfollowingthececalmigration, itmaybeconcludedthattheappendixissubjecttomoreor lessintenseaccidentalcircumstancesthatwillmodifyitsfinal positioningandthatareresponsibleforthevariouspositions inwhichthis organisdescribed.1,17 Gender,age,body pos-turechanges,andvaryingdegreesofcecalcontractionhave not been described as determinantsof the positionof the appendix.12,17
Inthecurrentstudy,the2ndand3rdpositionsmost com-mon are the subcecal (24.4%) and post-ileal (14.3%) – an unexpectedresult,sinceinnoneofthereviewedstudiessuch a high frequencywasfound (Table 1). These findings were attributedtothelocalcharacteristicsofthestudypopulation, predominantly made up ofmestizos ofvarious ethnicities. Inthesubcecalposition,theappendixisinafully intraperi-tonealcondition.Ifinflamed,itcancausediffuseperitonitis. Thus, this position can beregarded as the most suscepti-bletocomplications.8Duringembryonicdevelopment,further growthoftherightwallofthececumorastrongertorsionof thececumandascendingcoloncanshiftthebaseofappendix towardtheileo-cecaljunctionarea,resultinginpre-ilealand, inextremecases,post-ilealappendices.1,10,17
Inthisseries,thepelvicpositionwasthefourthmost fre-quent(9.3%).However,inmostofthereviewedstudies(Table1) thepelvicpositionappearsinthesecondplace,andseveral authors describethis positionasthemostprevalent, espe-cially innon-surgical casesand inolderindividuals.12 The highfrequencyofpelvicappendiceshasbeenassociatedwith thepresenceoftheso-calledgenitomesentericfold,whichisa foldofperitoneumcoursingverticallyfromtheposteriorface ofthe terminalileumtothedeepright inguinal ringor,in women, tothe rightovary. Theappendix, asit follows the cecum andturns up and totheleft, mustcomeinto close proximitywiththisfold,andtendstobedeflecteddownward, towardthepelviccavity.1,5,17
j
coloproctol
(rio
j).
2
0
1
5;
3
5(4)
:212–216
215
Reference n Type Length(mean) Retrocecal Subcecal Pelvic Pre-ileal Post-ileal Paracecal Ectopic
Liertz,1909 (abstract)
2.092 – 35% 9% 42.1% 13.9% –
Collins,1932 4.680
Postmortem
8.21cm 20.21% 1.24% 7.9% Appendiceswithanteriorlocation:70.72% –
Wakeley,1933 10.000
–
65.28% 2.26% 31.01% 1.00% 0.4% – 0.05%
Peterson,1934 373 31% – 42.2% 26.8% –
Shah,1945 405 61.2% 3.7% 8.2% Paracecal,parailealandectopic:26.9%
186 30.1% 7% 34.9% Paracecal,parailealandectopic:28%
Waas,1959 266 35.3% 13% 24.1% Paracecal,parailealandectopic:28.6%
Bailey,1959 (abstract)
– Post-surgical 74% 1.5% 21% 1% 5% 2% –
Maisel,1960 300 Postmortem 26.7% 5% 58% 1.3% 3.3% –
Collins,1963 40.000 Post-surgical 25.95% Appendicesanteriortocecum:74.05% –
Solanke,1970 125 Postmortem 38.4% 11.2% 31.2% Paracecal,parailealandectopic:19.2%
Buschard,1973 141(Denmark) Post-surgical andpost mortem
9.91cm 56.7% 2.1% 33.4% 7.8% –
93(Czechoslovakia)
Postmortem 9.12cm 44.1% 0 44.1% 11.8% –
Katzarski,1979 103 12cm(♂)and11.4cm(♀) 20.3% – 43.6% –
Williamson, 1981
481 Post-surgical – 21.8% –
Ajmani,1983 100 Postmortem 9.5cm(♂)and8.7cm(♀) 58% 5% 23% 2% 10% 2% –
Grunditz,1983 247 Radiological – 17% –
Ojeifo,1989 548 Post-surgical
andpost mortem
216
jcoloproctol(rioj).2015;35(4):212–216Agenesisofthe appendix, double appendixand ectopic appendixhavebeenreportedatafrequencyunder1%.12,15The authorsfoundonlyanectopicappendix(0.27%)inapre-cecal position.
Theauthorsfoundnocorrelationbetweenappendixlength andposition.Thiscorrelationhasalsonotbeenestablishedby otherresearchers.8,17,20
Conclusions
Inthepresentstudy,weobtainedthefollowingfrequenciesfor appendixpositions:retrocecal:43.5%,subcecal:24.4%, post-ileal:14.3%,pelvic:9.3%,paracecal:5.8%,pre-ileal:2.4%,other positions:0.27%.Thelengthrangedfrom1.0to20cm,witha meanof11.4cm.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. WakeleyCPG.Thepositionofthevermiformappendixas ascertainedbyanalysisof10,000cases.JAnat.1933;67:277–83.
2. ZernJT.Theapêndix:little,bigtrouble.DelMedJrl. 1995;67:326–34.
3. EllisH.Clinicalanatomy:arevisionandappliedanatomyfor clinicalstudents.9thed.Oxford:BlackwellScience;1997.
4. VolgAW,MitchelAWM.Gray’sanatomyforstudents.2nded. Philadelphia:Elsevier;2010.
5. GrayH.Gray’sanatomy.37thed.London:Churchill Livingstone;1989.
6.MonkhouseS.Mastermedicine:clinicalanatomy.Kidlington: Elsevier;2001.
7.TrevesF.Lecturesontheanatomyofthecanalintestinaland peritoneuminman.BritMedJ.1835;1:527–30.
8.AjmaniML,AjmaniK.Thepositionandarterialsupplyof vermiformappendix.AnatAnz.1983;153:369–74.
9.MaingotR.Postgraduatesurgery,vol.1.D.AppletonCentury Co.;1938.
10.DeGarisCF.Topographyanddevelopmentofthececusand appendix.AnnSurg.1941;113:540–8.
11.CourtneyMT,etal.Sabiston:tratadodecirurgia.17thed.Rio deJaneiro:Elsevier;2005.
12.OjeifoJO,EjiwunmiAB,IklakiJ.Thepositionofthevermiform appendixinNigerianswithareviewoftheliterature.West AfrJMed.1989;8:198–204.
13.CollinsDC.71,000humanappendixspecimens:afinalreport summarizingfortyyears’study.AmJProctol.1963;14: 365–81.
14.CollinsDC.Acuteretrocecalappendicitis.ArchSurg. 1938;36:729–43.
15.WilliamsonWA,BushRD,WilliamsLF.Retrocecal appendicitis.AmJSurg.1981;141:507–9.
16.MaiselH.Thepositionofthehumanvermiformappendixin fetalandadultagegroups.AnatRec.1960;136:385–91.
17.BuschardK,KjaeldgaardA.Investigationandanalysisofthe position,fixation,lengthandembryologyofthevermiform appendix.ActaChirScan.1973;139:293–8.
18.KarimOM,BoothroydAE,WyllieJH.McBurney’spoint–fact orfiction.AnnRCollSurgEngl.1990;72:304–8.
19.CollinsDC.Thelengthandpositionsofthevermiform appendix–astudyof4,680specimens.AnnSurg. 1932;96:1044–8.
20.GrunditzT,RydénCY,JanzonLars.Doestheretrocecal positioninfluencethecourseofacuteappendicitis.ActaChir Scand.1983;149:707–10.